Why Your Brain Blinds You For 2 Hours Every Day
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
…and then covers its tracks so that you don’t notice:
Now you see it…
The world you experience is not an accurate representation of reality. Your brain actively constructs your perception, editing your memories as they happen and manipulating your sense of time. What you perceive as the present moment is actually a processed and reconstructed version of past events.
Nor is your vision anywhere near as detailed as it seems. Only a small central portion is in high resolution, while the rest is blurry. Your brain compensates for this by filling in the gaps with its best guess and/or what it believes is there from the last time you saw it. Your eyes constantly make rapid movements called saccades, and during these (i.e. when your eyes are moving), your vision momentarily shuts down—making you effectively blind for (in total, if we add them all up) about two hours every day (according to this video, anyway; our calculations find it to be more than that, but you get the idea). Your brain stitches together the visual input, creating a seamless experience that feels continuous (much like an animation reel composed of still images).
Why does it do this?
It’s because your senses operate at different speeds—light reaches your eyes in nanoseconds, sound in milliseconds, and touch signals in tens of milliseconds. However, your brain processes these inputs together, creating the illusion of a smooth and simultaneous experience. In reality, what you perceive as the present is actually a delayed and selectively edited version of the past.
Instead of showing you the world as it is, your brain predicts what will happen next. In high-speed situations, such as playing table tennis, if your brain relied on past sensory data, you wouldn’t react in time. Instead, it estimates an object’s future position and presents that prediction as your visual reality.
This also means that because your brain effectively sees things slightly sooner than you do, your brain has already prepared multiple possible responses and when an event occurs, it quickly selects the most likely course of action, deleting the alternatives before you are even aware of them. By the time you think you’ve made a decision, your body has already acted.
This goes for more than just the things we think of as requiring quick reactions!
Walking is a complex task that involves multiple time layers—your brain processes past feedback, assesses your current state, and predicts future movements. That’s why it was something that cyberneticists found difficult to recreate for a very long time. If something unexpected happens, like slipping cartoon-style on a banana peel, your body reacts before you consciously notice the danger. Your spinal cord and brainstem trigger emergency reflexes to stabilize you before your conscious mind even catches up.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
This Main Feature Should Take You Two Minutes (and 18 Seconds) To Read ← There’s a problem nobody wants to talk about when it comes to speed-reading; can you guess what it is based on what we just talked about above?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is Your Diet Causing You Hair Loss?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to diet and hair health, most people know to get vitamin something, consume a mineral or so (usually zinc), and skip the polonium.
But, there’s a little more to it than most people realize:
Foods For & Against
Researchers (Dr. Beatriz Teixeira et al.) investigated, by means of a huge literature review (taking data from 17 observational studies, with 613,320 participants, of whom, mostly women), what things actually matter the most, for and against.
First, what not to do:
Foods and drinks that worsen hair loss include sugar-sweetened beverages, and even more strongly, alcohol:
- Sugar spikes cause inflammation that disrupts hair cycles
- Alcohol contributes in a whole stack of ways, both directly and indirectly, including:
- nutrient deficiencies (hypothesis: due to people drinking a higher portion of their calories in alcohol rather than eating nutritious food)
- poor absorption of nutrients (because alcohol causes the body to do almost everything worse, and especially messes with the gut, and not in a good way—one might struggle to spell “dysbiosis” when one’s had a tipple or two too many, but suffice it to say, alcohol causes the gut microbiome to swing wildly in the direction of Bad Things™, including C. albicans, also called simply Candida, the fungus which puts its roots through your intestinal walls, making holes there giving you leaky gut syndrome, and also interfaces with your nervous system via its roots that escape the gut and access the vagus nerve, and thus gives you cravings for more alcohol/sugar/flour, by sending false signals up to your brain) (we’re not exaggerating, check out the papers we cited in the relevant section of this article on gut health)
- liver stress (because that’s where alcohol is metabolized, and our liver is not supposed to have to do that much work)
- poor sleep (because of how it disrupts brain function, including while sleeping, at which time the brain’s job is normally “restore this” and it can’t do that correctly while impaired)
- systemic inflammation (because of the combination of the above plus the fact that the alcohol itself is toxic, and even when metabolized, produces sugars that also worsen inflammation)
Now, some things most people know about:
Zinc and biotin (vitamin B7) deficiencies can cause thinning; adults need 30 μg vitamin B7 daily from foods like seeds, nuts, and sweet potatoes (to pick some out from the paper; there are plenty more options, of course). The researchers concluded that beyond that, extra supplementation is unlikely to help without deficiency.
Now, into lesser-known things:
Insufficient protein can trigger shedding; the researchers suggest about 0.5 g per pound of body weight daily, which is a very normal recommendation. We wrote about this more here: How Much Protein Do We Need, Really?
On which note, the researchers also tentatively recommend considering collagen, but note that while it seems entirely reasonable that it should help, the actual science is mostly not there for it yet (i.e. mostly hasn’t been done). Most collagen RCTs have been about skin health or joint health; less about hair. For more on that though, do see our research review on this: We Are Such Stuff As Fish Are Made Of
And if you are vegetarian/vegan? Worry not, because you can simply enjoy The Best Foods For Collagen Production, picking the vegetarian/vegan options in each category as applicable.
And as for other supplements of note:
- Persimmon leaf: linked to better hair density and thickness through antioxidants like quercetin that improve scalp blood flow; available as tea or supplements.
- Pumpkin seed oil: in a study of men with male pattern baldness, 400 mg daily for 24 weeks led to greater growth, likely by reducing DHT, the hair-thinning hormone (it does more things than that, but that’s what’s relevant here—actually, while we’re on this, let’s note for the record that while DHT thins head hair, it increases body hair, which for many people isn’t a combination they’re hoping for)
- Vitamin D: five studies found higher levels protective against hair loss; a suggested dose is 2,000 IU daily, though excess carries toxicity risk, so do keep within the recommended bounds (and double-check what other supplements have “plus vitamin D” tagged on, and/or foods “fortified with vitamin D”).
- Iron: supplementation improved growth in women; absorption is best when paired with vitamin C; dietary sources include spinach, lentils, and almonds. See also: The Iron Dilemma: Factors To Consider
Finally, in the category of specific foods that were mostly strongly associated with healthy hair growth, the researchers highlighted:
- Cruciferous vegetables (e.g. broccoli, cauliflower, kale, sprouts, etc) likely due to antioxidant and anti-inflammatory phytochemicals, and especially sulforaphane.
- Soy products (especially edamame & tofu, i.e., the least-processed of soy products) likely due to the top-tier amino acid profile, plus that while the phytoestrogens can’t be used as estrogens in the body (not compatible), they can be broken down and the “ingredients” used to produce your own estrogen, if (and only* if) you have working ovaries.
- *Ok, so that was technically a lie; if you have working testes, then these can and do also produce estrogen, but in truly truly tiny amounts, and more than counterbalanced by the testosterone they produce. We wrote a bit about the science of ovaries and testes doing each other’s jobs, here. So if you are a reader with working testes rather than ovaries, then be aware: you could not physically eat enough soy to cause them to crank out enough estrogen to make the slightest change to your hair or any other part of your body. So our original statement stands, for all practical purposes: soy products will only increase your E levels if you have working ovaries to produce the E in question.
You can read the paper in full, here: Assessing the relationship between dietary factors and hair health: A systematic review
Want to learn more?
If you want to get very serious about it, you might want to consider: Hair-Loss Remedies, By Science
And/or if you want to go a drug-free route but without relying solely on diet, then check out: Gentler Hair Health Options
Take care!
Share This Post
-

The Brain-Gut Highway: A Two-Way Street
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Brain-Gut Two-Way Highway

This is Dr. Emeran Mayer. He has the rather niche dual specialty of being a gastroenterologist and a neurologist. He has published over 353 peer reviewed scientific articles, and he’s a professor in the Departments of Medicine, Physiology, and Psychiatry at UCLA. Much of his work has been pioneering medical research into gut-brain interactions.
We know the brain and gut are connected. What else does he want us to know?
First, that it is a two-way interaction. It’s about 90% “gut tells the brain things”, but it’s also 10% “brain tells the gut things”, and that 10% can make more like a 20% difference, if for example we look at the swing between “brain using that 10% communication to tell gut to do things worse” or “brain using that 10% communication to tell gut to do things better”, vs the midpoint null hypothesis of “what the gut would be doing with no direction from the brain”.
For example, if we are experiencing unmanaged chronic stress, that is going to tell our gut to do things that had an evolutionary advantage 20,000–200,000 years ago. Those things will not help us now. We do not need cortisol highs and adrenal dumping because we ate a piece of bread while stressed.
Read more (by Dr. Mayer): The Stress That Evolution Has Not Prepared Us For
With this in mind, if we want to look after our gut, then we can start before we even put anything in our mouths. Dr. Mayer recommends managing stress, anxiety, and depression from the head downwards as well as from the gut upwards.
Here’s what we at 10almonds have written previously on how to manage those things:
- No-Frills, Evidence-Based Mindfulness
- How To Set Anxiety Aside
- The Mental Health First-Aid You’ll Hopefully Never Need
Do eat for gut health! Yes, even if…
Unsurprisingly, Dr. Mayer advocates for a gut-friendly, anti-inflammatory diet. We’ve written about these things before:
…but there’s just one problem:
For some people, such as with IBS, Crohn’s, and colitis, the Mediterranean diet that we (10almonds and Dr. Mayer) generally advocate for, is inaccessible. If you (if you have those conditions) eat as we describe, a combination of the fiber in many vegetables and the FODMAPs* in many fruits, will give you a very bad time indeed.
*Fermentable Oligo-, Di-, Monosaccharides And Polyols
Dr. Mayer has the answer to this riddle, and he’s not just guessing; he and his team did science to it. In a study with hundreds of participants, he measured what happened with adherence (or not) to the Mediterranean diet (or modified Mediterranean diet) (or not), in participants with IBS (or not).
The results and conclusions from that study included:
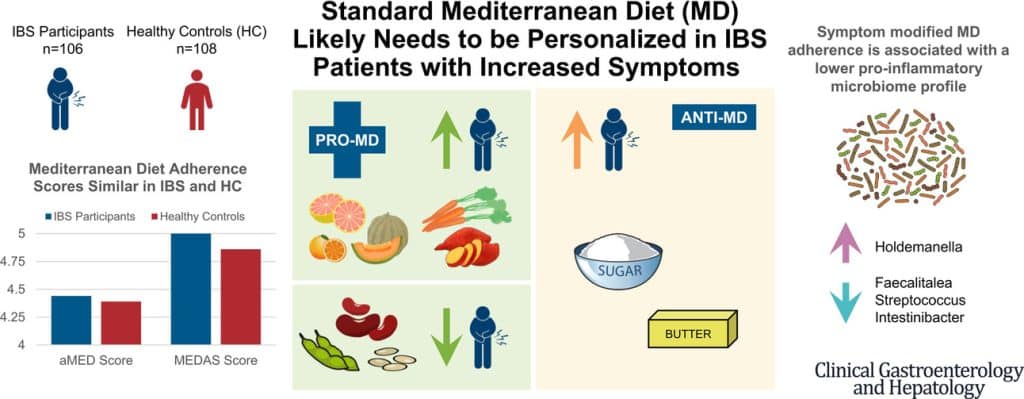
❝Among IBS participants, a higher consumption of fruits, vegetables, sugar, and butter was associated with a greater severity of IBS symptoms. Multivariate analysis identified several Mediterranean Diet foods to be associated with increased IBS symptoms.
A higher adherence to symptom-modified Mediterranean Diet was associated with a lower abundance of potentially harmful Faecalitalea, Streptococcus, and Intestinibacter, and higher abundance of potentially beneficial Holdemanella from the Firmicutes phylum.
A standard Mediterranean Diet was not associated with IBS symptom severity, although certain Mediterranean Diet foods were associated with increased IBS symptoms. Our study suggests that standard Mediterranean Diet may not be suitable for all patients with IBS and likely needs to be personalized in those with increased symptoms.❞
In graphical form:

And if you’d like to read more about this (along with more details on which specific foods to include or exclude to get these results), you can do so…
- The study itself (full article): The Association Between a Mediterranean Diet and Symptoms of Irritable Bowel Syndrome
- Dr. Mayer’s blog (lay explanation): The Benefits of a Modified Mediterranean Diet for Irritable Bowel Syndrome
Want to know more?
Dr. Mayer offers many resources, including a blog, books, recipes, podcasts, and even a YouTube channel:
Share This Post
-
Why Sitting Hurts Your Back Or Legs After An Hour
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Amy Konvalin explains (and what to do about it, besides “sit less”):
Is sitting getting on your nerves?
The problem: sitting with your hips bent to about 90° increases tension on the nerves that run from your lower back into your legs, and in a seated position, the low-back muscles often tighten and compress joints and discs, which can increase pressure on those nerves.
Fun fact: posture does matter, but not the way most people think!
Specifically: leaning to one side, crossing your legs, or sitting with one leg tucked changes the forces through your hips and spine and can increase nerve pressure or muscular tension.
The good news is, it’s not usually not stenosis or classic sciatica: spinal stenosis often improves when sitting and sciatica typically affects only one leg, so pain in both legs that appears mainly during sitting is more consistent with nerve sensitization*. In particular, if leg or back symptoms vanish after 3–5 minutes of walking, the problem is often temporary nerve irritation rather than a serious structural issue because movement relieves the tension cycle.
*This refers to how nerves leaving your lower back can become mildly irritated, which causes the muscles they supply to contract, and that muscle tightness further irritates the nerves in a feedback loop that, happily, movement can quickly break
One myth to be aware of is that of “military posture”: aggressively pulling your shoulders back and pushing your chest out can flatten the natural curves of your spine and create unnecessary strain instead of helping.
Another myth is that lumbar rolls will fix everything: they can help some people maintain a curve in the lower back, but if they’re positioned incorrectly or are too large they can worsen symptoms.
The key is, rather than trying to force a “perfect” posture (which usually isn’t anyway), to instead find the neutral position where your body can sit comfortably with minimal muscular effort. If comfortable, place both feet flat on the floor with equal weight and avoid crossing your legs so your pelvis and “sit bones” remain stable.
A particularly important thing that a lot of people miss: aim to keep your hips slightly higher than your knees because this gently tilts your pelvis forwards and makes it easier for your spine to stack naturally.
On which note, if it’s comfortable to do so, sit tall so your head rests above your shoulders and your shoulders above your hips, imagining a string lifting the top of your head upward without forcing your chest or shoulders.
And of course, all the usual standard advices do apply too—sit less often if you can, enjoy movement breaks, stay hydrated, etc.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Stand Up For Your Health (Or Don’t) ← our main feature on this also includes more things you can do if you must sit, to make sitting less bad!
Take care!
Share This Post


Related Posts
-

What Menopause Does To The Heart
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
World Menopause Day: Menopause & Cardiovascular Disease Risk
Today, the 18th of October, is World Menopause Day.
The theme for this year is cardiovascular disease (CVD), and if your first reaction is to wonder what that has to do with the menopause, then this is the reason why it’s being featured. Much of the menopause and its effects are shrouded in mystery; not because of a lack of science (though sometimes a bit of that too), but rather, because it is popularly considered an unimportant, semi-taboo topic.
So, let’s be the change we want to see, and try to fix that!
What does CVD have to do with the menopause?
To quote Dr. Anjana Nair:
❝The metabolic and clinical factors secondary to menopause, such as dyslipidemia, insulin resistance, fat redistribution and systemic hypertension, contribute to the accelerated risk for cardiovascular aging and disease.
Atherosclerosis appears to be the end result of the interaction between cardiovascular risk factors and their accentuation during the perimenopausal period.
The increased cardiovascular risk in menopause stems from the exaggerated effects of changing physiology on the cardiovascular system.❞
Source: Cardiovascular Changes in Menopause
See also: Menopause-associated risk of cardiovascular disease
Can we do anything about it?
Yes, we can! Here be science:
- Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association
- Cardiovascular risk in menopausal women and our evolving understanding of menopausal hormone therapy: risks, benefits, and current guidelines for use
This (in few words: get your hormone levels checked, and consider HRT if appropriate) is consistent with the advice from gynecologist Dr. Jen Gunter, whom we featured back in August:
What You Should Have Been Told About The Menopause Beforehand
What about lifestyle changes?
We definitely can do some good things; here’s what the science has to say:
- Mediterranean diet: yes, evidence-based
- High soy consumption: mixed evidence, unclear. So, eat it if you want, don’t if you don’t.
- Supplements e.g. vitamins and minerals: yes, evidence-based.
- Supplements e.g. herbal preparations: many may help, but watch out for adverse interactions with meds. Check with your pharmacist or doctor.
- Supplements; specifically CBD: not enough evidence yet
- Exercise: yes, evidence-based—especially low-impact high-resistance training, for bone strength, as well as regular moderate-intensity exercise and/or High-Intensity Interval Training, to guard against CVD.
For a full low-down on all of these:
Revealing the evidence-based lifestyle solutions to managing your menopause symptoms
Want to know more?
You can get the International Menopause Society’s free downloadable booklet here:
Menopause & Cardiovascular Disease: What Women Need To Know
You may also like our previous main feature:
What Does “Balance Your Hormones” Even Mean?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Meds Most Likely To Produce A Dangerous “Prescribing Cascade” In Later Life
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what is a “prescribing cascade”?
It’s what happens when a medication causes a side effect (or even a bunch of side effects), which can then lead to a “side effect train” whereby the patient then has to take something else to treat the side effect, then something else to treat the side effect(s) of that medication, and so on, until they are taking an increasingly large stack of medications.
To use a common statin as an example, a book that we reviewed cites a case in which a woman’s LDL levels were high and she was prescribed simvastatin (Zocor), 20mg/day. Here’s what happened, in sequence:
- Her own non-statin self-prescription (with her doctor’s signature) worked, and she went back to her life, her work, and took up running.
- She started getting panic attacks. So, her doctor prescribed her sertraline (Zoloft) (a very common SSRI antidepressant) and when that didn’t fix it, paroxetine (Paxil). This didn’t work either… because the problem was not actually her mental health. The panic attacks got worse…
- Then, while exercising, she started noticing progressive arm and leg weakness. Her doctor finally took her off the simvastatin, and temporarily switched to ezetimibe (Zetia), a less powerful nonstatin drug that blocks cholesterol absorption, which change eased her arm and leg problem.
- As the Zetia was a stopgap measure, the doctor put her on atorvastatin (Lipitor). Now she got episodes of severe chest pressure, and a skyrocketing heart rate. She also got tremors and lost her body temperature regulation.
- So the doctor stopped the atorvastatin and tried rosovastatin (Crestor), on which she now suffered exhaustion (we’re not surprised, by this point) and muscle pains in her arms and chest.
- So the doctor stopped the rosovastatin and tried lovastatin (Mevacor), and now she had the same symptoms as before, plus light-headedness.
- So the doctor stopped the lovastatin and tried fluvastatin (Lescol). Same thing happened.
- So he stopped the fluvastatin and tried pravastatin (Pravachol), without improvement.
- So finally he took her off all these statins because the high LDL was less deleterious to her life than all these things.
- She did her own research, and went back to the doctor to ask for cholestyramine (Questran), which is a bile acid sequestrent and nothing to do with statins. She also asked for a long-acting niacin. In high doses, niacin (one of the B-vitamins) raises HDL (good) cholesterol, lowers LDL, and lowers tryglycerides.
You can find that book, here: The Truth About Statins – by Barbara H. Roberts, M.D.
The highest-risk meds to be aware of
Researchers (Dr. Lisa Ellet et al.) investigated the prevalance of this happening in people entering long-term residential aged care (a demographic already at increased risk for overmedication, and also easy to observe), and found that before entering aged care, 16.7% of residents had at least one statistically significant prescribing cascade, increasing to 25.1% after admission.
Of these, many cascades involved medicines already known to carry higher risks in older adults, including antipsychotics, benzodiazepines, and opioids.
In other words, bluntly, the meds most commonly given by doctors and other prescribers to make patients less bothersome to them.
That said, not for nothing did we use statins as an example above, because starting statins was associated with later initiation of several other medications, including antipsychotics and antidepressants, while benzodiazepine use was associated with later antipsychotic prescribing.
The lesson to be learned from this?
❝There’s a real opportunity here to intervene earlier through routine medication reviews, better monitoring of side effects and, where appropriate, deprescribing strategies❞
~ Dr. Gill Caughey, another researcher in this study
You can read this paper in full, here: Prescribing cascades potentially associated with harms before and after transition to long-term care facilities
Want to know more?
You might find these previous articles of ours of interest:
- Are You Taking PIMs? Getting Off The Overmedication Train ← “PIMs” stands for “potentially inappropriate medications”, be they prescribed purely in error, or as part of a prescribing cascade
- Medications That Shouldn’t Be Taken Long-term (With Natural Alternatives)
- The Common Meds That Make You More Likely To Die From A fall
- The Commonly-Prescribed Painkiller That Barely Works (And Is Dangerous)
- The Common Meds That Make You Much More Susceptible To Heatstroke ← especially important in the kind of weather many of us are having these days!
And for a more in-depth exploration than we have room for here, check out this book that we reviewed:
To Medicate or Not? That is the Question! – by Dr. Asha Bohannon
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Cancer Journey – by Dr. Chadi Nabhan
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
After a brief introduction of what cancer actually is and what causes it, the layout of the rest of the book is in chronological order of patient experience, that is to say, what to expect during the journey from screening and diagnosis, to one’s first oncology visit (the author being an oncologist himself), how cancer staging works, getting second opinions, and a chapter-by-chapter review of many different treatment options, ranging from surgery and chemotherapy, to radiation and hormonal therapies, and even more modern targeted therapies, immunotherapy, cellular therapies, and yes, complementary and alternative therapies, amongst others we haven’t listed for the sake of brevity.
He doesn’t leave it there though; he also talks managing side effects, monitoring for recurrence, and even caring for the caregiver(s), along with eventual survivorship and that emotional journey, or if it comes down to it, palliative and hospice care.
Finishing on a hopeful note, he also brings attention to novel approaches that are being trialled presently, and the prospects for the near future of cancer care.
The style is very human and readable, notwithstanding that the author has hundreds of peer-reviewed publications to his name, the content here is presented in a much more approachable, less clinical way, while still conveying all the information that needs to be conveyed.
Bottom line: if you or a loved one is facing cancer, this book will be an invaluable resource.
Click here to check out The Cancer Journey, and understand each part of it!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: