I’ve been sick. When can I start exercising again?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You’ve had a cold or the flu and your symptoms have begun to subside. Your nose has stopped dripping, your cough is clearing and your head and muscles no longer ache.
You’re ready to get off the couch. But is it too early to go for a run? Here’s what to consider when getting back to exercising after illness.

Exercise can boost your immune system – but not always
Exercise reduces the chance of getting respiratory infections by increasing your immune function and the ability to fight off viruses.
However, an acute bout of endurance exercise may temporarily increase your susceptibility to upper respiratory infections, such as colds and the flu, via the short-term suppression of your immune system. This is known as the “open window” theory.
A study from 2010 examined changes in trained cyclists’ immune systems up to eight hours after two-hour high-intensity cycling. It found important immune functions were suppressed, resulting in an increased rate of upper respiratory infections after the intense endurance exercise.
So, we have to be more careful after performing harder exercises than normal.
Can you exercise when you’re sick?
This depends on the severity of your symptoms and the intensity of exercise.
Mild to moderate exercise (reducing the intensity and length of workout) may be OK if your symptoms are a runny nose, nasal congestion, sneezing and minor sore throat, without a fever.
Exercise may help you feel better by opening your nasal passages and temporarily relieving nasal congestion.

However, if you try to exercise at your normal intensity when you are sick, you risk injury or more serious illness. So it’s important to listen to your body.
If your symptoms include chest congestion, a cough, upset stomach, fever, fatigue or widespread muscle aches, avoid exercising. Exercising when you have these symptoms may worsen the symptoms and prolong the recovery time.
If you’ve had the flu or another respiratory illness that caused a high fever, make sure your temperature is back to normal before getting back to exercise. Exercising raises your body temperature, so if you already have a fever, your temperature will become high quicker, which makes you sicker.
If you have COVID or other contagious illnesses, stay at home, rest and isolate yourself from others.
When you’re sick and feel weak, don’t force yourself to exercise. Focus instead on getting plenty of rest. This may actually shorten the time it takes to recover and resume your normal workout routine.
I’ve been sick for a few weeks. What has happened to my strength and fitness?
You may think taking two weeks off from training is disastrous, and worry you’ll lose the gains you’ve made in your previous workouts. But it could be just what the body needs.
It’s true that almost all training benefits are reversible to some degree. This means the physical fitness that you have built up over time can be lost without regular exercise.
To study the effects of de-training on our body functions, researchers have undertaken “bed rest” studies, where healthy volunteers spend up to 70 days in bed. They found that V̇O₂max (the maximum amount of oxygen a person can use during maximal exercise, which is a measure of aerobic fitness) declines 0.3–0.4% a day. And the higher pre-bed-rest V̇O₂max levels, the larger the declines.
In terms of skeletal muscles, upper thigh muscles become smaller by 2% after five days of bed rest, 5% at 14 days, and 12% at 35 days of bed rest.
Muscle strength declines more than muscle mass: knee extensor muscle strength gets weaker by 8% at five days, 12% at 14 days and more than 20% after around 35 days of bed rest.
This is why it feels harder to do the same exercises after resting for even five days.

But in bed rest studies, physical activities are strictly limited, and even standing up from a bed is prohibited during the whole length of a study. When we’re sick in bed, we have some physical activities such as sitting on a bed, standing up and walking to the toilet. These activities could reduce the rate of decreases in our physical functions compared with study participants.
How to ease back into exercise
Start with a lower-intensity workout initially, such as going for a walk instead of a run. Your first workout back should be light so you don’t get out of breath. Go low (intensity) and go slow.
Gradually increase the volume and intensity to the previous level. It may take the same number of days or weeks you rested to get back to where you were. If you were absent from an exercise routine for two weeks, for example, it may require two weeks for your fitness to return to the same level.
If you feel exhausted after exercising, take an extra day off before working out again. A day or two off from exercising shouldn’t affect your performance very much.
Ken Nosaka, Professor of Exercise and Sports Science, Edith Cowan University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Behind Book Recommendations

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day!
Each Thursday, we respond to subscriber questions and requests! If it’s something small, we’ll answer it directly; if it’s something bigger, we’ll do a main feature in a follow-up day instead!
So, no question/request to big or small; they’ll just get sorted accordingly
Remember, you can always hit reply to any of our emails, or use the handy feedback widget at the bottom. We always look forward to hearing from you!
Q: What’s the process behind the books you recommend? You seem to have a limitless stream of recommendations
We do our best!
The books we recommend are books that…
- are on Amazon—it makes things tidy, consistent, and accessible. And if you end up buying one of the books, we get a small affiliate commission*.
- we have read—we would say “obviously”, but you might be surprised how many people write about books without having read them.
- pertain in at least large part to health and/or productivity.
- are written by humans—bookish people (and especially Kindle Unlimited users) may have noticed lately that there are a lot of low quality AI-written books flooding the market, sometimes with paid 5-star reviews to bolster them. It’s frustrating, but we can tell the difference and screen those out.
- are of a certain level of quality. They don’t have to be “top 5 desert-island books”, because well, there’s one every day and the days keep coming. But they do have to genuinely deliver the value that we describe, and merit a sincere recommendation.
- are varied—we try to not give a run of “samey” books one after another. We will sometimes review a book that covers a topic another previously-reviewed book did, but it must have something about it that makes it different. It may be a different angle or a different writing style, but it needs something to set it apart.
*this is from Amazon and isn’t product-specific, so this is not affecting our choice of what books to review at all—just that they will be books that are available on Amazon.
Share This Post
-

Just One Thing – by Dr. Michael Mosley
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a collection of easy-to-implement changes that have good science behind them to show how they can benefit us. Some things are obvious (e.g: drink water); others, less so (e.g: sing, to reduce inflammation).
The book is divided thematically into times of the day, though in many cases it’s not a hard rule that a thing needs to be done at a certain time. Others are, like a cold shower in the morning and hot bath before bed—you might not want to switch those around!
The style is very pop-science, and does not have in-line citations for claims, but it does have a bibliography in the bag organized by each “one thing”, e.g. it might say “get some houseplants” and then list a number of references supporting that, with links to the studies showing how that helps. For those with the paper version, don’t worry, you can copy the URL from the book into your browser and see it that way. In any case, there are 2–6 scientific references for each claim, which is very respectable for a pop-sci book.
Bottom line: if you’re looking for evidence-based “one little thing” changes that can make a big difference, this book has lots!
Click here to check out Just One Thing, and improve your life!
Share This Post
-

Your Health Audit, From Head To Toe
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Health Audit Time
Here at 10almonds, we often cover quite specific things, ranging from “the effect of sodium on organs other than your heart” to “make this one small change to save your knees while driving”.
But, we’re each a whole person, and we need to take care of the whole organism that makes up the wonderful being that we each are. If we let one part of it drop in health too much, the others will soon follow suit because of the knock-on effects.
So, let’s do a quick self-check-up, and see what can be done for each! How’s your…
Mental Health
We’re doing this audit head-to-to, so let’s start it here, because mental health is also just health, and it’s difficult to tackle the others without having this one at least under control!
Are you experiencing chronic stress? Anxiety? Depression? Joy?
If you answered “no” to “joy” but also “no” to “depression”, you might want to rethink your answer to “depression”, by the way. Life should be a joyous thing!
Some resources to address your mental health:
Brain Health
Your brain is a big, powerful organ. It uses more of your daily energy (in the physiological sense of the word, we’re talking calories and mitochondria and ATP) than any other organ, by far.
And when it comes to organ failure, if your brain fails, then having the best joints in the world won’t help you, for example.
Some resources to address your brain health:
- Brain Food? The Eyes Have It
- How To Reduce Your Alzheimer’s Risk
- The 6 Dimensions Of Sleep (And Why They Matter)
Heart Health
Everything depends on your heart, head to toe. Tirelessly pumping blood with oxygen, nutrients, and agents of your immune system all around your body, all day every day for your entire life.
What’s your resting heart rate like? How about your blood pressure? And while we’re on the topic of blood… how’s your blood sugar health?
These are all important things to a) know about and b) keep on top of!
Some resources to address your heart health:
- 1-Minute Heart Health Check-Up Tips
- A Five-Point Plan For Heart Health
- High Blood Pressure? Try These!
Gut Health
By cell count, we’re about 10% human and 90% bacteria. By gene count, also. Pretty important, therefore, that we look after our trillions of tiny friends that keep our organism working.
Most people in N. America, for example, get vastly under the recommended daily amount of fiber, and that’s just the most basic courtesy we could do for these bugs that keep us alive (they need that fiber to live, and their process of consuming it is beneficial to us in a stack of ways).
Some resources to address your gut health:
- Making Friends With Your Gut (You Can Thank Us Later)
- The Surprising Link Between Gut Health And Serotonin
- The Vagus Nerve: The Brain-Gut Highway!
Hormonal Health
Hormones are weird and wonderful and affect so much more than the obvious sex-related functions (but yes, those too). A lot of people don’t realize it, but having our hormones in good order or not can make the difference between abject misery and a happy, fulfilling life.
Some resources to address your hormonal health:
- What Does “Balance Your Hormones” Even Mean?
- Healthy Hormones And How To Hack Them
- Too Much Or Too Little Testosterone?
Bone/Joint Health
Fear nothing! For you are a ghost operating a skeleton clad in flesh. But also, you know, look after that skeleton; you only get one! Being animals, we’re all about movement, and being humans, we’ve ended up with some lifestyle situations that aren’t great for that mobility. We sit too much; we walk too little; we cramp ourselves into weird positions (driving, anyone?), and we forget the range of motion we’re supposed to have. But let’s remember…
Some resources to address your bone/joint health:
- Collagen’s benefits are more than skin deep
- Cool As A Cucumber (Move Over, Glucosamine + Chondroitin)
- 5 Best Bodyweight Exercises For Incredible Mobility
Lastly…
While it’s good to do a little self-audit like this every now and again, it’s even better to get a professional check-up!
As engineers say: if you don’t schedule time for maintenance, your equipment will schedule it for you.
Share This Post
-

Gluten: What’s The Truth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
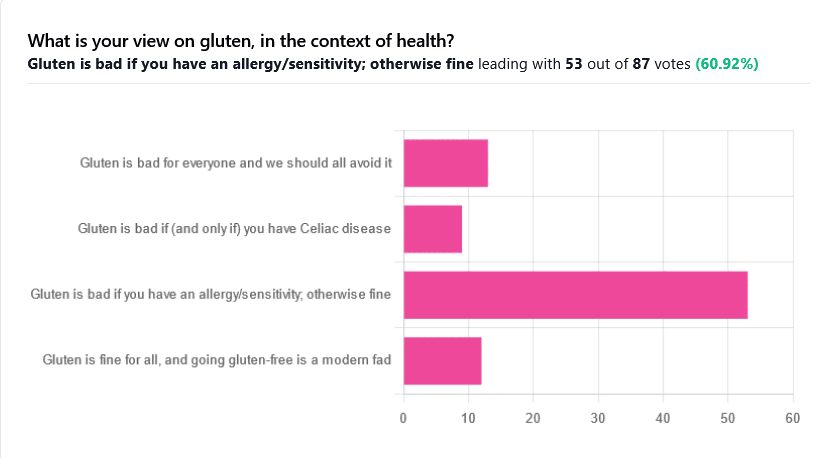
Gluten: What’s The Truth?

We asked you for your health-related view of gluten, and got the above spread of results. To put it simply:
Around 60% of voters voted for “Gluten is bad if you have an allergy/sensitivity; otherwise fine”
The rest of the votes were split fairly evenly between the other three options:
- Gluten is bad for everyone and we should avoid it
- Gluten is bad if (and only if) you have Celiac disease
- Gluten is fine for all, and going gluten-free is a modern fad
First, let’s define some terms so that we’re all on the same page:
What is gluten?
Gluten is a category of protein found in wheat, barley, rye, and triticale. As such, it’s not one single compound, but a little umbrella of similar compounds. However, for the sake of not making this article many times longer, we’re going to refer to “gluten” without further specification.
What is Celiac disease?
Celiac disease is an autoimmune disease. Like many autoimmune diseases, we don’t know for sure how/why it occurs, but a combination of genetic and environmental factors have been strongly implicated, with the latter putatively including overexposure to gluten.
It affects about 1% of the world’s population, and people with Celiac disease will tend to respond adversely to gluten, notably by inflammation of the small intestine and destruction of enterocytes (the cells that line the wall of the small intestine). This in turn causes all sorts of other problems, beyond the scope of today’s main feature, but suffice it to say, it’s not pleasant.
What is an allergy/intolerance/sensitivity?
This may seem basic, but a lot of people conflate allergy/intolerance/sensitivity, so:
- An allergy is when the body mistakes a harmless substance for something harmful, and responds inappropriately. This can be mild (e.g. allergic rhinitis, hayfever) or severe (e.g. peanut allergy), and as such, responses can vary from “sniffly nose” to “anaphylactic shock and death”.
- In the case of a wheat allergy (for example), this is usually somewhere between the two, and can for example cause breathing problems after ingesting wheat or inhaling wheat flour.
- An intolerance is when the body fails to correctly process something it should be able to process, and just ejects it half-processed instead.
- A common and easily demonstrable example is lactose intolerance. There isn’t a well-defined analog for gluten, but gluten intolerance is nonetheless a well-reported thing.
- A sensitivity is when none of the above apply, but the body nevertheless experiences unpleasant symptoms after exposure to a substance that should normally be safe.
- In the case of gluten, this is referred to as non-Celiac gluten sensitivity
A word on scientific objectivity: at 10almonds we try to report science as objectively as possible. Sometimes people have strong feelings on a topic, especially if it is polarizing.
Sometimes people with a certain condition feel constantly disbelieved and mocked; sometimes people without a certain condition think others are imagining problems for themselves where there are none.
We can’t diagnose anyone or validate either side of that, but what we can do is report the facts as objectively as science can lay them out.
Gluten is fine for all, and going gluten-free is a modern fad: True or False?
Definitely False, Celiac disease is a real autoimmune disease that cannot be faked, and allergies are also a real thing that people can have, and again can be validated in studies. Even intolerances have scientifically measurable symptoms and can be tested against nocebo.
See for example:
- Epidemiology and clinical presentations of Celiac disease
- Severe forms of food allergy that can precipitate allergic emergencies
- Properties of gluten intolerance: gluten structure, evolution, and pathogenicity
However! It may not be a modern fad, so much as a modern genuine increase in incidence.
Widespread varieties of wheat today contain a lot more gluten than wheat of ages past, and many other molecular changes mean there are other compounds in modern grains that never even existed before.
However, the health-related impact of these (novel proteins and carbohydrates) is currently still speculative, and we are not in the business of speculating, so we’ll leave that as a “this hasn’t been studied enough to comment yet but we recognize it could potentially be a thing” factor.
Gluten is bad if (and only if) you have Celiac disease: True or False?
Definitely False; allergies for example are well-evidenced as real; same facts as we discussed/linked just above.
Gluten is bad for everyone and we should avoid it: True or False?
False, tentatively and contingently.
First, as established, there are people with clinically-evidenced Celiac disease, wheat allergy, or similar. Obviously, they should avoid triggering those diseases.
What about the rest of us, and what about those who have non-Celiac gluten sensitivity?
Clinical testing has found that of those reporting non-Celiac gluten sensitivity, nocebo-controlled studies validate that diagnosis in only a minority of cases.
In the following study, for example, only 16% of those reporting symptoms showed them in the trials, and 40% of those also showed a nocebo response (i.e., like placebo, but a bad rather than good effect):
This one, on the other hand, found that positive validations of diagnoses were found to be between 7% and 77%, depending on the trial, with an average of 30%:
Re-challenge Studies in Non-celiac Gluten Sensitivity: A Systematic Review and Meta-Analysis
In other words: non-Celiac gluten sensitivity is a thing, and/but may be over-reported, and/but may be in some part exacerbated by psychosomatic effect.
Note: psychosomatic effect does not mean “imagining it” or “all in your head”. Indeed, the “soma” part of the word “psychosomatic” has to do with its measurable effect on the rest of the body.
For example, while pain can’t be easily objectively measured, other things, like inflammation, definitely can.
As for everyone else? If you’re enjoying your wheat (or similar) products, it’s well-established that they should be wholegrain for the best health impact (fiber, a positive for your health, rather than white flour’s super-fast metabolites padding the liver and causing metabolic problems).
Wheat itself may have other problems, for example FODMAPs, amylase trypsin inhibitors, and wheat germ agglutinins, but that’s “a wheat thing” rather than “a gluten thing”.
That’s beyond the scope of today’s main feature, but you might want to check out today’s featured book!
For a final scientific opinion on this last one, though, here’s what a respected academic journal of gastroenterology has to say:
From coeliac disease to noncoeliac gluten sensitivity; should everyone be gluten-free?
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Practical Programming for Strength Training – by Mark Rippetoe & Andy Baker
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Strength training is an important part of overall health maintenance, but it can be hard to find a good guide to progressive strength improvement that isn’t a bodybuilding book.
This one gives a ground-upwards approach, explaining small details to even quite basic things, before taking the reader through to more advanced progressions, and how to get the most strength-building out of each exercise over time.
As such, this is a good book for anyone of any level from beginner to quite experienced, and you can hop in at any point since there are always catch-up summaries and/or reiterations of the previous concepts that we’re now building on from.
The authors do also talk nutrition, hormones, and so forth, but most of it is about the exercises and the progressions thereof.
There is a slightly patronizing chapter towards the end, about “special populations”, for example offering “novice and intermediate training for women”, but it doesn’t take away from the majority of the book, as the exercises don’t care about your gender. Muscles are muscles, and we all start from wherever we are. Yes, testosterone boosts muscle mass, but let’s face it, there are a lot of women in the world who are stronger than a lot of men.
One thing to bear in mind is that a lot of this is barbell training, so you will need a barbell (or access to one at a gym). If purely bodyweight training is your preference, or perhaps some other form of weightlifting (e.g. kettlebells or such) then this isn’t the book for that.
Bottom line: if strength training is your focus and you like barbells, then this is a great book to take you quite a way along that road.
Click here to check out Practical Programming For Strength Training, and get stronger!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What Does “Balance Your Hormones” Even Mean?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hormonal Health: Is It Really A Balancing Act?
Have you ever wondered what “balancing your hormones” actually means?
The popular view is that men’s hormones look like this:
Testosterone (less) ⟷ Testosterone (more)
…And that women’s hormones look more like this:
♀︎ Estrogen ↭ Progesterone ⤵︎
⇣⤷ FSH ⤦ ↴ ☾ ⤹⤷ Luteinizing Hormone ⤦
DHEA ↪︎ Gonadotrophin ⤾
↪︎ Testosterone? ⥅⛢
Clear as mud, right?
But, don’t worry, Supplements McHerbal Inc will sell you something guaranteed to balance your hormones!
How can a supplement (or dietary adjustment) “balance” all that hotly dynamic chaos, and make everything “balanced”?
The truth is, “balanced” in such a nebulous term, and this is why you will not hear endocrinologists using it. It’s used in advertising to mean “in good order”, and “not causing problems”, and “healthy”.
In reality, our hormone levels depend on everything from our diet to our age to our anatomy to our mood to the time of the day to the phase of the moon.
Not that the moon has an influence on our physiology at all—that’s a myth—but you know, 28 day cycle and all. And, yes, half the hormones affect the levels of the others, either directly or indirectly.
Trying to “balance” them would be quite a game of whack-a-mole, and not something that a “cure-all” single “hormone-balancing” supplement could do.
So why aren’t we running this piece on Friday, for our “mythbusting” section? Well, we could have, but the more useful information is yet to come and will take up more of today’s newsletter than the myth-busting!
What, then, can we do to untangle the confusion of these hormones?
Well first, let’s understand what they do, in the most simple terms possible:
- Estrogen—the most general feminizing hormone from puberty onwards, busiest in the beginning of the menstrual cycle, and starts getting things ready for ovulation.
- Progesterone—secondary feminizing hormone, fluffs the pillows for the oncoming fertilized egg to be implanted, increases sex drive, and adjusts metabolism accordingly. Busiest in the second half of the menstrual cycle.
- Testosterone—is also present, contributes to sex drive, is often higher in individuals with PCOS. If menopause is untreated, testosterone will also rise, because there will be less estrogen
- (testosterone and estrogen “antagonize” each other, which is the colorfully scientific way of saying they work against each other)
- DHEA—Dehydroepiandrosterone, supports production of testosterone (and estrogen!). Sounds self-balancing, but in practice, too much DHEA can thus cause elevated testosterone levels, and thus hirsutism.
- Gonadotrophin—or more specifically human chorionic gonadotrophin, HcG, is “the pregnancy hormone“, present only during pregnancy, and has specific duties relating to such. This is what’s detected in (most) pregnancy test kits.
- FSH—follicle stimulating hormone, is critical to ovulation, and is thus essential to female fertility. On the other hand, when the ovaries stop working, FSH levels will rise in a vain attempt to encourage the ovulation that isn’t going to happen anymore.
- Luteinizing hormone—says “go” to the new egg and sends it on its merry way to go get fertilized. This is what’s detected by ovulation prediction kits.
Sooooooo…
What, for most women, most often is meant by a “hormonal imbalance” is:
- Low levels of E and/or P
- High levels of DHEA and/or T
- Low or High levels of FSH
In the case of low levels of E and/or P, the most reliable way to increase these is, drumroll please… To take E and/or P. That’s it, that’s the magic bullet.
Bonus Tip: take your E in the morning (this is when your body will normally make more and use more) take your P in the evening (it won’t make you sleepy, but it will improve your sleep quality when you do sleep)
In the case of high levels of DHEA and/or T, then that’s a bit more complex:
- Taking E will antagonize (counteract) the unwanted T.
- Taking T-blockers (such as spironolactone or bicalutamide) will do what it says on the tin, and block T from doing the jobs it’s trying to do, but the side-effects are considered sufficient to not prescribe them to most people.
- Taking spearmint or saw palmetto will lower testosterone’s effects
- Scientists aren’t sure how or why spearmint works for this
- Saw palmetto blocks testosterone’s conversion into a more potent form, DHT, and so “detoothes” it a bit. It works similarly to drugs such as finasteride, often prescribed for androgenic alopecia, called “male pattern baldness”, but it affects plenty of women too.
In the case of low levels of FSH, eating leafy greens will help.
In the case of high levels of FSH, see a doctor. HRT (Hormone Replacement Therapy) may help. If you’re not of menopausal age, it could be a sign something else is amiss, so it could be worth getting that checked out too.
What can I eat to boost my estrogen levels naturally?
A common question. The simple answer is:
- Flaxseeds and soy contain plant estrogens that the body can’t actually use as such (too incompatible). They’ve lots of high-quality nutrients though, and the polyphenols and isoflavones can help with some of the same jobs when it comes to sexual health.
- Fruit, especially peaches, apricots, blueberries, and strawberries, contain a lot of lignans and also won’t increase your E levels as such, but will support the same functions and reduce your breast cancer risk.
- Nuts, especially almonds (yay!), cashews, and pistachios, contain plant estrogens that again can’t be used as bioidentical estrogen (like you’d get from your ovaries or the pharmacy) but do support heart health.
- Leafy greens and cruciferous vegetables support a lot of bodily functions including good hormonal health generally, in ways that are beyond the scope of this article, but in short: do eat your greens!
Note: because none of these plant-estrogens or otherwise estrogenic nutrients can actually do the job of estradiol (the main form of estrogen in your body), this is why they’re still perfectly healthy for men to eat too, and—contrary to popular “soy boy” social myths—won’t have any feminizing effects whatsoever.
On the contrary, most of the same foods support good testosterone-related health in men.
The bottom line:
- Our hormones are very special, and cannot be replaced with any amount of herbs or foods.
- We can support our body’s natural hormonal functions with good diet, though.
- Our hormones naturally fluctuate, and are broadly self-correcting.
- If something gets seriously out of whack, you need an endocrinologist, not a homeopath or even a dietician.
In case you missed it…
We gave a more general overview of supporting hormonal health (including some hormones that aren’t sex hormones but are really important too), back in February.
Check it out here: Healthy Hormones And How To Hack Them
Want to read more?
Anthea Levi, RD, takes much the same view:
❝For some ‘hormone-balancing’ products, the greatest risk might simply be lost dollars. Others could come at a higher cost.❞
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: