Can We Drink To Good Health?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Can we drink to good health?
We asked you for your thoughts on alcohol and heart health, and we got quite an even spread of results!
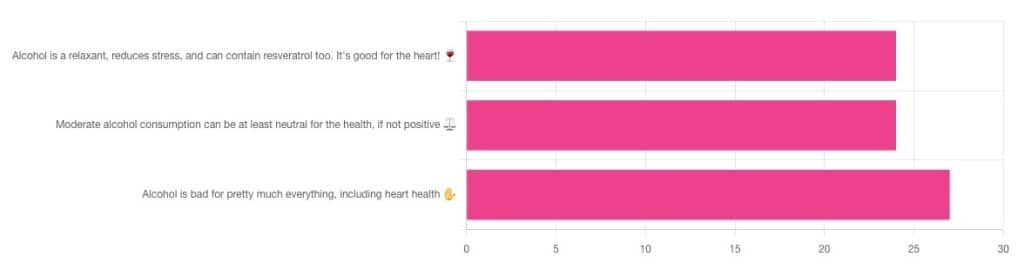
If perchance that’s too tiny to read, the figures were:
- 32% voted for “Alcohol is a relaxant, reduces stress, and can contain resveratrol too. It’s good for the heart!”
- 32% voted for: “Moderate alcohol consumption can be at least neutral for the health, if not positive ⚖️”
- 36% voted for: “Alcohol is bad for pretty much everything, including heart health ✋”
One subscriber who voted for “Alcohol is a relaxant, reduces stress, and can contain resveratrol too. It’s good for the heart!” added the following thoughts:
❝While it isn’t necessary to consume alcohol, moderate amounts can be beneficial and contribute to well-being through social activity, celebrations, etc.❞
That’s an interesting point, and definitely many people do see alcohol that way! Of course, that does not mean that one will find no social activities, celebrations, etc, in parts of the world where alcohol consumption is uncommon. Indeed, in India, wedding parties where no alcohol is consumed can go on for days!
But, “we live in a society” and all that, and while we’re a health newsletter not a social issues newsletter, it’d be remiss of us to not acknowledge the importance of socialization for good mental health—and thus the rest of our health too.
So, if indeed all our friends and family drink alcohol, it can certainly make abstaining more of a challenge.
On that note, let’s take a moment to consider “The French Paradox” (an observation of a low prevalence of ischemic heart disease despite high intakes of saturated fat, a phenomenon accredited to the consumption of red wine).
As it happens, a comprehensive review in “Circulation”, a cardiovascular health journal, has suggested the French Paradox may not be so paradoxical after all.
Research suggests it has more to do with other lifestyle factors (and historic under-reporting of cardiovascular disease by French doctors), which would explain why Japan has lower rates of heart disease, despite drinking little wine, and more beer and spirits.
So, our subscriber’s note may not be completely without reason! It’s just about the party, not the alcohol.
One subscriber who voted for “Moderate alcohol consumption can be at least neutral for the health, if not positive ⚖️” wrote:
❝Keeping in mind, moderate means one glass of wine for women a day and two for men. Hard alcohol doesn’t have the same heart benefits as wine❞
That is indeed the guideline according to some health bodies!
In other places with different guiding advisory bodies, that’s been dropped down to one a day for everyone (the science may be universal, but how government institutions interpret that is not).
About that wine… Specifically, red wine, for its resveratrol content:
While there are polyphenols such as resveratrol in red wine that could boost heart health, there’s so little per glass that you may need 100–1000 glasses to get the dosage that provides benefits in mouse studies. If you’re not a mouse, you might even need more.
To this end, many people prefer resveratrol supplementation. ← link is to an example product, but there are plenty more so feel free to shop around
A subscriber who voted for “Alcohol is bad for pretty much everything, including heart health ✋” says:
❝New guidelines suggest 1 to 2 drinks a week are okay but the less the better.❞
If you haven’t heard these new guidelines, we’ll mention again: every government has its own official bodies and guidelines so perhaps your local guidelines differ, but for example here’s what that World Health Organization has to say (as of January this year):
WHO: No level of alcohol consumption is safe for our health
So, whom to believe? The governments who hopefully consider the welfare of their citizenry more important than the tax dollars from alcohol sales, or the World Health Organization?
It’s a tough one, but we’ll always err on the side of the science.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Subtle Art of Not Giving a F*ck – by Mark Manson

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may wonder from the title: is this book arguing that we should all be callous heartless monsters? And no, it is not.
Instead, author Mark Manson advocates for cynicism, but less in the manner of Scrooge, and more in the manner of Diogenes:
- That life will involve struggle, so we might as well at least choose our struggles.
- That we will make mistakes, so we might as well accept them as learning experiences.
- That we will love and we will lose, so we might as well do it right while we can.
In short, the book is less about not caring… And more about caring about the right things only.
So, what are “the right things”? Manson bids us decide for ourselves, but certainly has ideas and pointers, with regard to what may or may not be healthy values to pursue.
The style throughout is casual and almost conversational, without being overly padded. It makes for very easy reading.
If the book has a weak point, it’s that when it briefly makes a suprisingly prescriptive turn into recommending we take up Buddhism, it may feel a bit like our friend who wants us to join in the latest MLM scheme. But, he’s soon back on track.
Bottom line: if you ever find yourself stressed with living up to unwanted expectations—your own, other people’s, and society’s—this book can really help streamline things.
Share This Post
-

This salt alternative could help reduce blood pressure. So why are so few people using it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One in three Australian adults has high blood pressure (hypertension). Excess salt (sodium) increases the risk of high blood pressure so everyone with hypertension is advised to reduce salt in their diet.
But despite decades of strong recommendations we have failed to get Australians to cut their intake. It’s hard for people to change the way they cook, season their food differently, pick low-salt foods off the supermarket shelves and accept a less salty taste.
Now there is a simple and effective solution: potassium-enriched salt. It can be used just like regular salt and most people don’t notice any important difference in taste.
Switching to potassium-enriched salt is feasible in a way that cutting salt intake is not. Our new research concludes clinical guidelines for hypertension should give patients clear recommendations to switch.
What is potassium-enriched salt?
Potassium-enriched salts replace some of the sodium chloride that makes up regular salt with potassium chloride. They’re also called low-sodium salt, potassium salt, heart salt, mineral salt, or sodium-reduced salt.
Potassium chloride looks the same as sodium chloride and tastes very similar.
Potassium-enriched salt works to lower blood pressure not only because it reduces sodium intake but also because it increases potassium intake. Insufficient potassium, which mostly comes from fruit and vegetables, is another big cause of high blood pressure.
What is the evidence?
We have strong evidence from a randomised trial of 20,995 people that switching to potassium-enriched salt lowers blood pressure and reduces the risks of stroke, heart attacks and early death. The participants had a history of stroke or were 60 years of age or older and had high blood pressure.
An overview of 21 other studies suggests much of the world’s population could benefit from potassium-enriched salt.
The World Health Organisation’s 2023 global report on hypertension highlighted potassium-enriched salt as an “affordable strategy” to reduce blood pressure and prevent cardiovascular events such as strokes.
What should clinical guidelines say?
We teamed up with researchers from the United States, Australia, Japan, South Africa and India to review 32 clinical guidelines for managing high blood pressure across the world. Our findings are published today in the American Heart Association’s journal, Hypertension.
We found current guidelines don’t give clear and consistent advice on using potassium-enriched salt.
While many guidelines recommend increasing dietary potassium intake, and all refer to reducing sodium intake, only two guidelines – the Chinese and European – recommend using potassium-enriched salt.
To help guidelines reflect the latest evidence, we suggested specific wording which could be adopted in Australia and around the world:

Recommended wording for guidance about the use of potassium-enriched salt in clinical management guidelines. Why do so few people use it?
Most people are unaware of how much salt they eat or the health issues it can cause. Few people know a simple switch to potassium-enriched salt can help lower blood pressure and reduce the risk of a stroke and heart disease.
Limited availability is another challenge. Several Australian retailers stock potassium-enriched salt but there is usually only one brand available, and it is often on the bottom shelf or in a special food aisle.
Potassium-enriched salts also cost more than regular salt, though it’s still low cost compared to most other foods, and not as expensive as many fancy salts now available.
It looks and tastes like normal salt.
Jimmy Dean/UnsplashA 2021 review found potassium-enriched salts were marketed in only 47 countries and those were mostly high-income countries. Prices ranged from the same as regular salt to almost 15 times greater.
Even though generally more expensive, potassium-enriched salt has the potential to be highly cost effective for disease prevention.
Preventing harm
A frequently raised concern about using potassium-enriched salt is the risk of high blood potassium levels (hyperkalemia) in the approximately 2% of the population with serious kidney disease.
People with serious kidney disease are already advised to avoid regular salt and to avoid foods high in potassium.
No harm from potassium-enriched salt has been recorded in any trial done to date, but all studies were done in a clinical setting with specific guidance for people with kidney disease.
Our current priority is to get people being managed for hypertension to use potassium-enriched salt because health-care providers can advise against its use in people at risk of hyperkalemia.
In some countries, potassium-enriched salt is recommended to the entire community because the potential benefits are so large. A modelling study showed almost half a million strokes and heart attacks would be averted every year in China if the population switched to potassium-enriched salt.
What will happen next?
In 2022, the health minister launched the National Hypertension Taskforce, which aims to improve blood pressure control rates from 32% to 70% by 2030 in Australia.
Potassium-enriched salt can play a key role in achieving this. We are working with the taskforce to update Australian hypertension management guidelines, and to promote the new guidelines to health professionals.
In parallel, we need potassium-enriched salt to be more accessible. We are engaging stakeholders to increase the availability of these products nationwide.
The world has already changed its salt supply once: from regular salt to iodised salt. Iodisation efforts began in the 1920s and took the best part of 100 years to achieve traction. Salt iodisation is a key public health achievement of the last century preventing goitre (a condition where your thyroid gland grows larger) and enhancing educational outcomes for millions of the poorest children in the world, as iodine is essential for normal growth and brain development.
The next switch to iodised and potassium-enriched salt offers at least the same potential for global health gains. But we need to make it happen in a fraction of the time.

Xiaoyue Xu (Luna), Scientia Lecturer, UNSW Sydney; Alta Schutte, SHARP Professor of Cardiovascular Medicine, UNSW Sydney, and Bruce Neal, Executive Director, George Institute Australia, George Institute for Global Health
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Why is pain so exhausting?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One of the most common feelings associated with persisting pain is fatigue and this fatigue can become overwhelming. People with chronic pain can report being drained of energy and motivation to engage with others or the world around them.
In fact, a study from the United Kingdom on people with long-term health conditions found pain and fatigue are the two biggest barriers to an active and meaningful life.
But why is long-term pain so exhausting? One clue is the nature of pain and its powerful effect on our thoughts and behaviours.
simona pilolla 2/Shutterstock Short-term pain can protect you
Modern ways of thinking about pain emphasise its protective effect – the way it grabs your attention and compels you to change your behaviour to keep a body part safe.
Try this. Slowly pinch your skin. As you increase the pressure, you’ll notice the feeling changes until, at some point, it becomes painful. It is the pain that stops you squeezing harder, right? In this way, pain protects us.
When we are injured, tissue damage or inflammation makes our pain system become more sensitive. This pain stops us from mechanically loading the damaged tissue while it heals. For instance, the pain of a broken leg or a cut under our foot means we avoid walking on it.
The concept that “pain protects us and promotes healing” is one of the most important things people who were in chronic pain tell us they learned that helped them recover.
But long-term pain can overprotect you
In the short term, pain does a terrific job of protecting us and the longer our pain system is active, the more protective it becomes.
But persistent pain can overprotect us and prevent recovery. People in pain have called this “pain system hypersensitivity”. Think of this as your pain system being on red alert. And this is where exhaustion comes in.
When pain becomes a daily experience, triggered or amplified by a widening range of activities, contexts and cues, it becomes a constant drain on one’s resources. Going about life with pain requires substantial and constant effort, and this makes us fatigued.
About 80% of us are lucky enough to not know what it is like to have pain, day in day out, for months or years. But take a moment to imagine what it would be like.
Imagine having to concentrate hard, to muster energy and use distraction techniques, just to go about your everyday tasks, let alone to complete work, caring or other duties.
Whenever you are in pain, you are faced with a choice of whether, and how, to act on it. Constantly making this choice requires thought, effort and strategy.
Mentioning your pain, or explaining its impact on each moment, task or activity, is also tiring and difficult to get across when no-one else can see or feel your pain. For those who do listen, it can become tedious, draining or worrying.
Concentrating hard, mustering energy and using distraction techniques can make everyday life exhausting. PRPicturesProduction/Shutterstock No wonder pain is exhausting
In chronic pain, it’s not just the pain system on red alert. Increased inflammation throughout the body (the immune system on red alert), disrupted output of the hormone cortisol (the endocrine system on red alert), and stiff and guarded movements (the motor system on red alert) also go hand in hand with chronic pain.
Each of these adds to fatigue and exhaustion. So learning how to manage and resolve chronic pain often includes learning how to best manage the over-activation of these systems.
Loss of sleep is also a factor in both fatigue and pain. Pain causes disruptions to sleep, and loss of sleep contributes to pain.
In other words, chronic pain is seldom “just” pain. No wonder being in long-term pain can become all-consuming and exhausting.
What actually works?
People with chronic pain are stigmatised, dismissed and misunderstood, which can lead to them not getting the care they need. Ongoing pain may prevent people working, limit their socialising and impact their relationships. This can lead to a descending spiral of social, personal and economic disadvantage.
So we need better access to evidence-based care, with high-quality education for people with chronic pain.
There is good news here though. Modern care for chronic pain, which is grounded in first gaining a modern understanding of the underlying biology of chronic pain, helps.
The key seems to be recognising, and accepting, that a hypersensitive pain system is a key player in chronic pain. This makes a quick fix highly unlikely but a program of gradual change – perhaps over months or even years – promising.
Understanding how pain works, how persisting pain becomes overprotective, how our brains and bodies adapt to training, and then learning new skills and strategies to gradually retrain both brain and body, offers scientifically based hope; there’s strong supportive evidence from clinical trials.
Every bit of support helps
The best treatments we have for chronic pain take effort, patience, persistence, courage and often a good coach. All that is a pretty overwhelming proposition for someone already exhausted.
So, if you are in the 80% of the population without chronic pain, spare a thought for what’s required and support your colleague, friend, partner, child or parent as they take on the journey.
More information about chronic pain is available from Pain Revolution.
Michael Henry, Physiotherapist and PhD candidate, Body in Mind Research Group, University of South Australia and Lorimer Moseley, Professor of Clinical Neurosciences and Foundation Chair in Physiotherapy, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-

Codependent No More – by Melody Beattie
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a book review, not a book summary, but first let’s quickly cover a common misconception, because the word “codependent” gets misused a lot in popular parlance:
- What codependence isn’t: “we depend on each other and must do everything together”
- What codependence is:“person 1 has a dependency on a substance (or perhaps a behavior, such as gambling); person 2 is trying to look after person 1, and so has developed a secondary relationship with the substance/behavior. Person 2 is now said to be codependent, because it becomes all-consuming for them too, even if they’re not using the substance/behavior directly”
Funny how often it happens that the reality is more complex than the perception, isn’t it?
Melody Beattie unravels all this for us. We get a compassionate and insightful look at how we can look after ourselves, while looking after another. Perhaps most importantly: how and where to draw a line of what we can and cannot do/change for them.
Because when we love someone, of course we want to fight their battles with them, if not for them. But if we want to be their rock of strength, we can’t get lost in it too, and of course that hurts.
Beatty takes us through these ideas and more, for example:
- How to examine our own feelings even when it’s scary
- How to practice self-love and regain self-worth, while still caring for them
- How to stop being reactionary, step back, and act with purpose
If the book has any weak point, it’s that it repeatedly recommends 12-step programs, when in reality that’s just one option. But for those who wish to take another approach, this book does not require involvement in a 12-step program, so it’s not a barrier to usefulness.
Click here to check out Codependent No More and take care of yourself, too
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Habits of a Happy Brain – by Dr. Loretta Graziano Breuning
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are lots of books on “happy chemicals” and “how to retrain your brain”, so what makes this one different?
Firstly, it focuses on four “happy chemicals”, not just one:
- Serotonin
- Dopamine
- Oxytocin
- Endorphins
It also looks at the role of cortisol, and how it caps off each of those just a little bit, to keep us just a little malcontent.
Behavioral psychology tends to focus most on dopamine, while prescription pharmaceuticals for happiness (i.e., most antidepressants) tend to focus on serotonin. Here, Dr. Breuning helps us understand the complex interplay of all of the aforementioned chemicals.
She also clears up many misconceptions, since a lot of people misattribute the functions of each of these.
Common examples include “I’m doing this for the serotonin!” when the activity is dopaminergic not serotoninergic, or considering dopamine “the love molecule” when oxytocin, or even something else like phenylethylamine would be more appropriate.
The above may seem like academic quibbles and not something of practical use, but if we want to biohack our brains, we need to do better than the equivalent of a chef who doesn’t know the difference between salt and sugar.
Where things are of less practical use, she tends to skip over or at least streamline them. For example, she doesn’t really discuss the role of post-dopamine prolactin in men—but the discussion of post-happiness cortisol covers the same ground anyway, for practical purposes.
Dr. Breuning also looks at where our evolved neurochemical responses go wrong, and lays out guidelines for such challenges as overcoming addiction, or embracing delayed gratification.
Bottom line: this book is a great user-manual for the brain. If you’d like to be happier and more effective with fewer bad habits, this is the book for you.
Click here to check out Habits of a Happy Brain, and get biohacking yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Turns out the viral ‘Sleepy Girl Mocktail’ is backed by science. Should you try it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many of us wish we could get a better night’s sleep. Wouldn’t it be great if it was as easy as a mocktail before bed?
That’s what the latest viral trend might have us believe. The “Sleepy Girl Mocktail” is a mix of tart cherry juice, powdered magnesium supplement and soda water. TikTok videos featuring the concoction have garnered hundreds of thousands of views. But, what does the science say? Do these ingredients actually help us sleep?
Tart cherry juice
There is research to show including tart cherry juice in your diet improves overall sleep. Clinical trials show tart cherry juice increases sleep quality and quantity, as well as a lessening insomnia symptoms (compared to a placebo). This could be due to the presence of melatonin, a sleep-promoting hormone, in cherries.
Tart cherry varieties such as Jerte Valley or Montmorency have the highest concentration of melatonin (approximately 0.135 micrograms of melatonin per 100g of cherry juice). Over the counter melatonin supplements can range from 0.5 milligram to over 100 milligrams, with research suggesting those beginning to take melatonin start with a dose of 0.5–2 milligrams to see an improvement in sleep.
Melatonin naturally occurs in our bodies. Our body clock promotes the release of melatonin in the evening to help us sleep, specifically in the two hours before our natural bedtime.
If we want to increase our melatonin intake with external sources, such as cherries, then we should be timing our intake with our natural increase in melatonin. Supplementing melatonin too close to bed will mean we may not get the sleep-promoting benefits in time to get off to sleep easily. Taking melatonin too late may even harm our long-term sleep health by sending the message to our body clock to delay the release of melatonin until later in the evening.
Magnesium – but how much?
Magnesium also works to promote melatonin, and magnesium supplements have been shown to improve sleep outcomes.
However, results vary depending on the amount of magnesium people take. And we don’t yet have the answers on the best dose of magnesium for sleep benefits.
We do know magnesium plays a vital role in energy production and bone development, making it an important daily nutrient for our diets. Foods rich in magnesium include wheat cereal or bread, almonds, cashews, pumpkin seeds, spinach, artichokes, green beans, soy milk and dark chocolate.
Bubbly water
Soda water serves as the base of the drink, rather than a pathway to better sleep. And bubbly water may make the mix more palatable. It is important to keep in mind that drinking fluids close to bedtime can be disruptive to our sleep as it might lead to waking during the night to urinate.
Healthy sleep recommendations include avoiding water intake in the two hours before bed. Having carbonated beverages too close to bed can also trigger digestive symptoms such as bloating, gassiness and reflux during the night.
Bottoms up?
Overall, there is evidence to support trying out the Sleepy Girl Mocktail to see if it improves sleep, however there are some key things to remember:
timing: to get the benefits of this drink, avoid having it too close to bed. Aim to have it two hours before your usual bedtime and avoid fluids after this time
consistency: no drink is going to be an immediate cure for poor sleep. However, this recipe could help promote sleep if used strategically (at the right time) and consistently as part of a balanced diet. It may also introduce a calming evening routine that helps your brain relax and signals it’s time for bed
- maximum magnesium: be mindful of the amount of magnesium you are consuming. While there are many health benefits to magnesium, the recommended daily maximum amounts are 420mg for adult males and 320mg for adult females. Exceeding the maximum can lead to low blood pressure, respiratory distress, stomach problems, muscle weakness and mood problems
sugar: in some of the TikTok recipes sugar (as flavoured sodas, syrups or lollies) is added to the drink. While this may help hide the taste of the tart cherry juice, the consumption of sugar too close to bed may make it more difficult to get to sleep. And sugar in the evening raises blood sugar levels at a time when our body is not primed to be processing sugar. Long term, this can increase our risk of diabetes
sleep environment: follow good sleep hygiene practices including keeping a consistent bedtime and wake time, a wind-down routine before bed, avoiding electronic device use like phones or laptops in bed, and avoiding bright light in the evening. Bright light works to suppress our melatonin levels in the evening and make us more alert.
What about other drinks?
Other common evening beverages include herbal tisanes or teas, hot chocolate, or warm milk.
Milk can be especially beneficial for sleep, as it contains the amino acid tryptophan, which can promote melatonin production. Again, it is important to also consider the timing of these drinks and to avoid any caffeine in tea and too much chocolate too close to bedtime, as this can make us more alert rather than sleepy.
Getting enough sleep is crucial to our health and wellbeing. If you have tried multiple strategies to improve your sleep and things are not getting better, it may be time to seek professional advice, such as from a GP.
Charlotte Gupta, Postdoctoral research fellow, CQUniversity Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: