What Does “Balance Your Hormones” Even Mean?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hormonal Health: Is It Really A Balancing Act?
Have you ever wondered what “balancing your hormones” actually means?
The popular view is that men’s hormones look like this:
Testosterone (less) ⟷ Testosterone (more)
…And that women’s hormones look more like this:
♀︎ Estrogen ↭ Progesterone ⤵︎
⇣⤷ FSH ⤦ ↴ ☾ ⤹⤷ Luteinizing Hormone ⤦
DHEA ↪︎ Gonadotrophin ⤾
↪︎ Testosterone? ⥅⛢
Clear as mud, right?
But, don’t worry, Supplements McHerbal Inc will sell you something guaranteed to balance your hormones!
How can a supplement (or dietary adjustment) “balance” all that hotly dynamic chaos, and make everything “balanced”?
The truth is, “balanced” in such a nebulous term, and this is why you will not hear endocrinologists using it. It’s used in advertising to mean “in good order”, and “not causing problems”, and “healthy”.
In reality, our hormone levels depend on everything from our diet to our age to our anatomy to our mood to the time of the day to the phase of the moon.
Not that the moon has an influence on our physiology at all—that’s a myth—but you know, 28 day cycle and all. And, yes, half the hormones affect the levels of the others, either directly or indirectly.
Trying to “balance” them would be quite a game of whack-a-mole, and not something that a “cure-all” single “hormone-balancing” supplement could do.
So why aren’t we running this piece on Friday, for our “mythbusting” section? Well, we could have, but the more useful information is yet to come and will take up more of today’s newsletter than the myth-busting!
What, then, can we do to untangle the confusion of these hormones?
Well first, let’s understand what they do, in the most simple terms possible:
- Estrogen—the most general feminizing hormone from puberty onwards, busiest in the beginning of the menstrual cycle, and starts getting things ready for ovulation.
- Progesterone—secondary feminizing hormone, fluffs the pillows for the oncoming fertilized egg to be implanted, increases sex drive, and adjusts metabolism accordingly. Busiest in the second half of the menstrual cycle.
- Testosterone—is also present, contributes to sex drive, is often higher in individuals with PCOS. If menopause is untreated, testosterone will also rise, because there will be less estrogen
- (testosterone and estrogen “antagonize” each other, which is the colorfully scientific way of saying they work against each other)
- DHEA—Dehydroepiandrosterone, supports production of testosterone (and estrogen!). Sounds self-balancing, but in practice, too much DHEA can thus cause elevated testosterone levels, and thus hirsutism.
- Gonadotrophin—or more specifically human chorionic gonadotrophin, HcG, is “the pregnancy hormone“, present only during pregnancy, and has specific duties relating to such. This is what’s detected in (most) pregnancy test kits.
- FSH—follicle stimulating hormone, is critical to ovulation, and is thus essential to female fertility. On the other hand, when the ovaries stop working, FSH levels will rise in a vain attempt to encourage the ovulation that isn’t going to happen anymore.
- Luteinizing hormone—says “go” to the new egg and sends it on its merry way to go get fertilized. This is what’s detected by ovulation prediction kits.
Sooooooo…
What, for most women, most often is meant by a “hormonal imbalance” is:
- Low levels of E and/or P
- High levels of DHEA and/or T
- Low or High levels of FSH
In the case of low levels of E and/or P, the most reliable way to increase these is, drumroll please… To take E and/or P. That’s it, that’s the magic bullet.
Bonus Tip: take your E in the morning (this is when your body will normally make more and use more) take your P in the evening (it won’t make you sleepy, but it will improve your sleep quality when you do sleep)
In the case of high levels of DHEA and/or T, then that’s a bit more complex:
- Taking E will antagonize (counteract) the unwanted T.
- Taking T-blockers (such as spironolactone or bicalutamide) will do what it says on the tin, and block T from doing the jobs it’s trying to do, but the side-effects are considered sufficient to not prescribe them to most people.
- Taking spearmint or saw palmetto will lower testosterone’s effects
- Scientists aren’t sure how or why spearmint works for this
- Saw palmetto blocks testosterone’s conversion into a more potent form, DHT, and so “detoothes” it a bit. It works similarly to drugs such as finasteride, often prescribed for androgenic alopecia, called “male pattern baldness”, but it affects plenty of women too.
In the case of low levels of FSH, eating leafy greens will help.
In the case of high levels of FSH, see a doctor. HRT (Hormone Replacement Therapy) may help. If you’re not of menopausal age, it could be a sign something else is amiss, so it could be worth getting that checked out too.
What can I eat to boost my estrogen levels naturally?
A common question. The simple answer is:
- Flaxseeds and soy contain plant estrogens that the body can’t actually use as such (too incompatible). They’ve lots of high-quality nutrients though, and the polyphenols and isoflavones can help with some of the same jobs when it comes to sexual health.
- Fruit, especially peaches, apricots, blueberries, and strawberries, contain a lot of lignans and also won’t increase your E levels as such, but will support the same functions and reduce your breast cancer risk.
- Nuts, especially almonds (yay!), cashews, and pistachios, contain plant estrogens that again can’t be used as bioidentical estrogen (like you’d get from your ovaries or the pharmacy) but do support heart health.
- Leafy greens and cruciferous vegetables support a lot of bodily functions including good hormonal health generally, in ways that are beyond the scope of this article, but in short: do eat your greens!
Note: because none of these plant-estrogens or otherwise estrogenic nutrients can actually do the job of estradiol (the main form of estrogen in your body), this is why they’re still perfectly healthy for men to eat too, and—contrary to popular “soy boy” social myths—won’t have any feminizing effects whatsoever.
On the contrary, most of the same foods support good testosterone-related health in men.
The bottom line:
- Our hormones are very special, and cannot be replaced with any amount of herbs or foods.
- We can support our body’s natural hormonal functions with good diet, though.
- Our hormones naturally fluctuate, and are broadly self-correcting.
- If something gets seriously out of whack, you need an endocrinologist, not a homeopath or even a dietician.
In case you missed it…
We gave a more general overview of supporting hormonal health (including some hormones that aren’t sex hormones but are really important too), back in February.
Check it out here: Healthy Hormones And How To Hack Them
Want to read more?
Anthea Levi, RD, takes much the same view:
❝For some ‘hormone-balancing’ products, the greatest risk might simply be lost dollars. Others could come at a higher cost.❞
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

3 drugs that went from legal, to illegal, then back again

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cannabis, cocaine and heroin have interesting life stories and long rap sheets. We might know them today as illicit drugs, but each was once legal.
Then things changed. Racism and politics played a part in how we viewed them. We also learned more about their impact on health. Over time, they were declared illegal.
But decades later, these drugs and their derivatives are being used legally, for medical purposes.
Here’s how we ended up outlawing cannabis, cocaine and heroin, and what happened next.

Peruvian Syrup, containing cocaine, was used to ‘cure’ a range of diseases. Smithsonian Museum of American History/Flickr Cannabis, religion and racism
Cannabis plants originated in central Asia, spread to North Africa, and then to the Americas. People grew cannabis for its hemp fibre, used to make ropes and sacks. But it also had other properties. Like many other ancient medical discoveries, it all started with religion.
Cannabis is mentioned in the Hindu texts known as the Vedas (1700-1100 BCE) as a sacred, feel-good plant. Cannabis or bhang is still used ritually in India today during festivals such as Shivratri and Holi.
From the late 1700s, the British in India started taxing cannabis products. They also noticed a high rate of “Indian hemp insanity” – including what we’d now recognise as psychosis – in the colony. By the late 1800s, a British government investigation found only heavy cannabis use seemed to affect people’s mental health.
This drug bottle from the United States contains cannabis tincture. Wikimedia In the 1880s, cannabis was used therapeutically in the United States to treat tetanus, migraine and “insane delirium”. But not everyone agreed on (or even knew) the best dose. Local producers simply mixed up what they had into a tincture – soaking cannabis leaves and buds in alcohol to extract essential oils – and hoped for the best.
So how did cannabis go from a slightly useless legal drug to a social menace?
Some of it was from genuine health concerns about what was added to people’s food, drink and medicine.
In 1908 in Australia, New South Wales listed cannabis as an ingredient that could “adulterate” food and drink (along with opium, cocaine and chloroform). To sell the product legally, you had to tell the customers it contained cannabis.
Some of it was international politics. Moves to control cannabis use began in 1912 with the world’s first treaty against drug trafficking. The US and Italy both wanted cannabis included, but this didn’t happen until until 1925.
Some of it was racism. The word marihuana is Spanish for cannabis (later Anglicised to marijuana) and the drug became associated with poor migrants. In 1915, El Paso, Texas, on the Mexican border, was the first US municipality to ban the non-medical cannabis trade.
By the late 1930s, cannabis was firmly entrenched as a public menace and drug laws had been introduced across much of the US, Europe and (less quickly) Australia to prohibit its use. Cannabis was now a “poison” regulated alongside cocaine and opiates.
The 1936 movie Reefer Madness fuelled cannabis paranoia. Motion Picture Ventures/Wikimedia Commons The 1936 movie Reefer Madness was a high point of cannabis paranoia. Cannabis smoking was also part of other “suspect” new subcultures such as Black jazz, the 1950s Beatnik movement and US service personnel returning from Vietnam.
Today recreational cannabis use is associated with physical and mental harm. In the short term, it impairs your functioning, including your ability to learn, drive and pay attention. In the long term, harms include increasing the risk of psychosis.
But what about cannabis as a medicine? Since the 1980s there has been a change in mood towards experimenting with cannabis as a therapeutic drug. Medicinal cannabis products are those that contain cannabidiol (CBD) or tetrahydrocannabinol (THC). Today in Australia and some other countries, these can be prescribed by certain doctors to treat conditions when other medicines do not work.
Medicinal cannabis has been touted as a treatment for some chronic conditions such as cancer pain and multiple sclerosis. But it’s not clear yet whether it’s effective for the range of chronic diseases it’s prescribed for. However, it does seem to improve the quality of life for people with some serious or terminal illnesses who are using other prescription drugs.
Cocaine, tonics and addiction
Several different species of the coca plant grow across Bolivia, Peru and Colombia. For centuries, local people chewed coca leaves or made them into a mildly stimulant tea. Coca and ayahuasca (a plant-based psychedelic) were also possibly used to sedate people before Inca human sacrifice.
In 1860, German scientist Albert Niemann (1834-1861) isolated the alkaloid we now call “cocaine” from coca leaves. Niemann noticed that applying it to the tongue made it feel numb.
But because effective anaesthetics such as ether and nitrous oxide had already been discovered, cocaine was mostly used instead in tonics and patent medicines.
Hall’s Coca Wine was made from the leaves of the coca plant. Stephen Smith & Co/Wellcome Collection, CC BY Perhaps the most famous example was Coca-Cola, which contained cocaine when it was launched in 1886. But cocaine was used earlier, in 1860s Italy, in a drink called Vin Mariani – Pope Leo XIII was a fan.
With cocaine-based products easily available, it quickly became a drug of addiction.
Cocaine remained popular in the entertainment industry. Fictional detective Sherlock Holmes injected it, American actor Tallulah Bankhead swore by it, and novelist Agatha Christie used cocaine to kill off some of her characters.
In 1914, cocaine possession was made illegal in the US. After the hippy era of the 1960s and 1970s, cocaine became the “it” drug of the yuppie 1980s. “Crack” cocaine also destroyed mostly Black American urban communities.
Cocaine use is now associated with physical and mental harms. In the short and long term, it can cause problems with your heart and blood pressure and cause organ damage. At its worst, it can kill you. Right now, illegal cocaine production and use is also surging across the globe.
But cocaine was always legal for medical and surgical use, most commonly in the form of cocaine hydrochloride. As well as acting as a painkiller, it’s a vasoconstrictor – it tightens blood vessels and reduces bleeding. So it’s still used in some types of surgery.
Heroin, coughing and overdoses
Opium has been used for pain relief ever since people worked out how to harvest the sap of the opium poppy. By the 19th century, addictive and potentially lethal opium-based products such as laudanum were widely available across the United Kingdom, Europe and the US. Opium addiction was also a real problem.
Because of this, scientists were looking for safe and effective alternatives for pain relief and to help people cure their addictions.
In 1874, English chemist Charles Romley Alder Wright (1844-1894) created diacetylmorphine (also known as diamorphine). Drug firm Bayer thought it might be useful in cough medicines, gave it the brand name Heroin and put it on the market in 1898. It made chest infections worse.
Allenburys Throat Pastilles contained heroin and cocaine. Seth Anderson/Flickr, CC BY-NC Although diamorphine was created with good intentions, this opiate was highly addictive. Shortly after it came on the market, it became clear that it was every bit as addictive as other opiates. This coincided with international moves to shut down the trade in non-medical opiates due to their devastating effect on China and other Asian countries.
Like cannabis, heroin quickly developed radical chic. The mafia trafficked into the US and it became popular in the Harlem jazz scene, beatniks embraced it and US servicemen came back from Vietnam addicted to it. Heroin also helped kill US singers Janis Joplin and Jim Morrison.
Today, we know heroin use and addiction contributes to a range of physical and mental health problems, as well as death from overdose.
However, heroin-related harm is now being outpaced by powerful synthetic opioids such as oxycodone, fentanyl, and the nitazene group of drugs. In Australia, there were more deaths and hospital admissions from prescription opiate overdoses than from heroin overdoses.
In a nutshell
Not all medicines have a squeaky-clean history. And not all illicit drugs have always been illegal.
Drugs’ legal status and how they’re used are shaped by factors such as politics, racism and social norms of the day, as well as their impact on health.
Philippa Martyr, Lecturer, Pharmacology, Women’s Health, School of Biomedical Sciences, The University of Western Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Sprout Book – by Doug Evans
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sprouting seeds are more nutritious than most people think, and “seeds” is also a much broader category than people think. Beyond even chia and sunflower and such, this book bids us remember that onions do not just appear on supermarket shelves fully formed (to give just one example of many); most plants come from seeds and of those, most can be usefully sprouted.
The author, most well-known for his tech companies, here is selling us a very low-tech health kick with very little profit to be found except for our health. By sprouting seeds of many kinds at home, we can enjoy powerful superfoods that are not only better than, but also cheaper than, most supplements.
Nor are the benefits of sprouting things marginal; we’re not talking about a 1–10% increase in bioavailable so much as what’s often a 100–1000% increase.
After explaining the science and giving a primer on sprouting things for oneself, there is a wide selection of recipes, but the biggest benefit of the book is in just getting the reader up-and-running with at-home sprouting.
Bottom line: if you like the idea of letting food be your medicine and even like the idea of essentially growing your own food with zero gardening skills, then this is an excellent book for you.
Share This Post
-

Rethinking Diabetes – by Gary Taubes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve previously reviewed this author’s “The Case Against Sugar” and “Why We Get Fat And What To Do About It“. There’s an obvious theme, and this book caps it off nicely:
By looking at the history of diabetes treatment (types 1 and 2) in the past hundred years, and analysing the patterns over time, we can see how:
- diabetics have been misled a lot over time by healthcare providers
- we can learn from those mistakes going forwards
Happily, he does this without crystal-balling the future or expecting diet to fix, for example, a pancreas that can’t produce insulin. But what he does do is focus on the “can” items rather than the “can’t” items.
In the category of criticism, one of the strategies he argues for is basically the keto diet, which is indeed just fine for diabetes but often not great for the heart in the long-term (it depends on various factors, including genes). However, even if you choose not to implement that, there is plenty more to try out in this book.
Bottom line: whether you have diabetes, love someone who does, or just plain like to be on top of your glycemic health, this book is full of important insights and opportunities to improve things progressively along the way.
Click here to check out Rethinking Diabetes, and rethink diabetes!
Share This Post





-

Radical Longevity – by Dr. Ann Gittleman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Gittleman takes a comprehensive approach, advising us about avoiding AGEs, freeing up fascia, stimulating cellular rejuvenation, the mind-gut connection, keeping the immune system healthy, and more.
The “plan” promised by the subtitle involves identifying the key factors of nutrition and lifestyle most impactful to you, and adjusting them accordingly, in a multistep, author-walks-the-reader-by-the-hand process.
There’s also, for those who prefer it, a large section (seven chapters) on a body part/system by body part/system approach, e.g. brain health, heart health, revitalizing skin, reversing hair loss, repairing bones, muscles, joints, etc.
The writing style is quite casual,butalso with a mind to education, with its call-out boxes, bullet-point summaries, and so forth. There is a “select references” section, but if one wants to find studies, it’s often necessary to go looking, as there aren’t inline citations.
Bottom line: we’d love to see better referencing, but otherwise this is a top-tier anti-aging book, and a lot more accessible than most, without skimping on depth and breadth.
Click here to check out Radical Longevity, and get rejuvenating radically!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
No Equipment Muscle Gain Routine for Ages 50+
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sarcopenia, the loss of muscle mass commonly associated with aging, can be a big problem as it leaves us vulnerable to injury (and also isn’t great for the metabolism—keeping adequate muscle mass ensures keeping the metabolism ticking over nicely). Will Harlow, over-50s specialist physiotherapist, is here to share a routine that works without weights:
Where it counts
There’s a fair amount of emphasis here on the lower body and core. That’s because in practical terms, this is what matters more for our health than having bulging biceps:
- First exercise: donkey calf raises to build strength in the calves using a chair.
- Second exercise: single-leg elevated lunge to work the quads and glutes, using a step or books for elevation.
- Third exercise: slow sit-to-stand for quads, glutes, and core strength, focusing on a slow descent.
- Fourth exercise: wall press-up to strengthen the chest, shoulders, and arms, with a variation using towels for increased resistance.
- Final exercise: shoulder raises using bottles or similar weights to target the shoulders and rotator cuffs.
Ok, so that last one was a slight cheat on his part as it does require grabbing a weight, but it’s not specialist equipment at least, and can just be something you grabbed at home. It’s also the least important of the five exercises, and can be skipped if necessary.
For more on all of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

10almonds Tells The Tea…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s Bust Some Myths!
It’s too late after puberty, hormones won’t change xyz
While yes, many adult trans people dearly wish they’d been able to medically transition before going through the “wrong” puberty, the truth is that a lot of changes will still occur later… even to “unchangeable” things like the skeleton.
The body is remaking itself throughout life, and hormones tell it how to do that. Some parts are just quicker or slower than others. Also: the skeleton is pulled-on constantly by our muscles, and in a battle of muscle vs bone, muscle will always win over time.
Examples of this include:
- trans men building bigger bones to support their bigger muscles
- trans women getting smaller, with wider hips and a pelvic tilt
Trans people have sporting advantages
Assuming at least a year’s cross-sex hormonal treatment, there is no useful advantage to being trans when engaging in a sport. There are small advantages and disadvantages (which goes for any person’s body, really). For example:
- Trans women will tend to be taller than cis women on average…
- …but that larger frame is now being powered by smaller muscles, because they shrink much quicker than the skeleton.
- Trans men taking T are the only athletes allowed to take testosterone…
- …but they will still often be smaller than their fellow male competitors, for example.
Read: Do Trans Women Athletes Have Advantages? (A rather balanced expert overview, which does also cover trans men)
There’s a trans population explosion; it’s a social contagion epidemic!

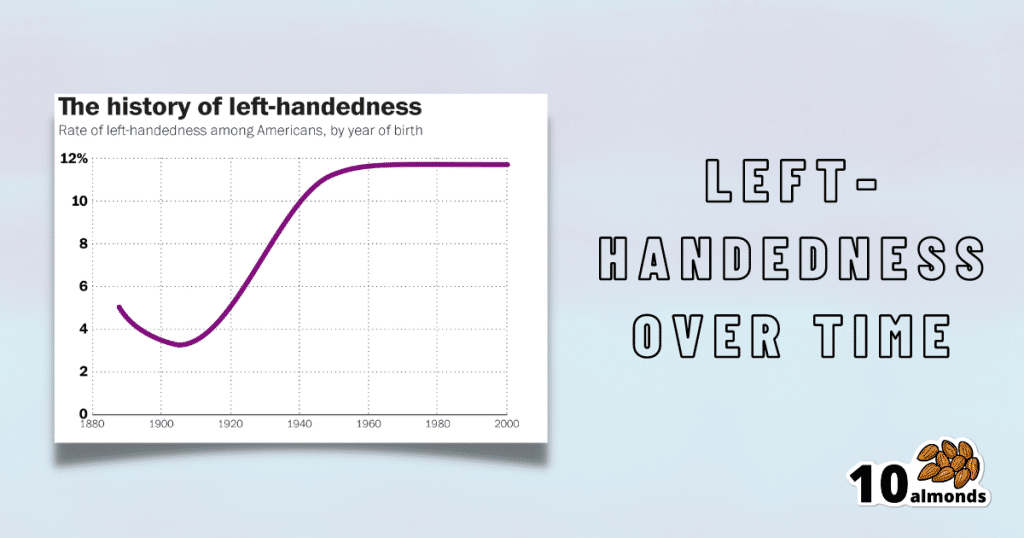
Source for figures: The Overall Rate Of Left-Handedness (Researchgate)
Left-handed people used to make up around 3% of the population… Until the 1920s, when that figure jumped sharply upwards, before plateauing at around 12% in around 1960, where it’s stayed since. What happened?! Simple, schools stopped forcing children to use their right hand.
Today, people ask for trans healthcare because they know it exists! Decades ago, it wasn’t such common knowledge.
The same explanation can be applied to other “population explosions” such as for autism and ADHD.
Fun fact: Mt. Everest was “discovered” in 1852, but scientists suspect it probably existed long before then! People whose ancestors were living on it long before 1852 also agree. Sometimes something exists for a long time, and only comes to wider public awareness later.
Transgender healthcare is too readily available, especially to children!
To believe some press outlets, you’d think:
- HRT is available from school vending machines,
- kids can get a walk-in top surgery at recess,
- and there’s an after-school sterilization club.
In reality, while availability varies from place to place, trans healthcare is heavily gatekept. Even adults have trouble getting it, often having to wait years and/or pay large sums of money… and get permission from a flock of doctors, psychologists, and the like. For those under the age of 18, it’s almost impossible in many places, even with parental support.
Puberty-blockers shouldn’t be given to teenagers, as the effects are irreversible
Quick question: who do you think should be given puberty-blockers? For whom do you think they were developed? Not adults, for sure! They were not developed for trans teens either, but for cis pre-teens with precocious puberty, to keep puberty at bay, to do it correctly later. Nobody argues they’re unsafe for much younger cis children, and only object when it’s trans teens.
They’re not only safe and reversible, but also self-reversing. Stop taking them, and the normally scheduled puberty promptly ensues by itself. For trans kids, the desired effect is to buy the kid time to make an informed and well-considered decision. After all, the effects of the wrong puberty are really difficult to undo!
A lot of people rush medical transition and regret it!
Trans people wish it could be rushed! It’s a lot harder to get gender-affirming care as a trans person, than it is to get the same (or comparable) care as a cis person. Yes, cis people get gender-affirming care, from hormones to surgeries, and have done for a long time.
As for regret… Medical transition has around a 1% regret rate. For comparison, hip replacement has a 4.8% regret rate and knee replacement has a 17.1% regret rate.
A medical procedure with a 99% success rate would generally be considered a miracle cure!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: