Ridged Nails: What Are They Telling You?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Yaseen Arsalan, a Doctor of Pharmacy, has advice on the “nutraceutical” side of things:
Onychorrhexis
Sounds like the name of a dinosaur, but it’s actually the condition that creates the vertical ridges that sometimes appear on nails. It’s especially likely in the case of thinner nails, and/or certain nutritional deficiencies. Overuse of certain chemicals (including nail polish remover, hair products that get on your hands a lot, and cleaning fluids) can also cause it. It can also be worsened by various conditions, including eczema, psoriasis, hypothyroidism, anemia, and amyloidosis, but it won’t usually be outright caused by those alone.
There are two main kinds of ridges on nails:
- Vertical ridges: associated with hypothyroidism, anemia, and aging. Often an indicator of low iron.
- Horizontal ridges (Beau’s lines): caused by interrupted nail growth, brute force trauma, chemotherapy, acrylic nails, and gel nail polishes. Can also be an indicator of low zinc.
There are an assortment of medical treatments available, which Dr. Arsalan discusses in the video, but for home remedy treatment, he recommends:
- Nail-strengthening creams (look for coconut oil, shea butter, beeswax, vitamin E)
- Hydration (this is about overall hydration e.g. water intake)
- Careful nail trimming (fingernails with a curved shape and toenails straight across)
- Nail ridge filler (he recommends the brand Barrielle, for not containing formaldehyde or formalin)
- Moisturization (with cuticle oil or hand creams, because that hydration we talked about earlier is important, and we want it to stay inside the nail)
For more on those things, plus the medical treatments plus other “how to avoid this” measures, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- The Counterintuitive Dos and Don’ts of Nail Health
- Regular Nail Polish vs Gel Nail Polish – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How To Keep On Keeping On?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Keep On Keeping On… Long Term!
For many when it comes to health-related goals and practices, it’s easy to find ourselves in a bit of a motivational dip around this time of year. The enthusiasm of new year’s resolutions has been and gone, and there’s not yet much of a drive to “get a beach body” or “be summer-ready”.
A word to the wise on those before moving on, though:
- How to get a beach body: take your body to a beach. Voilà. Beach body.
- Remember: the beach is there for your pleasure and entertainment, not the other way around!
- How to be summer-ready: the real question is, will summer be ready for you?
But what is this, demotivational rhetoric to discourage you from getting fit and healthy?
Not at all, but rather, to be sure that you’re pursuing your own goals and not just what you feel might be expected of you.
All that in mind, let’s get to the tips…
Focus on adding health
It can be tempting (and even, good) to cut down on unhealthy things. But when it comes to motivation, it’s harder to stay motivated for deprivation, than it is for some healthy addition to life.
So for example, this philosophy would advocate for:
- Instead of counting calories, count steps! Or even…
- Instead of counting calories, count colors! Eat the rainbow and all that. No, skittles do not count, but eating a variety of naturally different-colored foods will tend to result in adding different nutrients to your diet.
- Instead of cutting out sugar, add fruit! How many per day will you go for? If you don’t eat much fruit as it is, consider making it a goal to have even just one piece of fruit a day, then build up from there. Find fruit you like! If you pick the fruit you want instead of the fruit you think you “should” have, it’s basically a dessert snack.
We’ve recommended it before, and we’ll recommend it again, but if you’re interested in “adding health”, you should definitely check out:
Dr. Greger’s Daily Dozen (checklist, plus app if you want it)
More details: it’s a checklist of 12 things you should try to include in your diet, with a free streak-tracking app, if you want it, all based on the same scientific research as the best-selling book “How Not To Die”.
“Minimum effort!”
Did you see the movie “Deadpool”? The protagonist has a catch-phrase as he goes into battle, saying to himself “Maximum effort!”.
And, that’s all very well and good if your superpower is immediate recovery from pretty much anything, but for the rest of us, sometimes it’s good to hold ourselves to “minimum effort!”.
Sometimes, something worth doing is worth doing just a little a bit. It’s always better than nothing! Even if feels like you gained nothing from it, it’s the foundation of a habit, and the habit will grow and add up. Sometimes it may even take you by surprise…
Don’t feel like doing 20 bodyweight squats? Do literally just one. Make a deal with yourself: do just one, then you can stop if you like. Then after you’ve done one, you might think to yourself “huh, that wasn’t so bad”, and you try out a few more. Maybe after 5 you can feel your blood pumping a bit and you think “you know what, that’s enough for now”, and great, you did 5x as much exercise as you planned! Wonder what you’ll do tomorrow!
(personal note from your writer here: I’ve managed to “just extend this exercise a little bit more than last time” my way into hour-long exercise sessions before now; I started with “just 10 squats” or “just one sun salutation” etc, to get myself out of a no-exercise period that I’d slipped into, and it’s amazing how quickly adding just a little bit to the previous day’s “minimum effort!” adds up to a very respectable daily exercise session)
Wondering what a good, easy, respectable short term goal could be?
Check Out, For Example: The Seven-Minute Workout
(You might have heard of this one before; it’s an incredibly efficient well-optimized short complete workout that requires no special equipment, just a bit of floorspace and a wall—the above app allows for customizations of it per your preferences, but the basic routine is an excellent starting point for most people)
Commit to yourself (and do any self-negotiation up-front)
Really commit, though. No “or I will look silly because I told people I’d do it”, no “or I will donate x amount to charity” etc, just “I will do it and that’s that”. If you find yourself second-guessing yourself or renegotiating with yourself, just shut that down immediately and refuse to consider it.
Note: you should have break-clauses in this contract with yourself, though. For example, “unless I am ill or injured” is a sensible rule to have in advance for most exercise regimes that weren’t undertaken with your illness or injury in mind.
Make a “To-Don’t” list
Much like how addicts are often advised to not try to quit more than one thing at once, we must also be mindful of not taking on too much at once. It can be very tempting to think:
“I will turn my life around, now! I’ll quit alcohol and animal products and sugar and refined grains, and I’ll go for a run each morning, and I’ll do this and that and there, I’ve got it, here is the blueprint for my healthy perfect life from this day forth!”
And, it’s great to have any and all of that as your end goal if you want, but please, pick one or two things at most to start with, focus on those, and when those have become second nature to you and just a normal part of your life, then choose the next thing to work on.
(You can plan out the whole thing in advance if you want! i.e., I’ll do this, then this, then this, but just… make sure that you’ve really got each one down to a matter of comfort and ease before you take up the next one)
In summary:
- Focus on adding health, whatever that looks like to you
- Figure out what “minimum effort!” is for you, and let that be your baseline
- Commit to yourself (and do any self-negotiation up-front, not later)
- Decide what you’re not going to do yet, and stick to that, too.
Share This Post
- How to get a beach body: take your body to a beach. Voilà. Beach body.
-

Fast Like A Girl – by Dr. Mindy Pelz
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of information out there when it comes to intermittent fasting is very much centered on men in the 25–35 years age range. What about the rest of us?
Our physiological needs are not the same, and it’d be foolhardy to ignore that. But what things do still stand the same, and what things would benefit from a different approach in our cases?
Dr. Pelz has our back with this book packed with information based on the best science currently out there. She gives a general overview of fasting with full consideration to the fact that we the reader may well be female or over a certain age or both. In addition, the book offers:
- Metabolic switching (the “missing key to weight loss”)
- Building a fasting lifestyle (that works with your actual life, not just on paper)
- How to time fasting according to your menstrual cycle (if you don’t have a cycle, she has you covered too)
- How to break a fast—properly (and many other hacks/tips/tricks to make fasting so much easier)
Bottom line: if you want to do intermittent fasting and want to work with rather than against your body, then this book is a fine option.
Share This Post
-

How To Stay In Shape At 70
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Questions and Answers at 10almonds
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
This newsletter has been growing a lot lately, and so have the questions/requests, and we love that! In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
I have a question: what are the pros and cons of older people (60+) taking creatine every day?
It depends what else you’re doing, as creatine mostly helps the muscles recover after exercise. So:
- iff you’re doing resistance training (such as weights or bodyweight training), or HIIT (High Intensity Interval Training), then creatine monohydrate may help you keep at that and keep doing well.
- if you’re just doing light-to-moderate exercises, you might not get much benefit from creatine!
The topic merits diving deeper though, so we’ll queue that for one of our “Research Review Monday” days!
I wanted to ask if you think marine collagen is decent to take. I’ve heard a lot of bad press about it
We don’t know what you’ve heard, but generally speaking it’s been found to be very beneficial to bones, joints, and skin! We wrote about it quite recently on a “Research Review Monday”:
See: We Are Such Stuff As Fish Are Made Of
Natural alternatives to medication for depression?
Great question! We did a mean feature a while back, but we definitely have much more to say! We’ll do another main feature soon, but in the meantime, here’s what we previously wrote:
See: The Mental Health First-Aid That You’ll Hopefully Never Need
^This covers not just the obvious, but also why the most common advice is not helpful, and practical tips to actually make manageable steps back to wellness, on days when “literally just survive the day” is one’s default goal.
I am now in the “aging” population. A great concern for me is Alzheimers. My father had it and I am so worried. What is the latest research on prevention?
One good thing to note is that while Alzheimer’s has a genetic component, it doesn’t appear to be hereditary per se. Still, good to be on top of these things, and it’s never too early to start with preventive measures!
You might like a main feature we did on this recently:
See: How To Reduce Your Alzheimer’s Risk
Side effects of statins, are they worth it? Depression, are antidepressants worth it?
About statins, that depends a lot on you, your circumstances, and—as it happens—your gender. We covered this in a main feature recently, but a short answer is: for most people, they may not be the best first choice, and could even make things worse. For some people, however, they really are just what’s needed.
- Factors that make them more likely better for you: being a man, or having atherosclerosis
- Factors that make them more likely worse for you: being a woman in general
Check out the main feature we did: Statins: His & Hers?
As for antidepressants? That depends a lot on you, your physiology, your depression, your circumstances, and more. We’ll definitely do a main feature on that sometime soon, as there’s a lot that most people don’t know!
I am interested in the following: Aging, Exercise, Diet, Relationships, Purpose, Lowering Stress
You’re going to love our Psychology Sunday editions of 10almonds!
You may particularly like some of these:
- Seriously Useful Communication Skills! ← this is about relationship stuff
- Lower Your Cortisol! (Here’s Why & How) ← about “the stress hormone”
- How To Set Your Anxiety Aside ← these methods work for stress too
(This coming Psychology Sunday will have a feature specifically on stress, so do make sure to read that when it comes out!)
Hair growth strategies for men combing caffeine and minoxidil?
Well, the strategy for that is to use caffeine and minoxidil! Some more specific tips, though:
- Both of those things need to be massaged (gently!) into your scalp especially around your hairline.
- In the case of caffeine, that boosts hair growth. No extra thought or care needed for that one.
- In the case of minoxidil, it reboots the hair growth cycle, so if you’ve only recently started, don’t be surprised (or worried) if you see more shedding in the first three months. It’s jettisoning your old hairs because new ones were just prompted (by the minoxidil) to start growing behind them. So: it will get briefly worse before it gets better, but then it’ll stay better… provided you keep using it.
- If you’d like other options besides minoxidil, finasteride is a commonly prescribed oral drug that blocks the conversion of testosterone to DHT, which latter is what tells your hairline to recede.
- If you’d like other options besides prescription drugs, saw palmetto performs comparably to finasteride (and works the same way).
- You may also want to consider biotin supplementation if you don’t already enjoy that
- Consider also using a dermaroller on your scalp. If you’re unfamiliar, this is a device that looks like a tiny lawn aerator, with many tiny needles, and you roll it gently across your skin.
- It can be used for promoting hair growth, as well as for reducing wrinkles and (more slowly) healing scars.
- It works by breaking up the sebum that may be blocking new hair growth, and also makes the skin healthier by stimulating production of collagen and elastin (in response to the thousands of microscopic wounds that the needles make).
- Sounds drastic, but it doesn’t hurt and doesn’t leave any visible marks—the needles are that tiny. Still, practise good sterilization and ensure your skin is clean when using it.
See: How To Use A Dermaroller ← also explains more of the science of it
PS: this question was asked in the context of men, but the information goes the same for women suffering from androgenic alepoceia—which is a lot more common than most people think!
How to get to sleep at night as fast and as naturally as possible? Thank you!
We’ll definitely write more on that! You might like these articles we wrote already, meanwhile:
- Beating The Insomnia Blues ← this one is general advice and tips
- Time For Some Pillow Talk ← this one compares and reviews some popular sleep apps
- Insomnia? High Blood Pressure? Try these! ← this one tackles the matter from a dietary angle
Q: How to be your best self after 60: Self motivation / Avoiding or limiting salt, sugar & alcohol: Alternatives / Ways to sneak in more movements/exercise
…and, from a different subscriber…
Q: Inflammation & over 60 weight loss. Thanks!
Here are some of our greatest hits on those topics:
- Where Nutrition Meets Habits ← focusing on food that’s all three of: healthy + easy + cheap
- How To Keep On Keeping On ← exercise tips for when the motivation wanes
- Keep Inflammation At Bay ← science-based tips and advice
Also, while we’ve recommended a couple of books on stopping (or reducing) drinking, we’ve not done a main feature on that, so we definitely will one of these days!
Share This Post
Related Posts
-
Quick Healthy Recipe Ideas
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
“It was superb !! Just loved that healthy recipe !!! I would love to see one of those every day, if possible !! Keep up the fabulous work !!! ”
We’re glad you enjoyed! We can’t promise a recipe every day, but here’s one just for you:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

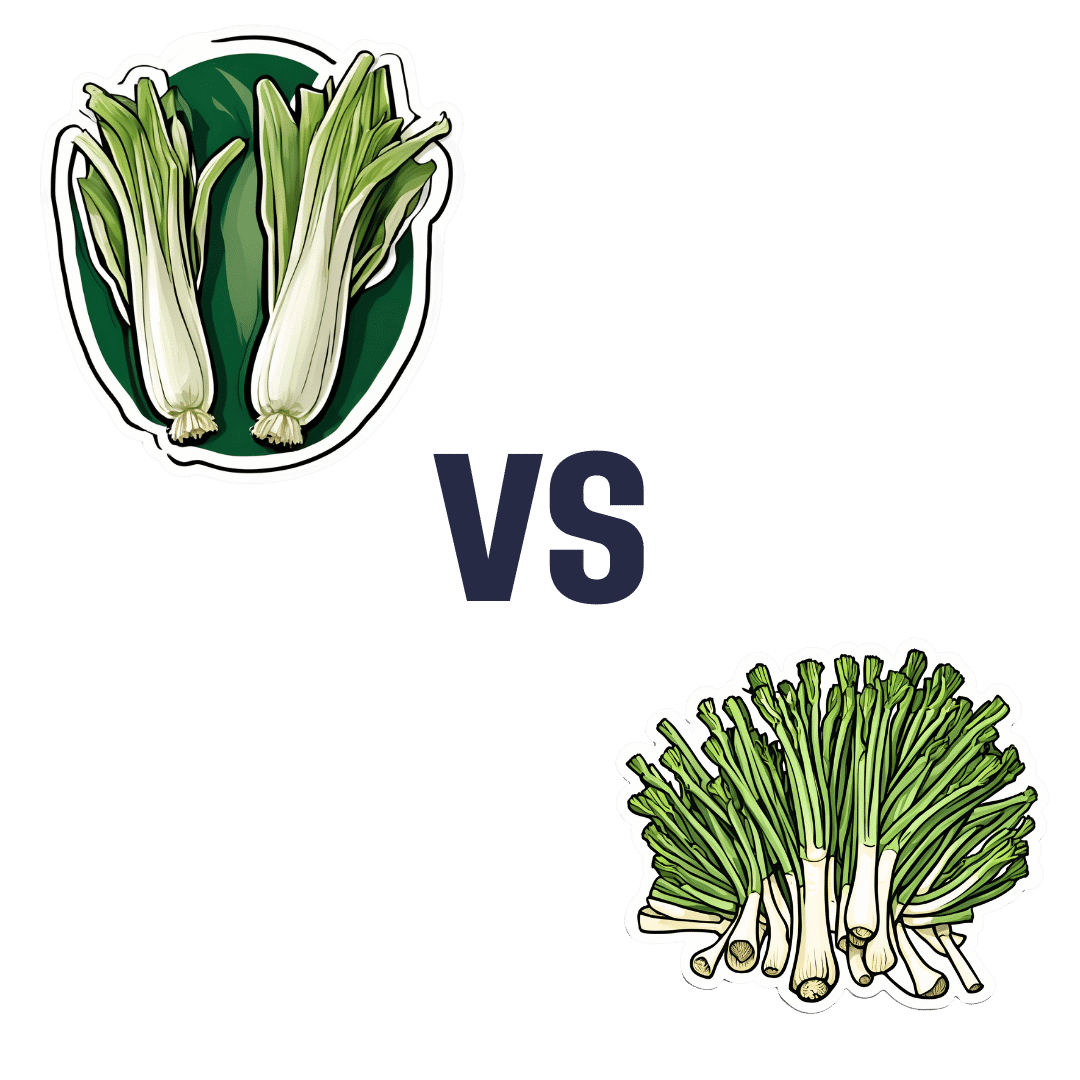
Leek vs Scallions – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing leek to scallions, we picked the leek.
Why?
In terms of macros, scallions might have a point: scallions have the lower glycemic index, thanks to leek having more carbs for the same amount of fiber. That said, leek already has a low glycemic index, so this is not a big deal.
When it comes to vitamins, leek has more of vitamins B1, B2, B3, B5, B6, B9, E, and choline, while scallions have more of vitamins A, C, and K. Noteworthily, a cup of chopped leek already provides the daily dose of vitamins A and K, and the difference in levels of vitamin C is minimal. All in all, an easy 8:3 win for leeks here, even without taking that into account.
In the category of minerals, leek has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and selenium, while scallions have a little more zinc.
Both of these allium-family plants (i.e., related to garlic) have an abundance of polyphenols, especially kaempferol.
Of course, enjoy whatever goes best with your meal, but if you’re looking for nutritional density, then leek is where it’s at.
Want to learn more?
You might like to read:
The Many Health Benefits Of Garlic
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Eat To Beat Chronic Fatigue!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Eat To Beat Chronic Fatigue
Chronic fatigue is on the rise, and it can make life a living Hell. Days blur into one, and you try to take each day as it comes, but sometimes several days gang up on you at once.
You probably know some lifestyle changes that might help—if only you had the energy to implement them.
You’d like to eat well, but you need to…
- Buy the fresh produce (and take a little rest after)
- Put the groceries away (and take a little rest after)
- Wash the vegetables (and take a little rest after)
- Chop the things as necessary (and take a little rest after)
- Cook dinner (and take a little rest after)
…and now you’re too exhausted to eat it.
So, what can be done?
First, avoid things that cause inflammation, as this is a major contributor to chronic fatigue. You might like our previous main feature:
Next up, really do stay hydrated. It’s less about quantity, and more about ubiquity. Hydrate often.
Best is if you always have some (hydrating) drink on the go.
Do experiment with your diet, and/but keep a food journal of what you eat and how you feel 30–60 minutes after eating it. Only make one change at a time, otherwise you won’t know which change made the difference.
Notice what patterns emerge over time, and adjust your ingredients accordingly.
Limit your caffeine intake. We know that sometimes it seems like the only way to get through the day, but you will always crash later, because it was only ever taxing your adrenal system (thus: making you more tired in the long run) and pulling the wool over the eyes of your adenosine receptors (blocking you from feeling how tired you are, but not actually reducing your body’s tiredness).
Put simply, caffeine is the “payday loan” of energy.
Eat more non-starchy vegetables, and enjoy healthy fats. Those healthy fats can come from nuts and seeds, avocado, or fish (not fried, though!).
The non-starchy vegetables will boost your vitamins and fiber while being easy on your beleaguered metabolism, while the healthy fats will perk up your energy levels without spiking insulin like sugars would.
Pay the fatigue tax up front. What this means is… Instead of throwing away vegetables that didn’t get used because it would take too much effort and you just need an easier dinner today, buy ready-chopped vegetables, for example.
And if you buy vegetables frozen, they’re also often not only cheaper, but also (counterintuitively) contain more nutrients.
A note of distinction:
Many more people have chronic fatigue (the symptom: being exhausted all the time) than have chronic fatigue syndrome (the illness: myalgic encephalomyelitis).
This is because fatigue can be a symptom of many, many other conditions, and can be heavily influenced by lifestyle factors too.
A lot of the advice for dealing with chronic fatigue is often the same in both cases, but some will be different, because for example:
- If your fatigue is from some other condition, that condition probably impacts what lifestyle factors you are (and are not) able to change, too
- If your fatigue is from lifestyle factors, that hopefully means you can change those and enjoy less fatigue…
- But if it’s not from lifestyle factors, as in ME/CFS, then advice to “exercise more” etc is not going to help so much.
There are ways to know the difference though:
Check out: Do You Have Chronic Fatigue Syndrome?
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: