Magic mushrooms may one day treat anorexia, but not just yet
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anorexia nervosa is a severe mental health disorder where people fear weight gain. Those with the disorder have distorted body image and hold rigid beliefs their body is too big. They typically manage this through restricted eating, leading to the serious medical consequences of malnutrition.
Anorexia has one of the highest death rates of any mental illness. Yet there are currently no effective drug treatments and the outcomes of psychotherapy (talk therapy) are poor. So we’re desperately in need of new and improved treatments.
Psilocybin, commonly known as magic mushrooms, is one such novel treatment. But while it shows early promise, you won’t see it used in clinical practice just yet – more research is needed to test if it’s safe and effective.

What does treatment involve?
The treatment involves the patient taking a dose of psilocybin in a safe environment, which is usually a specifically set up clinic. The patient undergoes preparation therapy before the dosing session and integration therapy after.
Psilocybin, extracted from mushrooms, is a psychedelic, which means it can produce altered thinking, sense of time and emotions, and can often result in hallucinations. It also has the potential to shift patients out of their rigid thinking patterns.
Psilocybin is not administered alone but instead with combined structured psychotherapy sessions to help the patient make sense of their experiences and the changes to their thinking. This is an important part of the treatment.
What does the research show?
Research has shown improved effects of psilocybin-assisted psychotherapy after one or two dosing sessions, a couple of weeks apart. Most research to date has targeted depression.
Psilocybin has been found to increase cognitive flexibility – our ability to adjust our thinking patterns according to changing environments or demands. This is one of the ways researchers believe psilocybin might improve symptoms for conditions such as depression and alcohol use disorder, which are marked by rigid thinking styles.
People with anorexia similarly struggle with rigid thinking patterns. So researchers and clinicians have recently turned their attention to anorexia.
In 2023, a small pilot study of ten women with anorexia was published in the journal Nature Medicine. It showed psilocybin-assisted psychotherapy (with 25mg of psilocybin) was safe and acceptable. There were no significant side effects and participants reported having valuable experiences.
Although the trial was not a formal efficacy trial, 40% of the patients did have significant drops in their eating disorder behaviour.
However, the trial only had one dosing session and no long-term follow up, so further research is needed.

A recent animal study using rats examined whether rigid thinking could be improved in rats when given psilocybin. After the psilocybin, rats gained weight and had more flexible thinking (using a reversal learning task).
These positive changes were related to the serotonin neurotransmitter system, which regulates mood, behaviour and satiety (feeling full).
Brain imaging studies in humans show serotonin disturbances in people with anorexia. Psilocybin-assisted psychotherapy is showing promise at modifying the serotonin disturbances and cognitive inflexibility that have been shown to be problematic in anorexia.
Research with animals can provide unique insights into the brain which can sometimes not be investigated in living humans. But animal models can never truly mimic human behaviour and the complex nature of chronic mental health conditions.
What’s next for research?
Further clinical trials in humans are very much needed – and are underway from a research team at the University of Sydney and ours at Swinburne.
Our trial will involve an initial 5mg dose followed by two subsequent doses of 25mg, several weeks apart. An initial low dose aims to help participants prepare for what is likely to be a new and somewhat unpredictable experience.
Our trial will examine the usefulness of providing psychotherapy that directly addresses body image disturbance. We are also investigating if including a family member or close friend in the treatment increases support for their loved one.

Data from other mental health conditions has suggested that not everyone sees benefits, with some people having bad trips and a deterioration in their mental health. So this treatment won’t be for everyone. It’s important to work out who is most likely to respond and under what conditions.
New trials and those underway will be critical in understanding whether psilocybin-assisted psychotherapy is a safe and effective treatment for anorexia, and the optimal conditions to improve the patient’s response. But we are some way off from seeing this treatment in the clinic. One of the big issues being the cost of this intervention and how this will be funded.
Susan Rossell, Director Clinical Trials and Professor Cognitive Neuropsychiatry Centre for Mental Health and Brain Sciences, Swinburne University of Technology and Claire Finkelstein, Clinical Psychologist and PhD candidate, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Stay off My Operating Table – by Dr. Philip Ovadia

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
With heart disease as the #1 killer worldwide, and 88% of adults being metabolically unhealthy (leading cause of heart disease), this is serious!
Rather than taking a “quick fix” advise-and-go approach, Dr. Ovadia puts the knowledge and tools in our hands to do better in the long term.
As a heart surgeon himself, his motto here is:
❝What foods to put on your table so you don’t end up on mine❞
There’s a lot more to this book than the simple “eat the Mediterranean diet”:
- While the Mediterranean diet is generally considered the top choice for heart health, he also advises on how to eat healthily on all manner of diets… Carnivore, Keto, Paleo, Atkins, Gluten-Free, Vegan, you-name-it.
- A lot of the book is given to clearing up common misconceptions, things that sounded plausible but are just plain dangerous. This information alone is worth the price of the book, we think.
- There’s also a section given over to explaining the markers of metabolic health, so you can monitor yourself effectively
- Rather than one-size-fits-all, he also talks about common health conditions and medications that may change what you need to be doing
- He also offers advice about navigating the health system to get what you need—including dealing with unhelpful doctors!
Bottom line: A very comprehensive (yet readable!) manual of heart health.
Get your copy of Stay Off My Operating Table from Amazon today!
Share This Post
-

The Power Foods Diet – by Dr. Neal Barnard
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this is not: it’s not a cookbook. There are recipes, more than a hundred if we consider such things as “barbecue sauce” as a standalone recipe, and if we overlook such things as how “perfect hot oatmeal” is followed on the next page by a recipe for “perfect hot oatmeal with berries”.
However, as we say, it’s not a cookbook; it’s first and foremost an educational text on the topic of nutrition.
Here we will learn about good eating for general health, which foods are natural appetite-suppressants, which foods reduce our body’s absorption of sugars from foods (not merely slowing, but flushing them away so they cannot be absorbed at all), and which foods actually boost metabolism for a few hours after the meal.
Dr. Barnard also talks about some foods that are more healthy, or less healthy, than popularly believed, and how to use all this information to craft a good, optimized, dietary plan for you.
Bottom line: there’s a lot of good information here, and the recipes are simply a bonus.
Click here to check out The Power Foods Diet, and optimize yours!
Share This Post
-

Brown Rice vs Rye – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing brown rice to rye, we picked the rye.
Why?
It’s a simple one today, and it wasn’t close:
In terms of macros, rye has nearly 4x the fiber for the same carbs and slightly more protein, winning easily in this category.
In the category of vitamins, brown rice has more of vitamins B1, B3, and B6, while rye has more of vitamins A, B2, B5, B7, B9, E, and K, winning another round easily.
Looking at minerals next, brown rice has more selenium, while rye has more calcium, copper, iron, potassium, and zinc, winning its third round in a row.
Adding up the sections makes for a clear overall win for rye, but by all means do still enjoy either or both, as diversity is best!
Want to learn more?
You might like:
- Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
- What Do The Different Kinds Of Fiber Do? 30 Foods That Rank Highest
- What Matters Most For Your Heart? Eat More (Of This) For Lower Blood Pressure ← Spoiler: it’s fiber
Enjoy!
Share This Post

-

Scheduling Tips for Overrunning Tasks
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Your Questions, Our Answers!
Q: Often I schedule time for things, but the task takes longer than I think, or multiplies while I’m doing it, and then my schedule gets thrown out. Any ideas?
A: A relatable struggle! Happily, there are remedies:
- Does the task really absolutely need to be finished today? If not, just continue it in scheduled timeslots until it’s completed.
- Some tasks do indeed need to be finished today (hi, writer of a daily newsletter here!), so it can be useful to have an idea of how long things really take, in advance. While new tasks can catch us unawares, recurring or similar-to-previous tasks can be estimated based on how long they took previously. For this reason, we recommend doing a time audit every now and again, to see how you really use your time.
- A great resource that you should include in your schedule is a “spare” timeslot, ideally at least one per day. Call it a “buffer” or a “backup” or whatever (in my schedule it’s labelled “discretionary”), but the basic idea is that it’s a scheduled timeslot with nothing scheduled in it, and it works as an “overflow” catch-all.
Additionally:
- You can usually cut down the time it takes you to do tasks by setting “Deep Work” rules for yourself. For example: cut out distractions, single-task, work in for example 25-minute bursts with 5-minute breaks, etc
- You can also usually cut down the time it takes you to do tasks by making sure you’re prepared for them. Not just task-specific preparation, either! A clear head on, plenty of energy, the resources you’ll need (including refreshments!) to hand, etc can make a huge difference to efficiency.
See Also: Time Optimism and the Planning Fallacy
Do you have a question you’d like to see answered here? Hit reply or use the feedback widget at the bottom; we’d love to hear from you!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Grapefruit vs Lime – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing grapefruit to lime, we picked the lime.
Why?
Both have their merits, but…
In terms of macros, limes have 2x the fiber, for comparable protein and carbs. Thus, the winner in the macros category.
In the category of vitamins, grapefruit has more of vitamins A, B1, and B9, while limes have more of vitamins E and K. They’re approximately equal on other vitamins they both contain (including, notably, vitamin C, of which they are both good sources, and one cup of chopped fruit will provide the RDA of vitamin C), so this is a marginal 3:2 win for grapefruit in this round.
Looking at minerals, grapefruit has more magnesium, manganese, and and potassium, while limes have more calcium, copper, iron, selenium, and zinc. So, a win for limes here.
One final consideration that’s not shown in the nutritional values, is that grapefruit contains high levels of furanocoumarin, which can inhibit cytochrome P-450 3A4 isoenzyme and P-glycoptrotein transporters in the intestine and liver—slowing down their drug metabolism capabilities, thus effectively increasing the bioavailability of many drugs manifold.
This may sound superficially like a good thing (improving bioavailability of things we want), but in practice it means that in the case of many drugs, if you take them with (or near in time to) grapefruit or grapefruit juice, then congratulations, you just took an overdose. This happens with a lot of meds for blood pressure, cholesterol (including statins), calcium channel-blockers, anti-depressants, benzo-family drugs, beta-blockers, and more. Oh, and Viagra, too. Which latter might sound funny, but remember, Viagra’s mechanism of action is blood pressure modulation, and that is not something you want to mess around with unduly. So, do check with your pharmacist to know if you’re on any meds that would be affected by grapefruit or grapefruit juice!
PS: the same substance is quite available in pummelos and sour oranges (but not meaningfully in sweet oranges); you can see a chart here showing the relative furanocoumarin contents of many citrus fruits, or lack thereof as the case may be, as it isn’t very present in lemons and most limes).
Adding up the sections gives us an overall win for limes, but by all means enjoy either or both; just watch out for that furanocoumarin content of grapefruit if you’re on any meds affected by such (again, do check with your pharmacist, as our list was far from exhaustive—and yes, this question is one that a pharmacist will answer more easily and accurately than a doctor will).
Want to learn more?
You might like:
Top 8 Fruits That Prevent & Kill Cancer ← citrus fruits in general make the list; they inhibit tumor growth and kill cancer cells; regular consumption is also associated with a lower cancer risk 🙂
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What Most People Don’t Know About HIV
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What To Know About HIV This World AIDS Day

Yesterday, we asked 10almonds readers to engage in a hypothetical thought experiment with us, and putting aside for a moment any reason you might feel the scenario wouldn’t apply for you, asked:
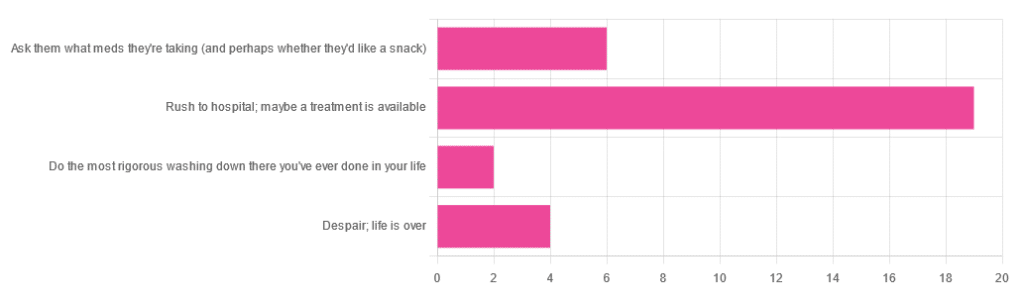
❝You have unprotected sex with someone who, afterwards, conversationally mentions their HIV+ status. Do you…❞
…and got the above-depicted, below-described, set of responses. Of those who responded…
- Just over 60% said “rush to hospital; maybe a treatment is available”
- Just under 20% said “ask them what meds they’re taking (and perhaps whether they’d like a snack)”
- Just over 10% said “despair; life is over”
- Two people said “do the most rigorous washing down there you’ve ever done in your life”
So, what does science say about it?
First, a quick note on terms
- HIV is the Human Immunodeficiency Virus. It does what it says on the tin; it gives humans immunodeficiency. Like many viruses that have become epidemic in humans, it started off in animals (called SIV, because there was no “H” involved yet), which were then eaten by humans, passing the virus to us when it one day mutated to allow that.
- It’s technically two viruses, but that’s beyond the scope of today’s article; for our purposes they are the same. HIV-1 is more virulent and infectious than HIV-2, and is the kind more commonly found in most of the world.
- AIDS is Acquired Immunodeficiency Syndrome, and again, is what it sounds like. When a person is infected with HIV, then without treatment, they will often develop AIDS.
- Technically AIDS itself doesn’t kill people; it just renders people near-defenseless to opportunistic infections (and immune-related diseases such as cancer), since one no longer has a properly working immune system. Common causes of death in AIDS patients include cancer, influenza, pneumonia, and tuberculosis.
People who contract HIV will usually develop AIDS if untreated. Untreated life expectancy is about 11 years.
HIV/AIDS are only a problem for gay people: True or False?
False, unequivocally. Anyone can get HIV and develop AIDS.
The reason it’s more associated with gay men, aside from homophobia, is that since penetrative sex is more likely to pass it on, then if we go with the statistically most likely arrangements here:
- If a man penetrates a woman and passes on HIV, that woman will probably not go on to penetrate someone else
- If a man penetrates a man and passes on HIV, that man could go on to penetrate someone else—and so on
- This means that without any difference in safety practices or promiscuity, it’s going to spread more between men on average, by simple mathematics.
- This is why “men who have sex with men” is the generally-designated higher-risk category.
There is medication to cure HIV/AIDS: True or False?
False so far (though there have been individual case studies of gene treatments that may have cured people—time will tell).
But! There are medications that can prevent HIV from being a life-threatening problem:
- PrEP (Pre-Exposure Prophylaxis) is a medication that one can take in advance of potential exposure to HIV, to guard against it.
- This is a common choice for people aren’t sure about their partners’ statuses, or people working in risky environments.
- PEP (Post-Exposure Prophylaxis) is a medication that one can take after potential exposure to HIV, to “nip it in the bud”.
- Those of you who were rushing to hospital in our poll, this is what you’re rushing there for.
- ARVs (Anti-RetroVirals) are a class of medications (there are different options; we don’t have room to distinguish them) that reduce an HIV+ person’s viral load to undetectable levels.
- Those of you who were asking what meds your partner was taking, these will be those meds. Also, most of them are to be taken in the morning with food, so that’s what the snack was for.
If someone is HIV+, the risk of transmission in unprotected sex is high: True or False?
True or False, with false being the far more likely. It depends on their medications, and this is why you were asking. If someone is on ARVs and their viral load is undetectable (as is usual once someone has been on ARVs for 6 months), they cannot transmit HIV to you.
U=U is not a fancy new emoticon, it means “undetectable = untransmittable”, which is a mathematically true statement in the case of HIV viral loads.
See: NIH | HIV Undetectable=Untransmittable (U=U)
If you’re thinking “still sounds risky to me”, then consider this:
You are safer having unprotected sex with someone who is HIV+ and on ARVs with an undetectable viral load, than you are with someone you are merely assuming is HIV- (perhaps you assume it because “surely this polite blushing young virgin of a straight man won’t give me cooties” etc)
Note that even your monogamous partner of many decades could accidentally contract HIV due to blood contamination in a hospital or an accident at work etc, so it’s good practice to also get tested after things that involve getting stabbed with needles, cut in a risky environment, etc.
If you’re concerned about potential stigma associated with HIV testing, you can get kits online:
CDC | How do I find an HIV self-test?
(these are usually fingerprick blood tests, and you can either see the results yourself at home immediately, or send it in for analysis, depending on the kit)
If I get HIV, I will get AIDS and die: True or False?
False, assuming you get treatment promptly and keep taking it. So those of you who were at “despair; life is over” can breathe a sigh of relief now.
However, if you get HIV, it does currently mean you will have to take those meds every day for the rest of your (no reason it shouldn’t be long and happy) life.
So, HIV is definitely still something to avoid, because it’s not great to have to take a life-saving medication every day. For a little insight as to what that might be like:
HIV.gov | Taking HIV Medication Every Day: Tips & Challenges
(as you’ll see there, there are also longer-lasting injections available instead of daily pulls, but those are much less widely available)
Summary
Some quick take-away notes-in-a-nutshell:
- Getting HIV may have been a death sentence in the 1980s, but nowadays it’s been relegated to the level of “serious inconvenience”.
- Happily, it is very preventable, with PrEP, PEP, and viral loads so low that they can’t transmit HIV, thanks to ARVs.
- Washing will not help, by the way. Safe sex will, though!
- As will celibacy and/or sexual exclusivity in seroconcordant relationships, e.g. you have the same (known! That means actually tested recently! Not just assumed!) HIV status as each other.
- If you do get it, it is very manageable with ARVs, but prevention is better than treatment
- There is no certain cure—yet. Some people (small number of case studies) may have been cured already with gene therapy, but we can’t know for sure yet.
Want to know more? Check out:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: