The Connection Cure – by Julia Hotz
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may recognize some of the things in the subtitle as being notable elements of the Blue Zones supercentenarians’ lifestyles, but this book looks at numerous quite diverse countries, and people from many walks of life.
What they have in common—and this is mostly a very person-centered book, relying a lot on case studies, with additional references coming from wider sociological data—is social prescribing.
What is social prescribing? That’s what the author (a journalist by general profession) answers comprehensively here, and it’s about looking at the ways medical problems can often have nonmedical solutions. It doesn’t necessarily mean that walking will cure your cancer or art will cure your diabetes, but it does mean that very often a key part of an unhealthy lifestyle is fundamentally something that can be fixed by one or more of: movement, nature, art, service, and belonging.
She looks at social prescribing in its birthplace (the UK, where cheap solutions that are nevertheless evidence-based are very much prioritized), in big countries like Canada and Australia, in aging countries like Singapore and South Korea, and yes, also in the #1 country of pill prescribing, the US.
The structure of the book is interesting, we first have 5 person-centered chapters addressing each of the social prescribing aspects and how they helped in two example case studies for each one, then 5 country-by-country epidemiological chapters looking at the big picture, then 5 person-centered chapters again, this time looking at personalizing social prescribing for oneself (this section of the book being headed “Social Prescribing For You And Me”), looking at what is going on in one’s life and health, which of the 5 elements might be missing, and what tangible goal-oriented benefits can—according to the evidence—be obtained by tending to what one actually needs in terms of social prescribing.
The style is narrative and journalistic, with very little hard science, but very little that’s wishy-washy either. It is, in short, a pleasant and informative read that helps the reader really understand social prescribing, the better to implement it in our own lives.
Bottom line: if you like having extra nonmedical approaches to avoid or alleviate medical problems, then this book will really help you achieve that.
Click here to check out The Connection Cure, and get social prescribing!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Resveratrol & Healthy Aging

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Resveratrol & Healthy Aging
Resveratrol is the compound found in red grapes, and thus in red wine, that have resulted in red wine being sometimes touted as a heart-healthy drink.
However, at the levels contained in red wine, you’d need to drink 100–1000 glasses of wine per day (depending on the wine) to get the dose of resveratrol that was associated with heart health benefits in mouse studies.
Which also means: if you are not a mouse, you might need to drink even more than that!
Further reading: can we drink to good health?
Resveratrol supplementation
Happily, resveratrol supplements exist. But what does resveratrol do?
It lowers blood pressure:
Effect of resveratrol on blood pressure: a meta-analysis of randomized controlled trials
It improves blood lipid levels:
It improves insulin sensitivity:
It has neuroprotective effects too:
Resveratrol promotes clearance of Alzheimer’s disease amyloid-beta peptides
Is it safe?
For most people, it is generally recognized as safe. However, if you are on blood-thinners or otherwise have a bleeding disorder, you might want to skip it:
Antiplatelet activity of synthetic and natural resveratrol in red wine
You also might want to check with your pharmacist/doctor, if you’re on blood pressure meds, anxiety meds, or immunosuppressants, as it can increase the amount of these drugs that will then stay in your system:
Resveratrol modulates drug- and carcinogen-metabolizing enzymes in a healthy volunteer study
And as ever, of course, if unsure just check with your pharmacist/doctor, to be on the safe side.
Where to get it?
We don’t sell it, but here’s an example product on Amazon for your convenience
Enjoy!
Share This Post
-

The Imperfect Nutritionist – by Jennifer Medhurst
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The idea of the “imperfect nutritionist” is to note that we’re all different with slightly different needs and sometimes very different preferences (or circumstances!) and having a truly perfect diet is probably a fool’s errand. Should we just give up, then? Not at all:
What we can do, Medhust argues, is find what’s best for us, realistically.
It’s better to have an 80% perfect diet 80% of the time, than to have a totally perfect diet for four and a half meals before running out of steam (and ingredients).
As for the “seven principles” mentioned in the title… we’re not going to keep those a mystery; they are:
- Focusing on wholefood
- Being diverse
- Knowing your fats
- Including fermented, prebiotic and probiotic foods
- Reducing refined carbohydrates
- Being aware of liquids
- Eating mindfully
The first part of the book is a treatise on how to implement those principles in your diet generally; the second part of the book is a recipe collection—70 recipes, with “these ingredients will almost certainly be available at your local supermarket” as a baseline. No instances of “the secret to being a good chef is knowing how to source fresh ingredients; ask your local greengrocer where to find spring-harvested perambulatory truffle-cones” here!
Basically, it focusses on adding healthy foods per your personal preferences and circumstances, and building these up into a repertoire of meals that will keep you and your family happy and healthy.
Pick Up Your Copy Of The Imperfect Nutritionist From Amazon Today!
Share This Post
-

How To Nap Like A Pro (No More “Sleep Hangovers”!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Be An Expert Nap-Artist
There’s a lot of science to say that napping can bring us health benefits—but mistiming it can just make us more tired. So, how to get some refreshing shut-eye, without ending up with a case of the midday melatonin blues?
First, why do we want to nap?
Well, maybe we’re just tired, but there are specific benefits even if we’re not. For example:
- Increased alertness
- Helps with learning
- Improved memory
- Boost to immunity
- Enhance athletic performance
What can go wrong?
There are two main things that can go wrong, physiologically speaking:
- We can overdo it, and not sleep well at night
- We can awake groggy and confused and tired
The first is self-explanatory—it messes with the circadian rhythm. For this reason, we should not sleep more than 90 minutes during the day. If that seems like a lot, and maybe you’ve heard that we shouldn’t sleep more than half an hour, there is science here, so read on…
The second is a matter of sleep cycles. Our brain naturally organizes our sleep into multiples of 20-minute segments, with a slight break of a few minutes between each. Consequently, naps should be:
- 25ish minutes
- 40–45 minutes
- 90ish minutes
If you wake up mid-cycle—for example, because your alarm went off, or someone disturbed you, or even because you needed to pee, you will be groggy, disoriented, and exhausted.
For this reason, a nap of one hour (a common choice, since people like “round” numbers) is a recipe for disaster, and will only work if you take 15 minutes to fall asleep. In which case, it’d really be a nap of 45 minutes, made up of two 20-minute sleep cycles.
Some interruptions are better/worse than others
If you’re in light or REM sleep, a disruption will leave you not very refreshed, but not wiped out either. And as a bonus, if you’re interrupted during a REM cycle, you’re more likely to remember your dreams.
If you’re in deep sleep, a disruption will leave you with what feels like an incredible hangover, minus the headache, and you’ll be far more tired than you were before you started the nap.
The best way to nap
Taking these factors into account, one of the “safest” ways to nap is to set your alarm for the top end of the time-bracket above the one you actually want to nap for (e.g., if you want to nap for 25ish minutes, set your alarm for 45).
Unless you’re very sleep-deprived, you’ll probably wake up briefly after 20–25 minutes of sleep. This may seem like nearer 30 minutes, if it took you some minutes to fall asleep!
If you don’t wake up then, or otherwise fail to get up, your alarm will catch you later at what will hopefully be between your next sleep cycles, or at the very least not right in the middle of one.
When you wake up from a nap before your alarm, get up. This is not the time for “5 more minutes” because “5 more minutes” will never, ever, be refreshing.
Rest well!
Share This Post
Related Posts
-

Avoiding/Managing Osteoarthritis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Avoiding/Managing Osteoarthritis
Arthritis is the umbrella term for a cluster of joint diseases involving inflammation of the joints, hence “arthr-” (joint) “-itis” (suffix used to denote inflammation).
Inflammatory vs Non-Inflammatory Arthritis
Arthritis is broadly divided into inflammatory arthritis and non-inflammatory arthritis.
Some forms, such as rheumatoid arthritis, are of the inflammatory kind. We wrote about that previously:
See: Avoiding/Managing Rheumatoid Arthritis
You may be wondering: how does one get non-inflammatory inflammation of the joints?
The answer is, in “non-inflammatory” arthritis, such as osteoarthritis, the damage comes first (by general wear-and-tear) and inflammation generally follows as part of the symptoms, rather than the cause.
So the name can be a little confusing. In the case of osteo- and other “non-inflammatory” forms of arthritis, you definitely still want to keep your inflammation at bay as best you can; it’s just not the prime focus.
So, what should we focus on?
First and foremost: avoiding wear-and-tear if possible. Naturally, we all must live our lives, and sometimes that means taking a few knocks, and definitely it means using our joints. An unused joint would suffer just as much as an abused one. But, we can take care of our joints!
We wrote on that previously, too:
See: How To Really Look After Your Joints
New osteoarthritis medication (hot off the press!)
At 10almonds, we try to keep on top of new developments, and here’s a shiny new one from this month:
- Methotrexate to treat hand osteoarthritis with synovitis (12th Oct, clinical trial)
- New research has found an existing drug could help many people with painful hand osteoarthritis (24th Oct, pop-science article about the above, but still written by one of the study authors!)
Note also that Dr. Flavia Cicuttini there talks about what we talked about above—that calling it non-inflammatory arthritis is a little misleading, as the inflammation still occurs.
And finally…
You might consider other lifestyle adjustments to manage your symptoms. These include:
- Exercise—gently, though!
- Rest—while keeping mobility going.
- Mobility aids—if it helps, it helps.
- Go easy on the use of braces, splints, etc—these can offer short-term relief, but at a long term cost of loss of mobility.
- Only you can decide where to draw the line when it comes to that trade-off.
You can also check out our previous article:
See: Managing Chronic Pain (Realistically!)
Take good care of yourself!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is Chiropractic All It’s Cracked Up To Be?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is Chiropractic All It’s Cracked Up To Be?

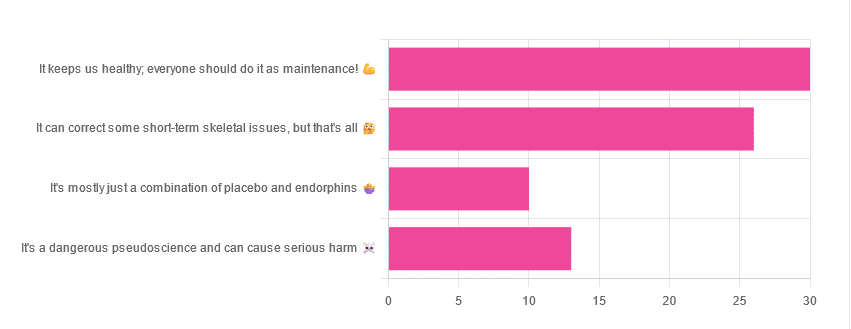
Yesterday, we asked you for your opinions on chiropractic medicine, and got the above-depicted, below-described set of results:
- 38% of respondents said it keeps us healthy, and everyone should do it as maintenance
- 33% of respondents said it can correct some short-term skeletal issues, but that’s all
- 16% of respondents said that it’s a dangerous pseudoscience and can cause serious harm
- 13% of respondents said that it’s mostly just a combination of placebo and endorphins
Respondents also shared personal horror stories of harm done, personal success stories of things cured, and personal “it didn’t seem to do anything for me” stories.
What does the science say?
It’s a dangerous pseudoscience and can cause harm: True or False?
False and True, respectively.
That is to say, chiropractic in its simplest form that makes the fewest claims, is not a pseudoscience. If somebody physically moves your bones around, your bones will be physically moved. If your bones were indeed misaligned, and the chiropractor is knowledgeable and competent, this will be for the better.
However, like any form of medicine, it can also cause harm; in chiropractic’s case, because it more often than not involves manipulation of the spine, this can be very serious:
❝Twenty six fatalities were published in the medical literature and many more might have remained unpublished.
The reported pathology usually was a vascular accident involving the dissection of a vertebral artery.
Conclusion: Numerous deaths have occurred after chiropractic manipulations. The risks of this treatment by far outweigh its benefit.❞
Source: Deaths after chiropractic: a review of published cases
From this, we might note two things:
- The abstract doesn’t note the initial sample size; we would rather have seen this information expressed as a percentage. Unfortunately, the full paper is not accessible, and nor are many of the papers it cites.
- Having a vertebral artery fatally dissected is nevertheless not an inviting prospect, and is certainly a very reasonable cause for concern.
It’s mostly just a combination of placebo and endorphins: True or False?
True or False, depending on what you went in for:
- If you went in for a regular maintenance clunk-and-click, then yes, you will get your clunk-and-click and feel better for it because you had a ritualized* experience and endorphins were released.
- If you went in for something that was actually wrong with your skeletal alignment, to get it corrected, and this correction was within your chiropractor’s competence, then yes, you will feel better because a genuine fault was corrected.
*this is not implying any mysticism, by the way. Rather it means simply that placebo effect is strongest when there is a ritual associated with it. In this case it means going to the place, sitting in a pleasant waiting room, being called in, removing your shoes and perhaps some other clothes, getting the full attention of a confident and assured person for a while, this sort of thing.
With regard to its use to combat specifically spinal pain (i.e., perhaps the most obvious thing to treat by chiropractic spinal manipulation), evidence is slightly in favor, but remains unclear:
❝Due to the low quality of evidence, the efficacy of chiropractic spinal manipulation compared with a placebo or no treatment remains uncertain. ❞
Source: Clinical Effectiveness and Efficacy of Chiropractic Spinal Manipulation for Spine Pain
It can correct some short-term skeletal issues, but that’s all: True or False?
Probably True.
Why “probably”? The effectiveness of chiropractic treatment for things other than short-term skeletal issues has barely been studied. From this, we may wish to keep an open mind, while also noting that it can hardly claim to be evidence-based—and it’s had hundreds of years to accumulate evidence. In all likelihood, publication bias has meant that studies that were conducted and found inconclusive or negative results were simply not published—but that’s just a hypothesis on our part.
In the case of using chiropractic to treat migraines, a very-related-but-not-skeletal issue, researchers found:
❝Pre-specified feasibility criteria were not met, but deficits were remediable. Preliminary data support a definitive trial of MCC+ for migraine.❞
Translating this: “it didn’t score as well as we hoped, but we can do better. We got some positive results, and would like to do another, bigger, better trial; please fund it”
Source: Multimodal chiropractic care for migraine: A pilot randomized controlled trial
Meanwhile, chiropractors’ claims for very unrelated things have been harshly criticized by the scientific community, for example:
Misinformation, chiropractic, and the COVID-19 pandemic
About that “short-term” aspect, one of our subscribers put it quite succinctly:
❝Often a skeletal correction is required for initial alignment but the surrounding fascia and muscles also need to be treated to mobilize the joint and release deep tissue damage surrounding the area. In combination with other therapies chiropractic support is beneficial.❞
This is, by the way, very consistent with what was said in the very clinically-dense book we reviewed yesterday, which has a chapter on the short-term benefits and limitations of chiropractic.
A truism that holds for many musculoskeletal healthcare matters, holds true here too:
❝In a battle between muscle and bone, muscle will always win❞
In other words…
Chiropractic can definitely help put misaligned bones back where they should be. However, once they’re there, if the cause of their misalignment is not treated, they will just re-misalign themselves shortly after you walking out of your session.
This is great for chiropractors, if it keeps you coming back for endless appointments, but it does little for your body beyond give you a brief respite.
So, by all means go to a chiropractor if you feel so inclined (and you do not fear accidental arterial dissection etc), but please also consider going to a physiotherapist, and potentially other medical professions depending on what seems to be wrong, to see about addressing the underlying cause.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Surprising Link Between Type 2 Diabetes & Alzheimer’s
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Surprising Link Between Type 2 Diabetes & Alzheimer’s

This is Dr. Rhonda Patrick. She’s a biomedical scientist with expertise in the areas of aging, cancer, and nutrition. In the past five years she has expanded her research of aging to focus more on Alzheimer’s and Parkinson’s, as she has a genetic predisposition to both.
What does that genetic predisposition look like? People who (like her) have the APOE-ε4 allele have a twofold increased risk of Alzheimer’s disease—and if you have two copies (i.e., one from each of two parents), the risk can be up to tenfold. Globally, 13.7% of people have at least one copy of this allele.
So while getting Alzheimer’s or not is not, per se, hereditary… The predisposition to it can be passed on.
What’s on her mind?
Dr. Patrick has noted that, while we don’t know for sure the causes of Alzheimer’s disease, and can make educated guesses only from correlations, the majority of current science seems to be focusing on just one: amyloid plaques in the brain.
This is a worthy area of research, but ignores the fact that there are many potential Alzheimer’s disease mechanisms to explore, including (to count only mainstream scientific ideas):
- The amyloid hypothesis
- The tau hypothesis
- The inflammatory hypothesis
- The cholinergic hypothesis
- The cholesterol hypothesis
- The Reelin hypothesis
- The large gene instability hypothesis
…as well as other strongly correlated factors such as glucose hypometabolism, insulin signalling, and oxidative stress.
If you lost your keys and were looking for them, and knew at least half a dozen places they might be, how often would you check the same place without paying any attention to the others?
To this end, she notes about those latter-mentioned correlated factors:
❝50–80% of people with Alzheimer’s disease have type 2 diabetes; there is definitely something going on❞
There’s another “smoking gun” for this too, because dysfunction in the blood vessels and capillaries that line the blood-brain barrier seem to be a very early event that is common between all types of dementia (including Alzheimer’s) and between type 2 diabetes and APOE-ε4.
Research is ongoing, and Dr. Patrick is at the forefront of that. However, there’s a practical take-away here meanwhile…
What can we do about it?
Dr. Patrick hypothesizes that if we can reduce the risk of type 2 diabetes, we may reduce the risk of Alzheimer’s with it.
Obviously, avoiding diabetes if possible is a good thing to do anyway, but if we’re aware of an added risk factor for Alzheimer’s, it becomes yet more important.
Of course, all the usual advices apply here, including a Mediterranean diet and regular moderate exercise.
Three other things Dr. Patrick specifically recommends (to reduce both type 2 diabetes risk and to reduce Alzheimer’s risk) include:
(links are to her blog, with lots of relevant science for each)
You can also hear more from Dr. Patrick personally, as a guest on Dr. Peter Attia’s podcast recently. She discusses these topics in much greater detail than we have room for in our newsletter:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: