New News From The Centenarian Blue Zones
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From Blue To Green…
We sometimes write about supercentenarians, which word is usually used in academia to refer to people who are not merely over 100 years of age, but over 110 years. These people can be found in many countries, but places where they have been found to be most populous (as a percentage of the local population) have earned the moniker “Blue Zones”—of which Okinawa and Sardinia are probably the most famous, but there are others too.
This is in contrast to, for example “Red Zones”, a term often used for areas where a particular disease is endemic, or areas where a disease is “merely” epidemic, but particularly rife at present.
In any case, back to the Blue Zones, where people live the longest and healthiest—because the latter part is important too! See also:
- Lifespan: how long we live
- Healthspan: how long we stay healthy (portmanteau of “healthy lifespan”)
Most of our readers don’t live in a Blue Zone (in fact, many live in the US, which is a COVID Red Zone, a diabetes Red Zone, and a heart disease Red Zone), but that doesn’t mean we can’t all take tips from the Blue Zones and apply them, for example:
- The basics: The Blue Zones’ Five Pillars Of Longevity
- Going beyond: The Five Key Traits Of Healthy Aging
You may be wondering… How much good will this do me? And, we do have an answer for that:
When All’s Said And Done, How Likely Are You To Live To 100?
Now that we’re all caught-up…
The news from the Blues
A team of researchers did a big review of observational studies of centenarians and near-centenarians (aged 95+). Why include the near-centenarians, you ask? Well, most of the studies are also longitudinal, and if we’re doing an observational study of the impact of lifestyle factors on a 100-year-old, it’s helpful to know what they’ve been doing recently. Hence nudging the younger-end cutoff a little lower, so as to not begin each study with fresh-faced 100-year-olds whom we know nothing about.
Looking at thousands of centenarians (and near-centenarians, but also including some supercentenarians, up the age of 118), the researchers got a lot of very valuable data, far more than we have room to go into here (do check out the paper at the bottom of this article, if you have time; it’s a treasure trove of data), but one of the key summary findings was a short list of four factors they found contributed the most to extreme longevity:
- A diverse diet with low salt intake: in particular, a wide variety of plant diversity, including protein-rich legumes, though fish featured prominently also. On average they got 57% and 65% of their energy intake from carbohydrates, 12% to 32% from protein, and 27% to 31% from fat. As for salt, they averaged 1.6g of sodium per day, which is well within the WHO’s recommendation of averaging under 2g of sodium per day. As a matter of interest, centenarians in Okinawa itself averaged 1.1g of sodium per day.
- Low medication use: obviously there may be a degree of non-causal association here, i.e. the same people who just happened to be healthier and therefore lived longer, correspondingly took fewer medications—they took fewer medications because they were healthier; they weren’t necessarily healthier because they took fewer medications. That said, overmedication can be a big problem, especially in places with a profit motive like the US, and can increase the risk of harmful drug interactions, and side effects that then need more medications to treat the side effects, as well as direct iatrogenic damage (i.e. this drug treats your condition, but as the cost of harming you in some other way). Naturally, sometimes we really do need meds, but it’s a good reminder to do a meds review with one’s doctor once in a while, and see if everything’s still of benefit.
- Getting good sleep: not shocking, and this one’s not exactly news. But what may be shocking is that 68% of centenarians reported consistently getting enough good-quality sleep. To put that into perspective, only 35% of 10almonds readers reported regularly getting sleep in the 7–9 hours range.
- Rural living environment: more than 75% of the centenarians and near-centenarians lived in rural areas. This is not usually something touted as a Blue Zones thing on lists of Blue zones things, but this review strongly highlighted it as very relevant. In the category of things that are more obvious once it’s pointed out, though, this isn’t necessarily such a difference between “country folk” and “city folk”, so much as the ability to regularly be in green spaces has well-established health benefits physically, mentally, and both combined (such as: neurologically).
And showing that yes, even parks in cities make a significant difference:
Want to know more?
You can read the study in full here:
A systematic review of diet and medication use among centenarians and near-centenarians worldwide
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Can you get sunburnt or UV skin damage through car or home windows?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When you’re in a car, train or bus, do you choose a seat to avoid being in the sun or do you like the sunny side?
You can definitely feel the sun’s heat through a window. But can you get sunburn or skin damage when in your car or inside with the windows closed?
Let’s look at how much UV (ultraviolet) radiation passes through different types of glass, how tinting can help block UV, and whether we need sunscreen when driving or indoors.

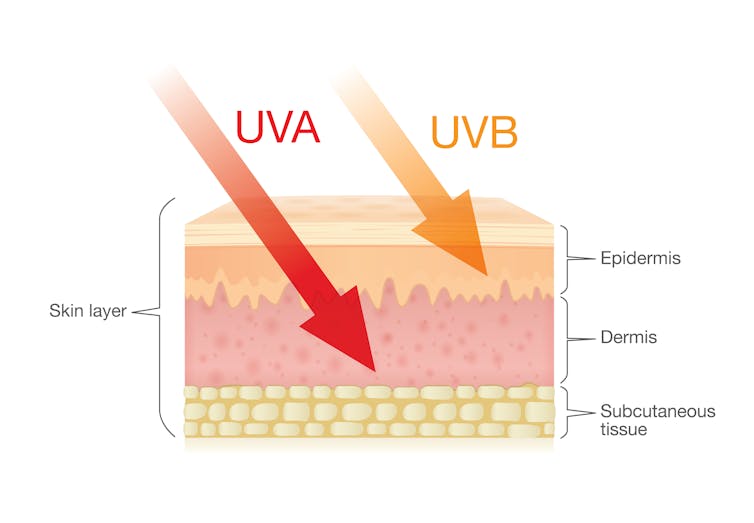
Zac Harris/Unsplash What’s the difference between UVA and UVB?
Of the total UV radiation that reaches Earth, about 95% is UVA and 5% is UVB.
UVB only reaches the upper layers of our skin but is the major cause of sunburn, cataracts and skin cancer.
UVA penetrates deeper into our skin and causes cell damage that leads to skin cancer.
UVA penetrates deeper than UVB. Shutterstock/solar22 Glass blocks UVA and UVB radiation differently
All glass used in house, office and car windows completely blocks UVB from passing through.
But only laminated glass can completely block UVA. UVA can pass through other glass used in car, house and office windows and cause skin damage, increasing the risk of cancer.
Car windscreens block UVA, but the side and rear windows don’t
A car’s front windscreen lets in lots of sunshine and light. Luckily it blocks 98% of UVA radiation because it is made of two layers of laminated glass.
But the side and rear car windows are made of tempered glass, which doesn’t completely block UVA. A study of 29 cars found a range from 4% to almost 56% of UVA passed through the side and rear windows.
The UVA protection was not related to the car’s age or cost, but to the type of glass, its colour and whether it has been tinted or coated in a protective film. Grey or bronze coloured glass, and window tinting, all increase UVA protection. Window tinting blocks around 95% of UVA radiation.
In a separate study from Saudi Arabia, researchers fitted drivers with a wearable radiation monitor. They found drivers were exposed to UV index ratings up to 3.5. (In Australia, sun protection is generally recommended when the UV index is 3 or above – at this level it takes pale skin about 20 minutes to burn.)
So if you have your windows tinted, you should not have to wear sunscreen in the car. But without tinted windows, you can accumulate skin damage.
UV exposure while driving increases skin cancer risk
Many people spend a lot of time in the car – for work, commuting, holiday travel and general transport. Repeated UVA radiation exposure through car side windows might go unnoticed, but it can affect our skin.
Indeed, skin cancer is more common on the driver’s side of the body. A study in the United States (where drivers sit on the left side) found more skin cancers on the left than the right side for the face, scalp, arm and leg, including 20 times more for the arm.
Another US study found this effect was higher in men. For melanoma in situ, an early form of melanoma, 74% of these cancers were on the on the left versus 26% on the right.
Earlier Australian studies reported more skin damage and more skin cancer on the right side.
Cataracts and other eye damage are also more common on the driver’s side of the body.
What about UV exposure through home or office windows?
We see UV damage from sunlight through our home windows in faded materials, furniture or plastics.
Most glass used in residential windows lets a lot of UVA pass through, between 45 and 75%.
Residential windows can let varied amounts of UVA through. Sherman Trotz/Pexels Single-pane glass lets through the most UVA, while thicker, tinted or coated glass blocks more UVA.
The best options are laminated glass, or double-glazed, tinted windows that allow less than 1% of UVA through.
Skylights are made from laminated glass, which completely stops UVA from passing through.
Most office and commercial window glass has better UVA protection than residential windows, allowing less than 25% of UVA transmission. These windows are usually double-glazed and tinted, with reflective properties or UV-absorbent chemicals.
Some smart windows that reduce heat using chemical treatments to darken the glass can also block UVA.
So when should you wear sunscreen and sunglasses?
The biggest risk with skin damage while driving is having the windows down or your arm out the window in direct sun. Even untinted windows will reduce UVA exposure to some extent, so it’s better to have the car window up.
For home windows, window films or tint can increase UVA protection of single pane glass. UVA blocking by glass is similar to protection by sunscreen.
When you need to use sunscreen depends on your skin type, latitude and time of the year. In a car without tinted windows, you could burn after one hour in the middle of the day in summer, and two hours in the middle of a winter’s day.
But in the middle of the day next to a home window that allows more UVA to pass through, it could take only 30 minutes to burn in summer and one hour in winter.
When the UV index is above three, it is recommended you wear protective sunglasses while driving or next to a sunny window to avoid eye damage.
Theresa Larkin, Associate Professor of Medical Sciences, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Why Zebras Don’t Get Ulcers – by Dr. Robert M. Sapolsky
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The book does kick off with a section that didn’t age well—he talks of the stress induced globally by the Spanish Flu pandemic of 1918, and how that kind of thing just doesn’t happen any more. Today, we have much less existentially dangerous stressors!
However, the fact we went and had another pandemic really only adds weight to the general arguments of the book, rather than detracting.
We are consistently beset by “the slings and arrows of outrageous fortune” as Shakespeare would put it, and there’s a reason (or twenty) why many people go grocery-shopping with the cortisol levels of someone being hunted for sport.
So, why don’t zebras get ulcers, as they actually are hunted for food?
They don’t have rent to pay or a mortgage, they don’t have taxes, or traffic, or a broken washing machine, or a project due in the morning. Their problems come one at a time. They have a useful stress response to a stressful situation (say, being chased by lions), and when the danger is over, they go back to grazing. They have time to recover.
For us, we are (usually) not being chased by lions. But we have everything else, constantly, around the clock. So, how to fix that?
Dr. Sapolsky comprehensively describes our physiological responses to stress in quite different terms than many. By reframing stress responses as part of the homeostatic system—trying to get the body back into balance—we find a solution, or rather: ways to help our bodies recover.
The style is “pop-science” and is very accessible for the lay reader while still clearly coming from a top-level academic who is neck-deep in neuroendocrinological research. Best of both worlds!
Bottom line: if you try to take very day at a time, but sometimes several days gang up on you at once, and you’d like to learn more about what happens inside you as a result and how to fix that, this book is for you!
Click here to check out “Why Zebras Don’t Get Ulcers” and give yourself a break!
Share This Post
-

The Cancer Code − by Dr. William Fung
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have previously reviewed, by the same author, “The Obesity Code” and “The Diabetes Code”, so, what does this one offer that’s new?
Mostly, it’s just a new focus, because the dietary approach is basically the same (because all three are fundamentally metabolism-related), with some small tweaks for cancer-specificity. If you’ve read one or more of the other books, you can probably comfortably get away with skipping this one, unless you or a loved one presently has cancer and you’re doing your best to squeeze out any extra 1% of anticancer potential.
Indeed, the former two books assumed that you are affected by obesity or diabetes, respectively, and this one assumes you are at least particularly concerned by cancer—he doesn’t assume you have it (although he does cover that too); he assumes however that you perhaps have a known risk factor or some other similar reason to be focusing on this.
To oversimplify a lot, the dietary approach recommended involves practising intermittent fasting, and also adjusting one’s diet to reduce fasting blood sugar levels and postprandial (after eating) blood sugar and insulin levels. Shocking nobody, he advocates for a lot of plants; he does however recommend a moderately low-carb diet (e.g. legumes are fine but maybe skip the fries).
The style is on the hard end of pop-science, while still quite readable provided one takes one’s time, and there are more than 30 pages of scientific references.
Bottom line: if you’d like to make your diet as anticancer as possible, this book will show you how.
Click there to check out The Cancer Code, and eat to beat cancer!
Share This Post


-

Heart Smarter for Women – by Dr. Jennifer Mieres
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Mieres takes us through understanding our own heart disease risks as individuals rather than as averages. As the title suggests, she does assume a female readership, so if you are a man and have no female loved ones, this might not be the book for you. But aside from that, she walks us through examining risk in the context of age, other health conditions, lifestyle factors, and so forth—including not turning a blind eye to factors that might intersect, such as for example if a physical condition reduces how much we can exercise, or if there’s some reason we can’t follow the usual gold standard of heart-healthy diet.
On which note, she does offer dietary advice, including information around recipes, meal-planning, and what things to always have in stock, as well as what things matter the most when it comes to what and how we eat.
It’s not all lifestyle medicine though; Dr. Mieres gives due attention to many of the medications available for heart health issues—and the pros and cons of these.
The style of the book is very simple and readable pop-science, without undue jargon, and with a generous glossary. As with many books of this genre, it does rely on (presumably apocryphal) anecdotes, though an interesting choice for this book is that it keeps a standing cast of four recurring characters, each to represent a set of circumstances and illustrate how certain things can go differently for different people, with different things then being needed and/or possible. Hopefully, any given reader will find themself represented at least moderately well somewhere in or between these four characters.
Bottom line: this is a very informative and accessible book, that demystifies a lot of common confusions around heart health.
Click here to check out Heart Smarter For Women, and take control of your health!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
First things first… How much fiber should we be eating?
- The World Health Organization recommends we each get at least 25g of fiber per day:
- A more recent meta-review of studies, involving thousands of people and decades of time, suggests 25–29g is ideal:
- The British Nutritional Foundation gives 30g as the figure:
- The US National Academy of Sciences’ Institute of Medicine recommends 21g–38g per day, depending on age and sex:
- A large study last year gave 30–40g as the figure:
*This one is also a great read to understand more about the “why” of fiber
Meanwhile, the average American gets 16g of fiber per day.
So, how to get more fiber, without piling on too many carbs?
Foods that contain fiber generally contain carbs (there’s a limit to how much celery most people want to eat), so there are two key ideas here:
- Getting a good carb:fiber ratio
- Making substitutions that boost fiber without overdoing (or in some case, even changing) carbs
Meat → Lentils
Well-seasoned lentils can be used to replaced ground beef or similar. A cup of boiled lentils contains 18g of fiber, so you’re already outdoing the average American’s daily total.
Meat → Beans
Black beans are a top-tier option here (15g per cup, cooked weight), but many kinds of beans are great.
Chicken/Fish → Chickpeas
Yes, chicken/fish is already meat, but we’re making a case for chickpeas here. Cooked and seasoned appropriately, they do the job, and pack in 12g of fiber per cup. Also… Hummus!
Bonus: Hummus, eaten with celery sticks.
White pasta/bread → Wholewheat pasta/bread
This is one where “moderation is key”, but if you’re going to eat pasta/bread, then wholewheat is the way to go. Fiber amounts vary, so read labels, but it will always have far more than white.
Processed salty snacks → Almonds and other nuts
Nuts in general are great, but almonds are top-tier for fiber, amongst other things. A 40g handful of almonds contains about 10g of fiber.
Starchy vegetables → Non-starchy vegetables
Potatoes, parsnips, and their friends have their place. But they cannot compete with broccoli, peas, cabbage, and other non-starchy vegetables for fiber content.
Bonus: if you’re going to have starchy vegetables though, leave the skins on!
Fruit juice → Fruit
Fruit juice has had most, if not all, of its fiber removed. Eat an actual juicy fruit, instead. Apples and bananas are great options; berries such as blackberries and raspberries are even better (at around 8g per cup, compared to the 5g or so depending on the size of an apple/banana)
Processed cereals → Oats
5g fiber per cup. Enough said.
Summary
Far from being a Herculean task, getting >30g of fiber per day can be easily accomplished by a lentil ragù with wholewheat pasta.
If your breakfast is overnight oats with fruit and some chopped almonds, you can make it to >20g already by the time you’ve finished your first meal of the day.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What’s the difference between a psychopath and a sociopath? Less than you might think
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Articles about badly behaved people and how to spot them are common. You don’t have to Google or scroll too much to find headlines such as 7 signs your boss is a psychopath or How to avoid the sociopath next door.
You’ll often see the terms psychopath and sociopath used somewhat interchangeably. That applies to perhaps the most famous badly behaved fictional character of all – Hannibal Lecter, the cannibal serial killer from The Silence of the Lambs.
In the book on which the movie is based, Lecter is described as a “pure sociopath”. But in the movie, he’s described as a “pure psychopath”. Psychiatrists have diagnosed him with something else entirely.
So what’s the difference between a psychopath and a sociopath? As we’ll see, these terms have been used at different times in history, and relate to some overlapping concepts.
Benoit Daoust/Shutterstock What’s a psychopath?
Psychopathy has been mentioned in the psychiatric literature since the 1800s. But the latest edition of the Diagnostic Statistical Manual of Mental Disorders (known colloquially as the DSM) doesn’t list it as a recognised clinical disorder.
Since the 1950s, labels have changed and terms such as “sociopathic personality disturbance” have been replaced with antisocial personality disorder, which is what we have today.
Was Hannibal Lecter from The Silence of the Lambs a psychopath, a sociopath or something else entirely? Ralf Liebhold/Shutterstock Someone with antisocial personality disorder has a persistent disregard for the rights of others. This includes breaking the law, repeated lying, impulsive behaviour, getting into fights, disregarding safety, irresponsible behaviours, and indifference to the consequences of their actions.
To add to the confusion, the section in the DSM on antisocial personality disorder mentions psychopathy (and sociopathy) traits. In other words, according to the DSM the traits are part of antisocial personality disorder but are not mental disorders themselves.
US psychiatrist Hervey Cleckley provided the first formal description of psychopathy traits in his 1941 book The Mask of Sanity. He based his description on his clinical observations of nine male patients in a psychiatric hospital. He identified several key characteristics, including superficial charm, unreliability and a lack of remorse or shame.
Canadian psychologist Professor Robert Hare refined these characteristics by emphasising interpersonal, emotional and lifestyle characteristics, in addition to the antisocial behaviours listed in the DSM.
When we draw together all these strands of evidence, we can say a psychopath manipulates others, shows superficial charm, is grandiose and is persistently deceptive. Emotional traits include a lack of emotion and empathy, indifference to the suffering of others, and not accepting responsibility for how their behaviour impacts others.
Finally, a psychopath is easily bored, sponges off others, lacks goals, and is persistently irresponsible in their actions.
So how about a sociopath?
The term sociopath first appeared in the 1930s, and was attributed to US psychologist George Partridge. He emphasised the societal consequences of behaviour that habitually violates the rights of others.
Academics and clinicians often used the terms sociopath and psychopath interchangeably. But some preferred the term sociopath because they said the public sometimes confused the word psychopath with psychosis.
“Sociopathic personality disturbance” was the term used in the first edition of the DSM in 1952. This aligned with the prevailing views at the time that antisocial behaviours were largely the product of the social environment, and that behaviours were only judged as deviant if they broke social, legal, and/or cultural rules.
Some of these early descriptions of sociopathy are more aligned with what we now call antisocial personality disorder. Others relate to emotional characteristics similar to Cleckley’s 1941 definition of a psychopath.
In short, different people had different ideas about sociopathy and, even today, sociopathy is less-well defined than psychopathy. So there is no single definition of sociopathy we can give you, even today. But in general, its antisocial behaviours can be similar to ones we see with psychopathy.
Over the decades, the term sociopathy fell out of favour. From the late 60s, psychiatrists used the term antisocial personality disorder instead.
Born or made?
Both “sociopathy” (what we now call antisocial personality disorder) and psychopathy have been associated with a wide range of developmental, biological and psychological causes.
For example, people with psychopathic traits have certain brain differences especially in regions associated with emotions, inhibition of behaviour and problem solving. They also appear to have differences associated with their nervous system, including a reduced heart rate.
However, sociopathy and its antisocial behaviours are a product of someone’s social environment, and tends to run in families. These behaviours has been associated with physical abuse and parental conflict.
What are the consequences?
Despite their fictional portrayals – such as Hannibal Lecter in Silence of the Lambs or Villanelle in the TV series Killing Eve – not all people with psychopathy or sociopathy traits are serial killers or are physically violent.
But psychopathy predicts a wide range of harmful behaviours. In the criminal justice system, psychopathy is strongly linked with re-offending, particularly of a violent nature.
In the general population, psychopathy is associated with drug dependence, homelessness, and other personality disorders. Some research even showed psychopathy predicted failure to follow COVID restrictions.
But sociopathy is less established as a key risk factor in identifying people at heightened risk of harm to others. And sociopathy is not a reliable indicator of future antisocial behaviour.
In a nutshell
Neither psychopathy nor sociopathy are classed as mental disorders in formal psychiatric diagnostic manuals. They are both personality traits that relate to antisocial behaviours and are associated with certain interpersonal, emotional and lifestyle characteristics.
Psychopathy is thought to have genetic, biological and psychological bases that places someone at greater risk of violating other people’s rights. But sociopathy is less clearly defined and its antisocial behaviours are the product of someone’s social environment.
Of the two, psychopathy has the greatest use in identifying someone who is most likely to cause damage to others.
Bruce Watt, Associate Professor in Psychology, Bond University and Katarina Fritzon, Associate Professor of Psychology, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: