The Knowledge That Harvard Medical School’s Clinical Instructor Dr. Monique Tello Thinks Everyone SHOULD Have About Heart Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anyone (who has not had a double mastectomy, anyway) can get breast cancer.
Breast cancer, if diagnosed early (before it spreads), has a 98% survival rate.
That survival rate drops to 31% if diagnosed after it has spread through the body.
(The US CDC’s breast cancer “stat bite” page has more stats and interactive graphs, so click here to see those charts and get the more detailed low-down on mortality/survival rates with various different situations)
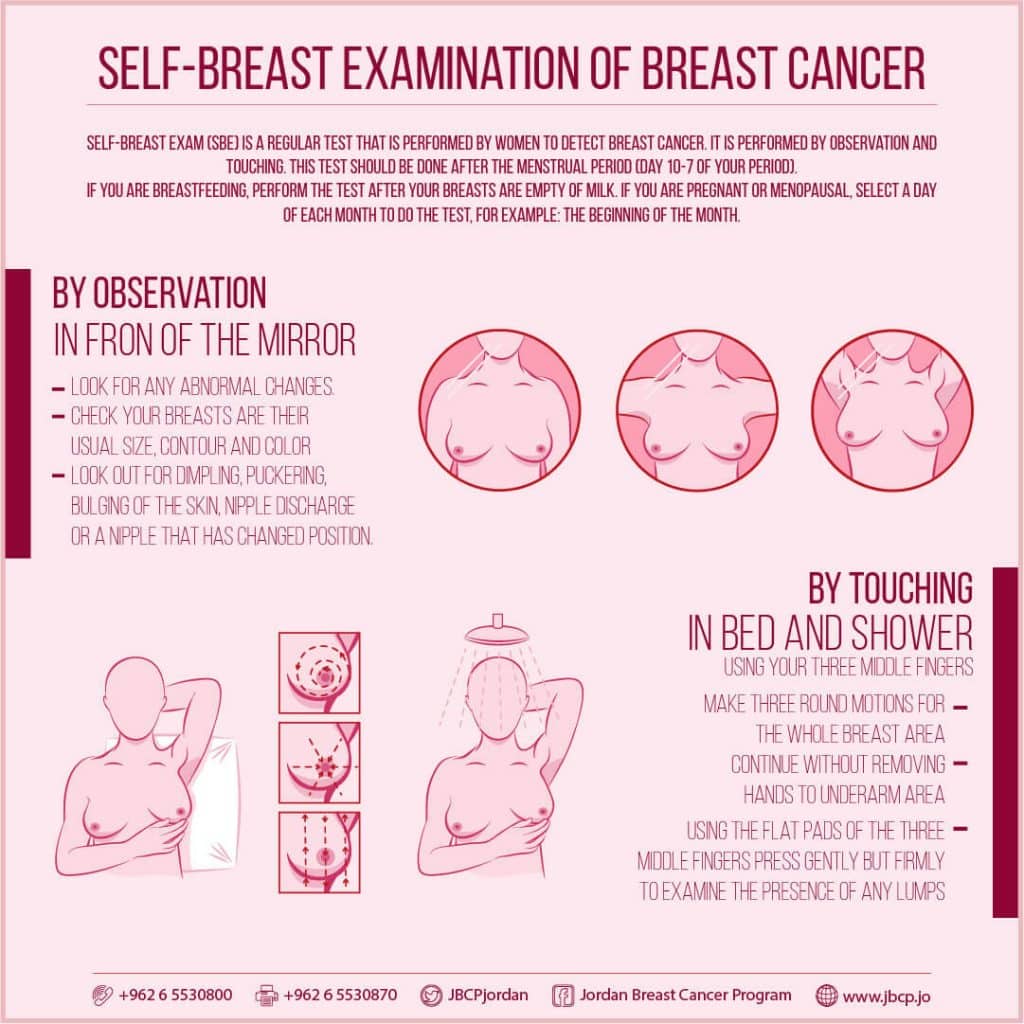
We think that the difference between 98% and 31% survival rates is more than enough reason to give ourselves a monthly self-check at the very least! You’ve probably seen how-to diagrams before, but here are instructions for your convenience:
This graphic created by the Jordan Breast Cancer Program (check them out, as they have lots of resources)
If you don’t have the opportunity to take matters into your own hands right now, rather than just promise yourself “I’ll do that later”, take this free 4-minute Breast Health Assessment from Aurora Healthcare. Again, we think the difference early diagnosis can make to your survival chances make these tests well worth it.
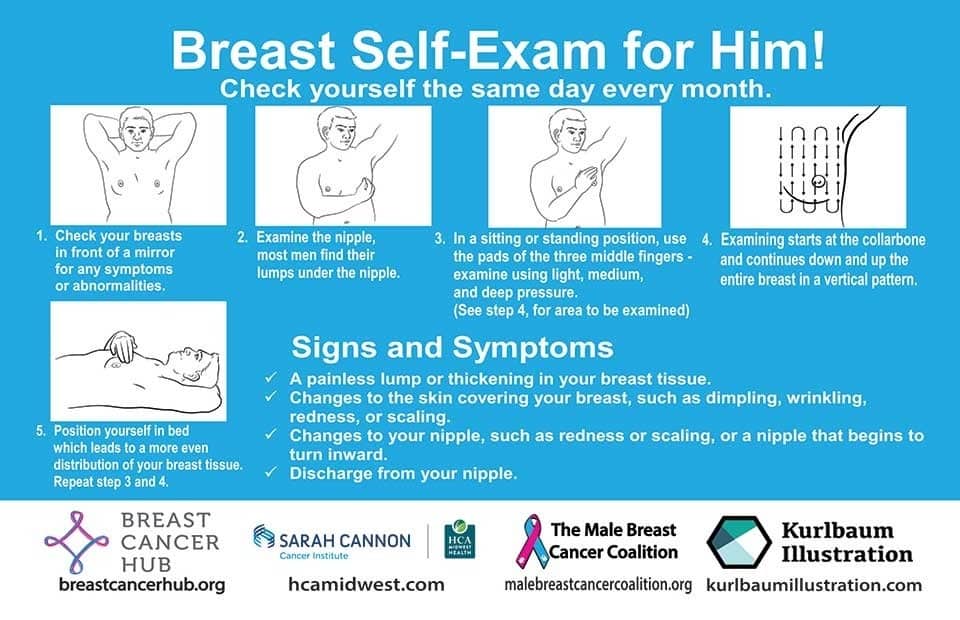
Lest we forget, men can also get breast cancer (the CDC has a page for men too), especially if over 50. But how do you check for breast cancer, when you don’t have breasts in the commonly-understood sense of the word?
So take a moment to do this (yes, really actually do it!), and set a reminder in your calendar to repeat it monthly—there really is no reason not to! Take care of yourself; you’re important.
Pssst! Did you scroll past the diagrams, looking for the online 4-minute test promised by the subtitle? If so, scroll back up; the link is in the middle!
Harvard Medical School’s Clinical Instructor’s Five-Point Plan for Heart Health
Dr. Monique Tello, M.D., M.P.H., is a practicing physician at Massachusetts General Hospital, director of research and academic affairs for the MGH DGM Healthy Lifestyle Program, clinical instructor at Harvard Medical School, and author of the evidence-based lifestyle change guide Healthy Habits for Your Heart.
Here are what she says are the five most important factors to help keep your ticker ticking:
5. Have (at most) a moderate alcohol intake! While there are polyphenols such as resveratrol in red wine that could boost heart health, there’s so little per glass that you may need 100–1000 glasses to get the dosage that provides benefits in mouse studies. If you’re not a mouse, it may not be as beneficial, and Dr. Tello recommends drinking no more than one glass per day of any alcohol. What constitutes a glass? It varies from one kind of drink to another, so here’s a handy guide.
4. Don’t smoke. Best of all to never start. But if you did, quit. Simple as that. There is no healthy amount of smoking. While paradoxically, quitting smoking may of course be stressful to you, the long term gains are considered more than worth it. As with all advice, do consult your own physician for guidance, as individual circumstances may vary, and that may change the best approach for you.
3. Maintain a healthy body weight. While BMI (Body Mass Index) is not a perfect system, it’s a system in popular use, and Dr. Tello recommends keeping a BMI between 18.5 and 24.9.
What’s your BMI? It takes into account your height and weight; here’s a Quick BMI Calculator for your convenience.
2. Keep a healthy level of physical activity—which ideally means at least 30 minutes per day vigorous activity, but obviously if you’re not used to this, take it slowly and build up over time. Even just small lifestyle changes (walking where possible, taking the stairs instead of the elevator where possible, etc) can add up to a big difference.
1. Enjoy a healthy diet. This is the single most important thing, and the best modern scientific consensus holds that the best diet contains plenty of vegetables, fruits and nuts, whole grains, and omega-3 fatty acids, while it avoids processed meats, sugar-sweetened beverages, trans fats (what are trans fats?), and too much sodium.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between burnout and depression?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If your summer holiday already feels like a distant memory, you’re not alone. Burnout – a state of emotional, physical and mental exhaustion following prolonged stress – has been described in workplaces since a 5th century monastery in Egypt.
Burnout and depression can look similar and are relatively common conditions. It’s estimated that 30% of the Australian workforce is feeling some level of burnout, while almost 20% of Australians are diagnosed with depression at some point in their lives.
So what’s the difference between burnout and depression?
Burnout is marked by helplessness and depression by hopelessness. They can have different causes and should also be managed differently.

Yuri A/Shutterstock What is burnout?
The World Health Organization defines burnout as an “occupational phenomenon” resulting from excessively demanding workload pressures. While it is typically associated with the workplace, carers of children or elderly parents with demanding needs are also at risk.
Our research created a set of burnout symptoms we captured in the Sydney Burnout Measure to assist self-diagnosis and clinicians undertaking assessments. They include:
- exhaustion as the primary symptom
- brain fog (poor concentration and memory)
- difficulty finding pleasure in anything
- social withdrawal
- an unsettled mood (feeling anxious and irritable)
- impaired work performance (this may be result of other symptoms such as fatigue).
People can develop a “burning out” phase after intense work demands over only a week or two. A “burnout” stage usually follows years of unrelenting work pressure.
What is depression?
A depressive episode involves a drop in self-worth, increase in self-criticism and feelings of wanting to give up. Not everyone with these symptoms will have clinical depression, which requires a diagnosis and has an additional set of symptoms.
Clinically diagnosed depression can vary by mood, how long it lasts and whether it comes back. There are two types of clinical depression:
- melancholic depression has genetic causes, with episodes largely coming “out of the blue”
- non-melancholic depression is caused by environmental factors, often triggered by significant life events which cause a drop in self-worth.
When we created our burnout measure, we compared burnout symptoms with these two types of depression.
Burnout shares some features with melancholic depression, but they tend to be general symptoms, such as feeling a loss of pleasure, energy and concentration skills.
We found there were more similarities between burnout and non-melancholic (environmental) depression. This included a lack of motivation and difficulties sleeping or being cheered up, perhaps reflecting the fact both have environmental causes.
Looking for the root cause
The differences between burnout and depression become clearer when we look at why they happen.
Personality comes into play. Our work suggests a trait like perfectionism puts people at a much higher risk of burnout. But they may be less likely to become depressed as they tend to avoid stressful events and keep things under control.
Excessive workloads can contribute to burnout. tartanparty/Shutterstock Those with burnout generally feel overwhelmed by demands or deadlines they can’t meet, creating a sense of helplessness.
On the other hand, those with depression report lowered self-esteem. So rather than helpless they feel that they and their future is hopeless.
However it is not uncommon for someone to experience both burnout and depression at once. For example, a boss may place excessive work demands on an employee, putting them at risk of burnout. At the same time, the employer may also humiliate that employee and contribute to an episode of non-melancholic depression.
What can you do?
A principal strategy in managing burnout is identifying the contributing stressors. For many people, this is the workplace. Taking a break, even a short one, or scheduling some time off can help.
Australians now have the right to disconnect, meaning they don’t have to answer work phone calls or emails after hours. Setting boundaries can help separate home and work life.
Burnout can be also be caused by compromised work roles, work insecurity or inequity. More broadly, a dictatorial organisational structure can make employees feel devalued. In the workplace, environmental factors, such as excessive noise, can be a contributor. Addressing these factors can help prevent burnout.
As for managing symptoms, the monks had the right idea. Strenuous exercise, meditation and mindfulness are effective ways to deal with everyday stress.
Regular exercise can help manage symptoms of burnout. alexei_tm/Shutterstock Deeper contributing factors, including traits such as perfectionism, should be managed by a skilled clinical psychologist.
For melancholic depression, clinicians will often recommend antidepressant medication.
For non-melancholic depression, clinicians will help address and manage triggers that are the root cause. Others will benefit from antidepressants or formal psychotherapy.
While misdiagnosis between depression and burnout can occur, burnout can mimic other medical conditions such as anemia or hypothyroidism.
For the right diagnosis, it’s best to speak to your doctor or clinician who should seek to obtain a sense of “the whole picture”. Only then, once a burnout diagnosis has been affirmed and other possible causes ruled out, should effective support strategies be put in place.
If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14.
Correction: This article originally stated that depression is marked by helplessness and burnout by hopelessness, when in fact it is vice versa. This has been amended.
Gordon Parker, Scientia Professor of Psychiatry, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Blood and Water
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Q&A with the 10almonds Team
Q: I really loved the information about macular degeneration! I was wondering if you have any other advice about looking after eye health?
A: We may well do a full feature on it sometime! Meanwhile, some top tips include:
- Eat your greens (as you know from this last Tuesday’s edition of 10almonds)!
- Exercise! Generally. We’re not talking about eye exercises here, we’re talking about exercises that will support:
- Healthy heart rate
- Healthy blood pressure
- Healthy blood oxygenation
- Healthy blood sugar levels
- Healthy blood flow in general (so keep hydrated too! There’s a reason phlebotomists ask you to be well-hydrated before they take blood)
Eye health is a good indicator for a lot of other things, and that’s because whether or not the eyes are the window to your soul, they’re definitely the window to what your blood’s like, and that affects (and is affected by) so many other things.
- On that note, don’t smoke!
- Protect your eyes physically, too. This means:
- UV-blocking sunglasses when appropriate
- Protective eye-wear when appropriate
You think safety glasses are for laboratories and construction sites, then you go and do comparable tasks in your home? Your eyes are just as damageable in your kitchen or garden as they would be in a lab or workshop.
Some bits and bobs that can help:
- Safety sunglasses! Because a thing can do two jobs (useful in the garden now the days are brightening up!)
- Pulse oximeter! Check your own heart rate, pulse strength, and blood oxygenation at home!
- Blood pressure monitor! Because it’s so important for a lot of things and you really should have one.
Share This Post
-
Cavolo Nero & Sweet Potato Hash
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
🎶 Sweet potato hash? It’s a seasonal smash… Catches on in a flash… Let’s do the hash 🎶
You will need
- 6 oz cavolo nero, tough stems removed, chopped
- 1 large sweet potato, diced
- 1 large red onion, finely chopped
- 1 parsnip, grated
- 1 small red pepper, chopped
- 4 oz baby portobello mushrooms, chopped
- ½ cup fresh or thawed peas
- ¼ bulb garlic, thinly sliced
- 1 tbsp nutritional yeast
- 2 tsp black pepper, coarse ground
- 1 tsp dried rosemary
- 1 tsp dried thyme (dried for convenience; fresh is also fine if you have it)
- 1 tsp red chili flakes (dried for convenience; fresh is also fine if you have it)
- 1 tsp ground turmeric
- ½ tsp MSG or 1 tsp low-sodium salt
- Extra virgin olive oil
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 425℉ / 220℃.
2) Toss the diced sweet potato in 1 tbsp olive oil, as well as the nutritional yeast, ground turmeric, black pepper, and MSG/salt, ensuring an even distribution. Roast in the oven on a lined baking tray, for 30 minutes, turning at least once to get all sides of the potato. When it is done, remove from the oven and set aside.
3) Heat a little oil in a sauté pan or large skillet (either is fine; we’re not adding liquids today), and fry the onion, parsnip, and pepper until softened, which should take about 5 minutes (this is one reason why we grated the parsnip; the other is for the variation in texture).
4) Add the garlic, mushrooms, herbs, and chili flakes, and cook for a further 1 minute, while stirring.
5) Add the cavolo nero and peas, stir until the cavolo nero begins to wilt, and then…
6) Add the roasted sweet potato; cook for about 5 more minutes, pressing down with the spatula here and there to mash the ingredients together.
7) Turn the hash over when it begins to brown on the bottom, to lightly brown the other side too.
8) Serve hot.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Brain Food? The Eyes Have It!
- Which Bell Peppers To Pick?
- Ergothioneine: “The Longevity Vitamin” (That’s Not A Vitamin)
- Our Top 5 Spices: How Much Is Enough For Benefits?
- What’s Your Plant Diversity Score?
Take care!
Share This Post




Related Posts
-

7 Healthy Gut Habits For Women Over 40 – by Lara West
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
With regard to the titular 7 healthy gut habits for women over 40, a chapter is devoted to each one of those habits, and she goes into quite some detail in each category, more than you might expect.
As for the 7 things, we’ll not keep them a mystery; they are:
- Intermittent fasting
- Prebiotics & probiotics
- Mindful eating
- Understanding ingredients
- Movement
- Sleep
- Stress management
Of course, all of these things are good regardless of one’s age or gender, but West is writing with women over 40 in mind, and as such, she will focus on things that are especially relevant to those of us who are indeed women over 40.
You may be wondering: what if I’m a long way over 40, and menopause is a distant memory? In that case, 90% of this will still be relevant to you; the only parts that won’t be, are those that pertain specifically to the menopausal transitional phase itself, rather than the post-menopause state.
You may also be wondering: what if I’m a man, and menopause is just not in the cards for me? In that case, maybe about 70% of this will still be relevant to you, because of the broad applicability of most of the advice. That said, if it’s just for yourself, you’d probably do better with a book of which 100% is relevant to you, rather than this one.
The style is conversational pop-science, with personal anecdotes mixed in with references to science. It’s definitely on the light/easy-reading end of books that we’ve reviewed on the topic.
Bottom line: if you’re a woman over 40 who would like to improve your gut health, this book was written for you.
Click here to check out 7 Healthy Gut Habits For Women Over 40, and rediscover vitality!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Stop Cancer 20 Years Ago
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Get Abreast And Keep Abreast

This is Dr. Jenn Simmons. Her specialization is integrative oncology, as she—then a breast cancer surgeon—got breast cancer, decided the system wasn’t nearly as good from the patients’ side of things as from the doctors’ side, and took to educate herself, and now others, on how things can be better.
What does she want us to know?
Start now
If you have breast cancer, the best time to start adjusting your lifestyle might be 20 years ago, but the second-best time is now. We realize our readers with breast cancer (or a history thereof) probably have indeed started already—all strength to you.
What this means for those of us without breast cancer (or a history therof) is: start now
Even if you don’t have a genetic risk factor, even if there’s no history of it in your family, there’s just no reason not to start now.
Start what, you ask? Taking away its roots. And how?
Inflammation as the root of cancer
To oversimplify: cancer occurs because an accidentally immortal cell replicates and replicates and replicates and takes any nearby resources to keep on going. While science doesn’t know all the details of how this happens, it is a factor of genetic mutation (itself a normal process, without which evolution would be impossible), something which in turn is accelerated by damage to the DNA. The damage to the DNA? That occurs (often as not) as a result of cellular oxidation. Cellular oxidation is far from the only genotoxic thing out there, and a lot of non-food “this thing causes cancer” warnings are usually about other kinds of genotoxicity. But cellular oxidation is a big one, and it’s one that we can fight vigorously with our lifestyle.
Because cellular oxidation and inflammation go hand-in-hand, reducing one tends to reduce the other. That’s why so often you’ll see in our Research Review Monday features, a line that goes something like:
“and now for those things that usually come together: antioxidant, anti-inflammatory, anticancer, and anti-aging”
So, fight inflammation now, and have a reduced risk of a lot of other woes later.
See: How to Prevent (or Reduce) Inflammation
Don’t settle for “normal”
People are told, correctly but not always helpfully, such things as:
- It’s normal to have less energy at your age
- It’s normal to have a weaker immune system at your age
- It’s normal to be at a higher risk of diabetes, heart disease, etc
…and many more. And these things are true! But that doesn’t mean we have to settle for them.
We can be all the way over on the healthy end of the distribution curve. We can do that!
(so can everyone else, given sufficient opportunity and resources, because health is not a zero-sum game)
If we’re going to get a cancer diagnosis, then our 60s are the decade where we’re most likely to get it. Earlier than that and the risk is extant but lower; later than that and technically the risk increases, but we probably got it already in our 60s.
So, if we be younger than 60, then now’s a good time to prepare to hit the ground running when we get there. And if we missed that chance, then again, the second-best time is now:
See: Focusing On Health In Our Sixties
Fast to live
Of course, anything can happen to anyone at any age (alas), but this is about the benefits of living a fasting lifestyle—that is to say, not just fasting for a 4-week health kick or something, but making it one’s “new normal” and just continuing it for life.
This doesn’t mean “never eat”, of course, but it does mean “practice intermittent fasting, if you can”—something that Dr. Simmons strongly advocates.
See: Intermittent Fasting: We Sort The Science From The Hype
While this calls back to the previous “fight inflammation”, it deserves its own mention here as a very specific way of fighting it.
It’s never too late
All of the advices that go before a cancer diagnosis, continue to stand afterwards too. There is no point of “well, I already have cancer, so what’s the harm in…?”
The harm in it after a diagnosis will be the same as the harm before. When it comes to lifestyle, preventing a cancer and preventing it from spreading are very much the same thing, which is also the same as shrinking it. Basically, if it’s anticancer, it’s anticancer, no matter whether it’s before, during, or after.
Dr. Simmons has seen too many patients get a diagnosis, and place their lives squarely in the hands of doctors, when doctors can only do so much.
Instead, Dr. Simmons recommends taking charge of your health as best you are able, today and onwards, no matter what. And that means two things:
- Knowing stuff
- Doing stuff
So it becomes our responsibility (and our lifeline) to educate ourselves, and take action accordingly.
Want to know more?
We recently reviewed her book, and heartily recommend it:
The Smart Woman’s Guide to Breast Cancer – by Dr. Jenn Simmons
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Aging with Grace – by Dr. David Snowdon
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this book is not: a book about Christianity. Don’t worry, we didn’t suddenly change the theme of 10almonds.
Rather, what this book is: a book about a famous large (n=678) study into the biology of aging, that took a population sample of women who had many factors already controlled-for, e.g. they ate the same food, had the same schedule, did the same activities, etc—for many years on end. In other words, a convent of nuns.
This allowed for a lot more to be learned about other factors that influence aging, such as:
- Heredity / genetics in general
- Speaking more than one language
- Supplementing with vitamins or not
- Key adverse events (e.g. stroke)
- Key chronic conditions (e.g. depression)
The book does also cover (as one might expect) the role that community and faith can play in healthy longevity, but since the subjects were 678 communally-dwelling people of faith (thus: no control group of faithless loners), this aspect is discussed only in anecdote, or in reference to other studies.
The author of this book, by the way, was the lead researcher of the study, and he is a well-recognised expert in the field of Alzheimer’s in particular (and Alzheimer’s does feature quite a bit throughout).
The writing style is largely narrative, and/but with a lot of clinical detail and specific data; this is by no means a wishy-washy book.
Bottom line: if you’d like to know what nuns were doing in the 1980s to disproportionally live into three-figure ages, then this book will answer those questions.
Click here to check out Aging with Grace, and indeed age with grace!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: