Where Nutrition Meets Habits!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Where Nutrition Meets Habits…
This is Claudia Canu, MSc., INESEM. She’s on a mission to change the way we eat:
Often, diet is a case of…
- Healthy
- Easy
- Cheap
(choose two)
She wants to make it all three, and tasty too. She has her work cut out for her, but she’s already blazed quite a trail personally:
❝Nine months before turning 40 years old, I set a challenge for myself: Arrive to the day I turn 40 as the best possible version of myself, physically, mentally and emotionally.❞
~ Claudia Canu
In Her Own Words: My Journey To My Healthy 40s
And it really was quite a journey:
- September: Changes That Destabilize
- October: Looking for Focus
- November: New Habits
- December: Analyzing The First Results
- January: Traveling & Perfectionism
- February: Habits & Goals
- March: Connection, Cravings, & Organization
- April: Physical & Emotional Changes After 7 Months
- May: Reflections & Considerations
- June: Challenge Is Over
For those of us who’d like the short-cut rather than a nine-month quasi-spiritual journey… based on both her experience, and her academic and professional background in nutrition, her main priorities that she settled on were:
- Making meals actually nutritionally balanced, which meant re-thinking what she thought a meal “should” be
- Making nutritionally balanced meals that didn’t require a lot of skill and/or resources
- That’s it!
But, easier said than done… Where to begin?
She shares an extensive list of recipes, from meals to snacks (I thought I was the only one who made coffee overnight oats!), but the most important thing from her is:
Claudia’s 10 Guiding Principles:
- Buy only fresh ingredients that you are going to cook yourself. If you decide to buy pre-cooked ones, make sure they do not have added ingredients, especially sugar (in all its forms).
- Use easy and simple cooking methods.
- Change ingredients every time you prepare your meals.
- Prepare large quantities for three or four days.
- Store the food separately in tightly closed Tupperware.
- Organize yourself to always have ready-to-eat food in the fridge.
- When hungry, mix the ingredients in the ideal amounts to cover the needs of your body.
- Chew well and take the time to taste your food.
- Eat foods that you like and enjoy.
- Do not overeat but don’t undereat either.
We have only two quibbles with this fine list, which are:
About Ingredients!
Depending on what’s available around you, frozen and/or tinned “one-ingredient” foods can be as nutritional as (if not more nutritional than) fresh ones. By “one-ingredient” foods here we mean that if you buy a frozen pack of chopped onions, the ingredients list will be: “chopped onions”. If you buy a tin of tomatoes, the ingredients will say “Tomatoes” or at most “Tomatoes, Tomato Juice”, for example.
She does list the ingredients she keeps in; the idea that with these in the kitchen, you’ll never be in the position of “oh, we don’t have much in, I guess it’s a pizza delivery night” or “well there are some chicken nuggets at the back of the freezer”.
Check Out And Plan: 10 Types Of Ingredients You Should Always Keep In Your Kitchen
Here Today, Gone Tomorrow?
Preparing large quantities for three or four days can result in food for one or two days if the food is unduly delicious
But! Claudia has a remedy for that:
Read: How To Eliminate Food Cravings And What To Do When They Win
Anyway, there’s a wealth of resources in the above-linked pages, so do check them out!
Perhaps the biggest take-away is to ask yourself:
“What are my guiding principles when it comes to food?”
If you don’t have a ready answer, maybe it’s time to tackle that—whether Claudia’s way or your own!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Science of Nutrition – by Rhiannon Lambert

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
While there are a lot of conflicting dietary approaches out there, the science itself is actually fairly cohesive in most regards. This book does a lot of what we do here at 10almonds, and presents the science in a clear fashion without having any particular agenda to push.
The author is a nutritionist (BSc, MSc, RNutr) and therefore provides an up-to-date evidence-based approach for eating.
As a result, the only part of this book that brings it down in this reviewer’s opinion is the section on Intermittent Fasting. Being not strictly about nutrition, she has less expertise on that topic, and it shows.
The information is largely presented in double-page spreads each answering a particular question. Because of this, and the fact there are colorful graphic representations of information too, we do recommend the print version over Kindle*.
Bottom line: if you like the notion of real science being presented in a clear and simple fashion (we like to think our subscribers do!), then you’ll surely enjoy this book.
Click here to check out the Science of Nutrition, and get a clear overview!
*Writer’s note: I realize I’ve two days in a row recommended this (yesterday because there are checkboxes to check, worksheets to complete, etc), but it’s not a new trend; just how it happened to be with these two books. I love my Kindle dearly, but sometimes print has the edge for one reason or another!
Share This Post
-

Reduce Your Stroke Risk
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
❝Each year in the U.S., over half a million people have a first stroke; however, up to 80% of strokes may be preventable.❞
~ American Stroke Association
Source: New guideline: Preventing a first stroke may be possible with screening, lifestyle changes
So, what should we do?
Some of the risk factors are unavoidable or not usefully avoidable, like genetic predispositions and old age, respectively (i.e. it is possible to avoid old age—by dying young, which is not a good approach).
Some of the risk factors are avoidable. Let’s look at the most obvious first:
You cannot drink to your good health
While overall, the World Health Organization has declared that “the only safe amount of alcohol is zero”, when it comes to stroke risk specifically, it seems that low consumption is not associated with stroke, while moderate to high consumption is associated with a commensurately increased risk of stroke:
Alcohol Intake as a Risk Factor for Acute Stroke
Note: there are some studies out there that say that a low to moderate consumption may decrease the risk compared to zero consumption. However, any such study that this writer has seen has had the methodological flaw of not addressing why those who do not drink alcohol, do not drink it. In many cases, someone who drinks no alcohol at all does so because either a) it would cause problems with some medication(s) they are taking, or b) they used to drink heavily, and quit. In either case, their reasons for not drinking alcohol may themselves be reasons for an increased stroke risk—not the lack of alcohol itself.
Smoke now = stroke later
This one is straightforward; smoking is bad for pretty much everything, and that includes stroke risk, as it’s bad for your heart and brain both, increasing stroke risk by 200–400%:
Smoking and stroke: the more you smoke the more you stroke
So, the advice here of course is: don’t smoke
Diet matters
The American Stroke Association’s guidelines recommend, just for a change, the Mediterranean Diet. This does not mean just whatever is eaten in the Mediterranean region though, and there are specifically foods that are included and excluded, and the ratios matter, so here’s a run-down of what the Mediterranean Diet does and doesn’t include:
The Mediterranean Diet: What Is It Good For? ← what isn’t it good for?!
You can outrun stroke
Or out-walk it; that’s fine too. Most important here is frequency of exercise, more than intensity. So basically, getting those 150 minutes moderate exercise per week as a minimum.
See also: The Doctor Who Wants Us To Exercise Less & Move More
Which is good, because it means we can get a lot of exercise in that doesn’t feel like “having to do” exercise, for example:
Do You Love To Go To The Gym? No? Enjoy These “No-Exercise Exercises”!
Your brain needs downtime too
Your brain (and your heart) both need you to get good regular sleep:
Sleep Disorders in Stroke: An Update on Management
We sometimes say that “what’s good for your heart is good for your brain” (because the heart feeds the brain, and also ultimately clears away detritus), and that’s true here too, so we might also want to prioritize sleep regularity over other factors, even over duration:
How Regularity Of Sleep Can Be Even More Important Than Duration ← this is about adverse cardiovascular events, including ischemic stroke
Keep on top of your blood pressure
High blood pressure is a very modifiable risk factor for stroke. Taking care of the above things will generally take care of this, especially the DASH variation of the Mediterranean diet:
Hypertension: Factors Far More Relevant Than Salt
However, it’s still important to actually check your blood pressure regularly, because sometimes an unexpected extra factor can pop up for no obvious reason. As a bonus, you can do this improved version of the usual blood pressure test, still using just a blood pressure cuff:
Try This At Home: ABI Test For Clogged Arteries
Consider GLP-1 receptor agonists (or…)
GLP-1 receptor agonists (like Ozempic et al.) seem to have cardioprotective and neuroprotective (thus: anti-stroke) activity independent of their weight loss benefits:
Of course, GLP-1 RAs aren’t everyone’s cup of tea, and they do have their downsides (including availability, cost, and the fact benefits reverse themselves if you stop taking them), so if you want a similar effect from a natural approach, there are some foods that work on the body’s incretin responses in the same way as GLP-1 RAs do:
5 Foods That Naturally Mimic The “Ozempic Effect”
Better to know sooner rather than too late
Rather than waiting until one half of our face is drooping to know that there was a stroke risk, here are things to watch out for to know about it before it’s too late:
6 Signs Of Stroke (One Month In Advance)
Take care!
Share This Post
-

How we can prepare for future public health emergencies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
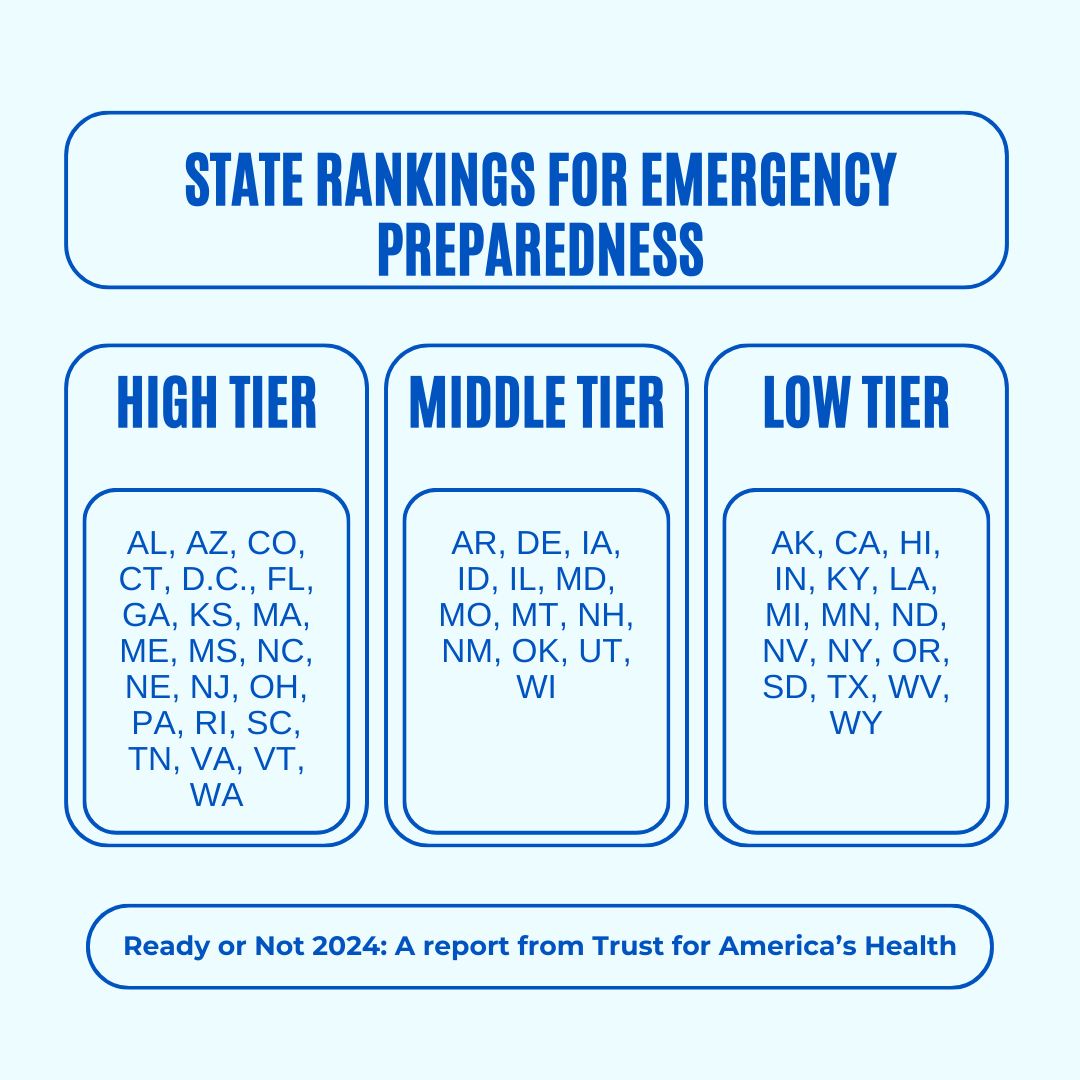
The U.S. is experiencing an increasing number of disease outbreaks and extreme weather events. While state and national preparedness for public health emergencies has improved in some areas, dangerous gaps remain, says a recent report from Trust for America’s Health.
Titled, “Ready or Not 2024: Protecting the Public’s Health from Diseases, Disasters, and Bioterrorism,” the report identifies gaps in national and state preparedness for public health emergencies and provides recommendations for improvement.
Using nine key indicators, the report categorizes all U.S. states and the District of Columbia into three readiness levels: high, medium, and low. The writers hope the report will help policymakers in under-performing states improve public health infrastructure.
Read on to learn more about what the research found and how we can individually prepare for future public health emergencies.
There’s work to be done

The report highlights areas with strong performance as well as those that need improvement.
Some areas with strong performance:
- State public health funding: Most states and the District of Columbia either maintained or increased their public health funding during the 2023 fiscal year.
- Health care labor force preparedness: Most states have started expanding the health care labor force for improved emergency response. As of 2023, 39 states participated in the Nurse Licensure Compact, which allows nurses to work in multiple member states without the need for additional state licenses.
Some areas that need improvement:
- Hospital safety scores: Only 25 percent of acute care hospitals earned the highest patient safety grade in fall 2023. These scores measure health care-associated infection rates, intensive care unit capacity, and other metrics. More high-scoring hospitals would improve preparedness for future public health emergencies.
- Access to paid time off: From March 2018 to March 2023, only 55 percent of U.S. workers used paid time off. Access to paid time off is important for reducing the spread of infectious diseases.
We can all do our part by staying up to date on vaccines
While the report focuses on policy changes that would improve emergency preparedness, Trust for America’s Health’s research identifies one way that we can individually prepare for future public health emergencies: staying up to date on vaccines.
The report found that during the 2022-2023 flu season, only 49 percent of those eligible for the flu vaccine received it. Public health experts are concerned that false claims about COVID-19 vaccines have resulted in overall vaccine hesitancy.
A decline in vaccination rates has led to an uptick in life-threatening, vaccine-preventable diseases, such as measles. Increasing vaccine uptake would prevent the spread of vaccine-preventable diseases and reduce strain on hospital systems during public health crises.
Make sure that you and your children have received all recommended vaccines to prevent severe illness, hospitalization, and death. Learn more about recommended vaccines for adults and children from the CDC.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post

Related Posts
-
Escape Self-Sabotage
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Stop Making The Same Mistakes
It’s easy to think that a self-destructive cycle is easy to avoid if you have no special will to self-destruction. However, the cycle is sneaky.
It’s sneaky because it can be passive, and/or omissions rather than actions, procrastinations rather than obvious acts of impulse, and so forth.
So, they’re often things that specifically aren’t there to see.
How to catch them
How often do you think “I wish I had [done xyz]” or “I wish I had [done yxz] sooner”?
Now, how often have you thought that about the same thing more than once? For example, “I should have kept up my exercise”.
For things like this, habit-trackers are a great way to, well, keep track of habits. If for example you planned to do a 10-minute exercise session daily but you’ve been postponing it since you got distracted on January the 2nd, then it’ll highlight that. See also:
How To Really Pick Up (And Keep!) Those Habits
Speaking of habits, this goes for other forms of procrastination, too. For example, if you are always slow to get medical check-ups, or renew your prescriptions, or get ready for some regularly-occurring thing in your schedule, then set a reminder in your preferred way (phone app, calendar on the wall, whatever) and when the appointed time arrives (to book the check-up, renew the prescription, do your taxes, whatever), do it on the day you set your reminder for, as a personal rule for you that you keep to, barring extreme calamity.
By “extreme calamity” we mean less “running late today” and more “house burned down”.
Digital traps
Bad habits can be insidious in other ways too, like getting sucked into social media scrolling (it is literally designed to do that to you; you are not immune modern programming hijacking evolutionary dopamine responses).
Setting a screentime limit (you can specify “just these apps” if you like) will help with this. On most devices, this feature includes a sticky notification in the notification bar, that’ll remind you “27 out of 30 minutes remaining” or whatever you set it for. That’ll remind you to do what you went there to do, instead of getting caught in the endless scroll (and if you went there to just browse, to do so briefly).
Here’s how to set that:
Instructions for iOS devices | Instructions for Android devices
Oh, and on the topic of social media? If you find yourself getting caught up in unproductive arguments on the Internet, try the three-response rule:
- You reply; they reply (no progress made)
- You reply; they reply (still no progress made)
- You reply; they reply (still yet no progress made)
You reply just one more time: “I have a personal rule that if I’m arguing on the Internet and no progress has been made after three replies, I don’t reply further—I find this is helpful to avoid a lot of time lost to pointless arguing that isn’t going anywhere. Best wishes.”
(and then stick to it, no matter how they try to provoke you; best is to just not look until at least the next day)
When “swept up in love” gets to one of those little whirlpools…
The same works in personal relationships, by the way. If for example you are arguing with a loved one and not making progress, it can be good if you both have a pre-arranged agreement that either of you can, up to once on any given day, invoke a “time-out” (e.g. 30 minutes, but you agree the time between you when you first make this standing policy) during which you will both keep out of the other’s way, and come back with a more productive head on (remembering that things go best when it’s you both vs the problem, rather than vs each other).
See also:
Seriously Useful Communication Skills: Conflict Resolution
What if the self-sabotaging cycle is active and apparent?
Well, that is less sneaky, but certainly no less serious, and sometimes moreso. An obvious example is drinking too much; this is often cyclical in nature. We wrote about this one previously:
That article’s alcohol-specific, but the same advices go for other harmful activities, including other substance abuse (which in turn includes binge-eating), as well psychological addictions (such as gambling, for example).
Finally…
If your destructive cycle is more of a rut you’ve got stuck in, a common advice is to change something, anything, to get out of the rut.
That can be very bad advice! Because sometimes the change you go for is absolutely not the change that was needed, and is rather just cracking under pressure and doing something impulsive.
Here’s one way to actively get out of a slump:
Behavioral Activation Against Depression & Anxiety
Note: you do not have to be depressed or anxious to do this. But the point is, it’s a tool you can use even if you are depressed and/or anxious, so it’s a good thing to try for getting out of most kinds of slumps.
And really finally, here’s a resource for, well, the title speaks for itself:
When You Know What You “Should” Do (But Knowing Isn’t The Problem)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Radical Remission – by Dr. Kelly Turner
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this is not:an autobiographical account of the “I beat cancer and you can too” pep-talk style.
What it is: a very readable pop-science book based on the author’s own PhD research into radical remission.
She knew that a very small percentage of people experience spontaneous radical remission (or quasi-spontaneous, if the remission is attributed to lifestyle changes, and/or some alternative therapy), but a small percentage of people means a large number worldwide, so she travelled the world studying over 1,000 cases of people with late-stage cancer who had either not gone for conventional anticancer drugs, or had and then stopped, and lived to tell the tale.
While she doesn’t advocate for any particular alternative therapy, she does report on what things came to her attention. She does advocate for some lifestyle changes.
Perhaps the biggest value this book offers is in its promised “9 key factors that can make a real difference”, which are essentially her conclusions from her PhD dissertation.
There isn’t room to talk about them here in a way that wouldn’t be misleading/unhelpful for a paucity of space, so perhaps we’ll do a main feature one of these days.
Bottom line: if you have (or a loved one has) cancer, this is an incredibly sensible book to read. If you don’t, then it’s an interesting and thought-provoking book to read.
Click here to check out Radical Remission, and learn about the factors at hand!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Kiwi vs Lemon – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kiwi to lemon, we picked the kiwi.
Why?
A fairly straightforward one today!
In terms of macros, kiwi has more protein, carbs, and fiber, the ratio of the latter two also giving it the lower glycemic index. An easy win for kiwi here.
In the category of vitamins, kiwi has more of vitamins A, B2, B3, B9, C, E, K, and choline, while lemon has more of vitamins B1 and B6. Yes, that’s right, lemon didn’t even win on the vitamin C that it’s famous for. In any case, a clear 8:2 win for kiwi.
Looking at minerals, kiwi has more calcium, copper, magnesium, manganese, phosphorus, potassium, and zinc, while lemon has more iron and selenium. So, looking at this 7:2 win for kiwi, you might want to reconsider that “glass of lemon water to replenish minerals” trend!
None of this is to knock lemons, by the way; lemons are still a very respectable fruit, nutritionally. Probably very few people are out there eating lemons the way one might eat kiwi…
(writer’s note: I say “very few”, as once upon a time when my son was small, I remember coming into the kitchen to find he had helped himself to lemon wedges and was just eating them, so it can happen. But I also one time when he was just as small, found him drinking hot sauce directly from the bottle, so hey, he clearly already enjoyed strong flavors. Lest I seem a very inattentive mother, I’ll say in my defense that our kitchen has no real toddler-height hazards when the oven is cold, and those items were from the bottom of the fridge, so easy to access if I leave the room for a moment to grab something)
…but what we do want to say here is: if you don’t care for lemons so much, you’re not missing out. If the lemon water isn’t calling to you, you can skip it guilt-free.
In any case, do enjoy either or both, but kiwi’s the clear winner here!
Want to learn more?
You might like to read:
Top 8 Fruits That Prevent & Kill Cancer ← kiwi is top of the list! It has some cool properties, as you’ll see, killing cancer cells while sparing healthy ones.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: