Just One Thing – by Dr. Michael Mosley
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a collection of easy-to-implement changes that have good science behind them to show how they can benefit us. Some things are obvious (e.g: drink water); others, less so (e.g: sing, to reduce inflammation).
The book is divided thematically into times of the day, though in many cases it’s not a hard rule that a thing needs to be done at a certain time. Others are, like a cold shower in the morning and hot bath before bed—you might not want to switch those around!
The style is very pop-science, and does not have in-line citations for claims, but it does have a bibliography in the bag organized by each “one thing”, e.g. it might say “get some houseplants” and then list a number of references supporting that, with links to the studies showing how that helps. For those with the paper version, don’t worry, you can copy the URL from the book into your browser and see it that way. In any case, there are 2–6 scientific references for each claim, which is very respectable for a pop-sci book.
Bottom line: if you’re looking for evidence-based “one little thing” changes that can make a big difference, this book has lots!
Click here to check out Just One Thing, and improve your life!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Neuroaffirming care values the strengths and differences of autistic people, those with ADHD or other profiles. Here’s how

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve come a long way in terms of understanding that everyone thinks, interacts and experiences the world differently. In the past, autistic people, people with attention deficit hyperactive disorder (ADHD) and other profiles were categorised by what they struggled with or couldn’t do.
The concept of neurodiversity, developed by autistic activists in the 1990s, is an emerging area. It promotes the idea that different brains (“neurotypes”) are part of the natural variation of being human – just like “biodiversity” – and they are vital for our survival.
This idea is now being applied to research and to care. At the heart of the National Autism Strategy, currently in development, is neurodiversity-affirming (neuroaffirming) care and practice. But what does this look like?

Unsplash Reframing differences
Neurodiversity challenges the traditional medical model of disability, which views neurological differences solely through a lens of deficits and disorders to be treated or cured.
Instead, it reframes it as a different, and equally valuable, way of experiencing and navigating the world. It emphasises the need for brains that are different from what society considers “neurotypical”, based on averages and expectations. The term “neurodivergent” is applied to Autistic people, those with ADHD, dyslexia and other profiles.
Neuroaffirming care can take many forms depending on each person’s needs and context. It involves accepting and valuing different ways of thinking, learning and experiencing the world. Rather than trying to “fix” or change neurodivergent people to fit into a narrow idea of what’s considered “normal” or “better”, neuroaffirming care takes a person-centered, strengths-based approach. It aims to empower and support unique needs and strengths.
Neuroaffirming care can look different in a school or clinical setting. Shutterstock/Inna Reznik Adaptation and strengths
Drawing on the social model of disability, neuroaffirming care acknowledges there is often disability associated with being different, especially in a world not designed for neurodivergent people. This shift focuses away from the person having to adapt towards improving the person-environment fit.
This can include providing accommodations and adapting environments to make them more accessible. More importantly, it promotes “thriving” through greater participation in society and meaningful activities.
At school, at work, in clinic
In educational settings, this might involve using universal design for learning that benefits all learners.
For example, using systematic synthetic phonics to teach reading and spelling for students with dyslexia can benefit all students. It also could mean incorporating augmentative and alternative communication, such as speech-generating devices, into the classroom.
Teachers might allow extra time for tasks, or allow stimming (repetitive movements or noises) for self-regulation and breaks when needed.
In therapy settings, neuroaffirming care may mean a therapist grows their understanding of autistic culture and learns about how positive social identity can impact self-esteem and wellbeing.
They may make efforts to bridge the gap in communication between different neurotypes, known as the double empathy problem. For example, the therapist may avoid relying on body language or facial expressions (often different in autistic people) to interpret how a client is feeling, instead of listening carefully to what the client says.
Affirming therapy approaches with children involve “tuning into” their preferred way of communicating, playing and engaging. This can bring meaningful connection rather than compliance to “neurotypical” ways of playing and relating.
In workplaces, it can involve flexible working arrangements (hours, patterns and locations), allowing different modes of communication (such as written rather than phone calls) and low-sensory workspaces (for example, low-lighting, low-noise office spaces).
In public spaces, it can look like providing a “sensory space”, such as at large concerts, where neurodivergent people can take a break and self-regulate if needed. And staff can be trained to recognise, better understand and assist with hidden disabilities.
Combining lived experience and good practice
Care is neuroaffirmative when it centres “lived experience” in its design and delivery, and positions people with disability as experts.
As a result of being “different”, people in the neurodivergent community experience high rates of bullying and abuse. So neuroaffirming care should be combined with a trauma-informed approach, which acknowledges the need to understand a person’s life experiences to provide effective care.
Culturally responsive care acknowledges limited access to support for culturally and racially marginalised Autistic people and higher rates of LGBTQIA+ identification in the neurodivergent community.
In the workplace, we can acknowledge how difference can fuel ideas. Unsplash/Jason Goodman Authentic selves
The draft National Autism Strategy promotes awareness that our population is neurodiverse. It hopes to foster a more inclusive and understanding society.
It emphasises the societal and public health responsibilities for supporting neurodivergent people via public education, training, policy and legislation. By providing spaces and places where neurodivergent people can be their authentic, unmasked selves, we are laying the foundations for feeling seen, valued, safe and, ultimately, happy and thriving.
The author would like to acknowledge the assistance of psychologist Victoria Gottliebsen in drafting this article. Victoria is a member of the Oversight Council for the National Autism Strategy.
Josephine Barbaro, Associate Professor, Principal Research Fellow, Psychologist, La Trobe University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

For Many Rural Women, Finding Maternity Care Outweighs Concerns About Abortion Access
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
BAKER CITY, Ore. — In what has become a routine event in rural America, a hospital maternity ward closed in 2023 in this small Oregon town about an hour from the Idaho border.
For Shyanne McCoy, 23, that meant the closest hospital with an obstetrician on staff when she was pregnant was a 45-mile drive away over a mountain pass.
When McCoy developed symptoms of preeclampsia last January, she felt she had the best chance of getting the care she needed at a larger hospital in Boise, Idaho, two hours away. She spent the final week of her pregnancy there, too far from home to risk leaving, before giving birth to her daughter.
Six months later, she said it seems clear to her that the health care needs of rural young women like her are largely ignored.
For McCoy and others, figuring out how to obtain adequate care to safely have a baby in Baker City has quickly eclipsed concerns about another medical service lacking in the area: abortion. But in Oregon and elsewhere in the country, progressive lawmakers’ attempts to expand abortion access sometimes clash with rural constituencies.
Oregon is considered one of the most protective states in the country when it comes to abortion. There are no legal limits on when someone can receive an abortion in the state, and the service is covered by its Medicaid system. Still, efforts to expand access in the rural, largely conservative areas that cover most of the state have encountered resistance and incredulity.
It’s a divide that has played out in elections in such states as Nevada, where voters passed a ballot measure in November that seeks to codify abortion protections in the state constitution. Residents in several rural counties opposed the measure.
In Oregon, during the months just before the Baker City closure was announced, Democratic state lawmakers were focused on a proposed pilot program that would launch two mobile reproductive health care clinics in rural areas. The bill specified that the van-based clinics would include abortion services.
State Rep. Christine Goodwin, a Republican from a southwestern Oregon district, called the proposal the “latest example” of urban legislators telling rural leaders what their communities need.
The mobile health clinic pilot was eventually removed from the bill that was under discussion. That means no new abortion options in Oregon’s Baker County — and no new state-funded maternity care either.
“I think if you expanded rural access in this community to abortions before you extended access to maternal health care, you would have an uprising on your hands,” said Paige Witham, 27, a member of the Baker County health care steering committee and the mother of two children, including an infant born in October.
A study published in JAMA in early December that examined nearly 5,000 acute care hospitals found that by 2022, 52% of rural hospitals lacked obstetrics care after more than a decade of unit closures. The health implications of those closures for young women, the population most likely to need pregnancy care, and their babies can be significant. Research has shown that added distance between a patient and obstetric care increases the likelihood the baby will be admitted to a neonatal intensive care unit, or NICU.
Witham said that while she does not support abortion, she believes the government should not “legislate it away completely.” She said that unless the government provides far more support for young families, like free child care and better mental health care, abortion should remain legal.
Conversations with a liberal school board member, a moderate owner of a timber company, members of Baker City’s Republican Party chapter, a local doula, several pregnant women, and the director of the Baker County Health Department — many of whom were not rigidly opposed to abortion — all turned up the same answer: No mobile clinics offering abortions here, please.
Kelle Osborn, a nurse supervisor for the Baker County Health Department, loved the idea of a mobile clinic that would provide education and birth control services to people in outlying areas. She was less thrilled about including abortion services in a clinic on wheels.
“It’s not something that should just be handed out from a mobile van,” she said of abortion services. She said people in her conservative rural county would probably avoid using the clinics for anything if they were understood to provide abortion services.
Both Osborn and Meghan Chancey, the health department’s director, said they would rank many health care priorities higher, including the need for a general surgeon, an ICU, and a dialysis clinic.
Nationally, reproductive health care services of all types tend to be limited for people in rural areas, even within states that protect abortion access. More than two-thirds of people in “maternity care deserts” — all of which are in rural counties — must drive more than a half-hour to get obstetric care, according to a 2024 March of Dimes report. For people in the Southern states where lawmakers installed abortion bans, abortion care can be up to 700 miles away, according to a data analysis by Axios.
Nathan Defrees grew up in Baker City and has practiced medicine here since 2017. He works for a family medicine clinic. If a patient asks about abortion, he provides information about where and how one can be obtained, but he doesn’t offer abortions himself.
“There’s not a lot of anonymity in small towns for physicians who provide that care,” he said. “Many of us aren’t willing to sacrifice the rest of our career for that.”
He also pointed to the small number of patients requesting the service locally. Just six people living in Baker County had an abortion in 2023, according to data from the Oregon Department of Public Health. Meanwhile, 125 residents had a baby that year.
A doctor with obstetric training living in another rural part of the state has chosen to quietly provide early-stage abortions when asked. The doctor, concerned for their family’s safety in the small, conservative town where they live, asked not to be identified.
The idea that better access to abortion is not needed in rural areas seems naive, the doctor said. People most in need of abortion often don’t have access to any medical service not already available in town, the doctor pointed out. The first patient the doctor provided an abortion for at the clinic was a meth user with no resources to travel or to manage an at-home medication abortion.
“It seemed entirely inappropriate for me to turn her away for care I had the training and the tools to do,” the doctor said.
Defrees said it has been easier for Baker County residents to get an abortion since the U.S. Supreme Court overturned Roe v. Wade.
A new Planned Parenthood clinic in Ontario, Oregon, 70 miles away in neighboring Malheur County, was built primarily to provide services to people from the Boise metro area, but it also created an option for many living in rural eastern Oregon.
Idaho is one of the 16 states with near-total bans on abortion. Like many states with bans, Idaho has struggled to maintain its already small fleet of fetal medicine doctors. The loss of regional expertise touches Baker City, too, Defrees said.
For example, he said, the treatment plan for women who have a desired pregnancy but need a termination for medical reasons is now far less clear. “It used to be those folks could go to Boise,” he said. “Now they can’t. That does put us in a bind.”
Portland is the next closest option for that type of care, and that means a 300-mile drive along a set of highways that can be treacherous in winter.
“It’s a lot scarier to be pregnant now in Baker City than it ever has been,” Defrees said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post
-

Nutrivore – by Dr. Sarah Ballantyne
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The core idea of this book is that foods can be assigned a numerical value according to their total nutritional value, and that this number can be used to guide a person’s diet such that we will eat, in aggregate, a diet that is more nutritious. So far, so simple.
What Dr. Ballantyne also does, besides explaining and illustrating this system (there are chapters explaining the calculation system, and appendices with values), is also going over what to consider important and what we can let slide, and what things we might need more of to address a wide assortment of potential health concerns. And yes, this is definitely a “positive diet” approach, i.e. it focuses on what to add in, not what to cut out.
The premise of the “positive diet” approach is simple, by the way: if we get a full set of good nutrients, we will be satisfied and not crave unhealthy food.
She also offers a lot of helpful “rules of thumb”, and provides a variety of cheat-sheets and suchlike to make things as easy as possible.
There’s also a recipes section! Though, it’s not huge and it’s probably not necessary, but it’s just one more “she’s thinking of everything” element.
Bottom line: if you’d like a single-volume “Bible of” nutrition-made-easy, this is a very usable tome.
Click here to check out Nutrivore, and start filling up your diet!
Share This Post



Related Posts
-

Vaping: A Lot Of Hot Air?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Vaping: A Lot Of Hot Air?

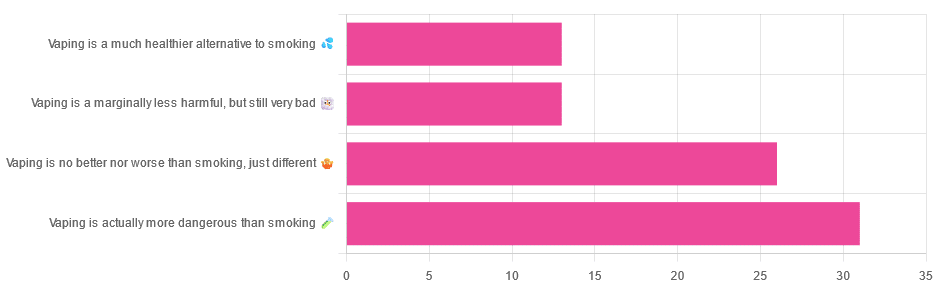
Yesterday, we asked you for your (health-related) opinions on vaping, and got the above-depicted, below-described, set of responses:
- A little over a third of respondents said it’s actually more dangerous than smoking
- A little under a third of respondents said it’s no better nor worse, just different
- A little over 10% of respondents said it’s marginally less harmful, but still very bad
- A little over 10% of respondents said it’s a much healthier alternative to smoking
So what does the science say?
Vaping is basically just steam inhalation, plus the active ingredient of your choice (e.g. nicotine, CBD, THC, etc): True or False?
False! There really are a lot of other chemicals in there.
And “chemicals” per se does not necessarily mean evil green glowing substances that a comicbook villain would market, but there are some unpleasantries in there too:
- Potential harmful health effects of inhaling nicotine-free shisha-pen vapor: a chemical risk assessment of the main components propylene glycol and glycerol
- Inflammatory and Oxidative Responses Induced by Exposure to Commonly Used e-Cigarette Flavoring Chemicals and Flavored e-Liquids without Nicotine
So, the substrate itself can cause irritation, and flavorings (with cinnamaldehyde, the cinnamon flavoring, being one of the worst) can really mess with our body’s inflammatory and oxidative responses.
Vaping can cause “popcorn lung”: True or False?
True and False! Popcorn lung is so-called after it came to attention when workers at a popcorn factory came down with it, due to exposure to diacetyl, a chemical used there.
That chemical was at that time also found in most vapes, but has since been banned in many places, including the US, Canada, the EU and the UK.
Vaping is just as bad as smoking: True or False?
False, per se. In fact, it’s recommended as a means of quitting smoking, by the UK’s famously thrifty NHS, that absolutely does not want people to be sick because that costs money:
Of course, the active ingredients (e.g. nicotine, in the assumed case above) will still be the same, mg for mg, as they are for smoking.
Vaping is causing a health crisis amongst “kids nowadays”: True or False?
True—it just happens to be less serious on a case-by-case basis to the risks of smoking.
However, it is worth noting that the perceived harmlessness of vapes is surely a contributing factor in their widespread use amongst young people—decades after actual smoking (thankfully) went out of fashion.
On the other hand, there’s a flipside to this:
Flavored vape restrictions lead to higher cigarette sales
So, it may indeed be the case of “the lesser of two evils”.
Want to know more?
For a more in-depth science-ful exploration than we have room for here…
BMJ | Impact of vaping on respiratory health
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Doctor Who Wants Us To Exercise Less, & Move More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Today we’re talking about Dr. Rangan Chatterjee. He’s a medical doctor with decades of experience, and he wants us all to proactively stay in good health, rather than waiting for things to go wrong.
Great! What’s his deal?
Dr. Chatterjee advises that we take care of the following four pillars of good health:
- Relaxation
- Food
- Movement
- Sleep
And, they’re not in this order at random. Usually advice starts with diet and exercise, doesn’t it?
But for Dr. Chatterjee, it’s useless to try to tackle diet first if one is stressed-to-death by other things. As for food next, he knows that a good diet will fuel the next steps nicely. Speaking of next steps, a day full of movement is the ideal setup to a good night’s sleep—ready for a relaxing next day.
Relaxation
Here, Dr. Chatterjee advises that we go with what works for us. It could be meditation or yoga… Or it could be having a nice cup of tea while looking out of the window.
What’s most important, he says, is that we should take at least 15 minutes per day as “me time”, not as a reward for when we’ve done our work/chores/etc, but as something integrated into our routine, preferably early in the day.
Food
There are no grand surprises here: Dr. Chatterjee advocates for a majority plant-based diet, whole foods, and importantly, avoiding sugar.
He’s also an advocate of intermittent fasting, but only so far as is comfortable and practicable. Intermittent fasting can give great benefits, but it’s no good if that comes at a cost of making us stressed and suffering!
Movement
This one’s important. Well, they all are, but this one’s particularly characteristic to Dr. Chatterjee’s approach. He wants us to exercise less, and move more.
The reason for this is that strenuous exercise will tend to speed up our metabolism to the point that we will be prompted to eat high calorie quick-energy foods to compensate, and when we do, our body will rush to store that as fat, understanding (incorrectly) that we are in a time of great stress, because why else would we be exerting ourselves that much?
Instead, he advocates for building as much natural movement into our daily routine as possible. Walking more, taking the stairs, doing the gardening/housework.
That said, he does also advise some strength-training on a daily basis—bodyweight exercises like squats and lunges are top of his list.
Sleep
Here, aside from the usual “sleep hygiene” advices (dark cool room, fresh bedding, etc), he also advises we do as he does, and take an hour before bedtime as a purely wind-down time. In gentle lighting, perhaps reading (not on a bright screen!), for example.
Ready to start the next day, relaxed and ready to go.
If you’d like to know more about Dr. Chatterjee’s approach…
You can check out his:
If you don’t know where to start, we recommend the blog! It has a lot of guests there too, including Wim Hof, Gabor Maté, Mindy Pelz, and come to think of it, a lot of other people we’ve also featured ideas from previously!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Black Bean & Butternut Balti
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Protein, fiber, and pungent polyphenols abound in this tasty dish that’s good for your gut, heart, brain, and more:
You will need
- 2 cans (each 14 oz or thereabouts) black beans, drained and rinsed (or: 2 cups black beans, cooked, drained, and rinsed)
- 1 butternut squash, peeled and cut into ½” cubes
- 1 cauliflower, cut into florets
- 1 red onion, finely chopped
- 1 can (14 oz or thereabouts) chopped tomatoes
- 1 cup coconut milk
- ½ bulb garlic, crushed
- 1″ piece of fresh ginger, peeled and finely chopped
- 1 fresh red chili (or multiply per your preference and the strength of your chilis), finely chopped
- 1 tbsp black pepper, coarse ground
- 1 tbsp garam masala
- 2 tsp cumin seeds
- 2 tsp ground coriander
- 1 tsp ground turmeric
- 1 tsp ground paprika
- ½ tsp MSG or 1 tsp low-sodium salt
- Juice of ½ lemon
- Extra virgin olive oil
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 400℉ / 200℃.
2) Toss the squash and cauliflower in a little olive oil, to coat evenly. No need to worry about seasoning, because these are going into the curry later and will get plenty there.
3) Roast them on a baking tray lined with baking paper for about 25 minutes.
You can enjoy a 10-minute break for the first 10 minutes of that, before continuing, such that the timing will be perfect:
4) Heat a little oil in a sauté pan (or anything that’s suitable for both frying and adding volume; we’re going to be using the space later; everything is going in here!) and fry the onion on medium for about 5 minutes, stirring well.
5) Add the spices/seasonings, including the garlic, ginger, and chili, and stir well to combine.
6) Add the tomatoes, beans, and coconut milk, and simmer for 10 minutes. You can add a little water at any time if it seems to need it.
7) Stir in the roasted vegetables (they should be finished now), and heat through. Add the lemon juice and stir.
8) Serve as-is, or with your preferred carbohydrate (we recommend our Tasty Versatile Rice recipe), or if you have time, keep it warm for a while until you’re ready to use it (the flavors will benefit from this time, if available).

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Chickpeas vs Black Beans – Which is Healthier?
- Butternut Squash vs Pumpkin – Which is Healthier?
- Our Top 5 Spices: How Much Is Enough For Benefits? ← 5/5 today!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: