Ayurveda’s Contributions To Science
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ayurveda’s Contributions To Science (Without Being Itself Rooted in Scientific Method)
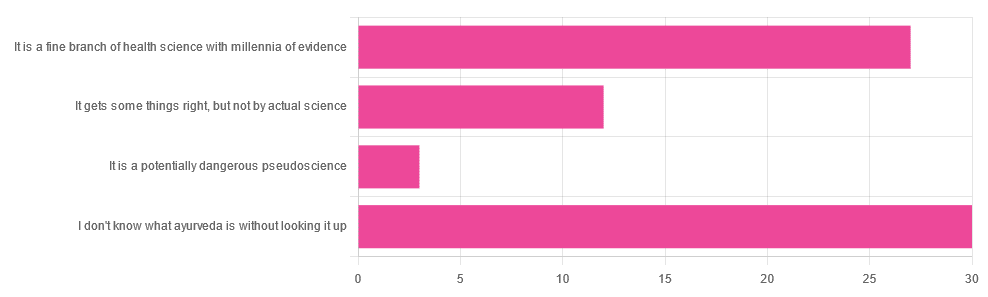
Yesterday, we asked you for your opinions on ayurveda, and got the above-depicted, below-described, set of responses. Of those who responded…
- A little over 41% said “I don’t know what ayurveda is without looking it up”
- A little over 37% said “It is a fine branch of health science with millennia of evidence”
- A little over 16% said “It gets some things right, but not by actual science”
- A little over 4% said “It is a potentially dangerous pseudoscience”
So, what does the science say?
Ayurveda is scientific: True or False?
False, simply. Let’s just rip the band-aid off in this case. That doesn’t mean it’s necessarily without merit, though!
Let’s put it this way:
- If you drink coffee to feel more awake because scientific method has discerned that caffeine has vasoconstrictive and adenosine-blocking effects while also promoting dopaminergic activity, then your consumption of coffee is evidence-based and scientific. Great!
- If you drink coffee to feel more awake because somebody told you that that somebody told them that it energizes you by balancing the elements fire (the heat of the coffee), air (the little bubbles on top), earth (the coffee grinds), water (the water), and ether (steam), then that is neither evidence-based nor scientific, but it will still work exactly the same.
Ayurveda is a little like that. It’s an ancient traditional Indian medicine, based on a combination of anecdotal evidence and supposition.
- The anecdotal evidence from ayurveda has often resulted in herbal remedies that, in modern scientific trials, have been found to have merit.
- Ayurvedic meditative practices also have a large overlap with modern mindfulness practices, and have also been found to have merit
- Ayurveda also promotes the practice of yoga, which is indeed a very healthful activity
- The supposition from ayurveda is based largely in those five elements we mentioned above, as well as a “balancing of humors” comparable to medieval European medicine, and from a scientific perspective, is simply a hypothesis with no evidence to support it.
Note: while ayurveda is commonly described as a science by its practitioners in the modern age, it did not originally claim to be scientific, but rather, wisdom handed down directly by the god Dhanvantari.
Ayurveda gets some things right: True or False?
True! Indeed, we covered some before in 10almonds; you may remember:
Bacopa Monnieri: A Well-Evidenced Cognitive Enhancer
(Bacopa monnieri is also known by its name in ayurveda, brahmi)
There are many other herbs that have made their way from ayurveda into modern science, but the above is a stand-out example. Others include:
- Ashwagandha: The Root of All Even-Mindedness?
- Boswellia serrata (Frankincense) Against Pain and Depression/Anxiety
Yoga and meditation are also great, and not only that, but great by science, for example:
- NCCIH | Yoga for Health: Clinical Guidelines, Scientific Literature, Info for Patients
- The Neuroscience of Mindfulness: How Mindfulness Alters the Brain and Facilitates Emotion Regulation
Ayurveda is a potentially dangerous pseudoscience: True or False?
Also True! We covered why it’s a pseudoscience above, but that doesn’t make it potentially dangerous, per se (you’ll remember our coffee example).
What does, however, make it potentially dangerous (dose-dependent) is its use of heavy metals such as lead, mercury, and arsenic:
Heavy Metal Content of Ayurvedic Herbal Medicine Products
Some final thoughts…
Want to learn more about the sometimes beneficial, sometimes uneasy relationship between ayurveda and modern science?
A lot of scholarly articles trying to bridge (or further separate) the two were very biased one way or the other.
Instead, here’s one that’s reasonably optimistic with regard to ayurveda’s potential for good, while being realistic about how it currently stands:
Development of Ayurveda—Tradition to trend
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Fish Oil Can Harm Your Brain

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Omega-3 fatty acids have many benefits for the health, including for the brain!
We wrote about some of them, here: What Omega-3 Fatty Acids Really Do For Us
There are even some less well-known benefits, such as: Why Healthy Teeth May Depend On Omega-3 & Exercise
Now, the press has not been all positive, for example: Fish Oil Can Backfire Without This Enzyme
But what’s this about omega-3s harming the brain?
Brain recovery impediment
Researchers (Dr. Eda Karakaya et al.) examined how omega-3 fatty acids from fish oil affect brain recovery, and the results were not happy ones.
In few words: the fish-derived omega-3 fatty acid EPA (eicosapentaenoic acid) accumulated in the brain and was linked to reduced recovery capacity after injury.
Further, EPA altered cortical gene programs by suppressing pathways involved in vascular repair* and extracellular matrix organization while increasing lipid metabolism activity.
*And this is critical. Regular 10almonds readers will remember that we often say “what’s good for your heart is good for your brain”, and it’s because the former feeds the latter, with nutrients, oxygen, etc, and also ultimately takes away detritus (yes, it’s the glymphatic system that does it directly, but without good blood flow, there’s nowhere for it to usefully drain to). So all this means that if cerebrovascular repair is impaired, then ultimately, brain maintenance will be impaired too.
More than just that, in human brain microvascular endothelial cells, EPA reduced the ability to form repair networks under conditions promoting fatty acid use.
And while no ethics board would let the researchers take brain slices from living human volunteers to look at under the microscope, postmortem brain samples from humans with chronic traumatic encephalopathy showed disrupted fatty acid balance and vascular-related gene changes consistent with EPA-linked effects.
In other words: a further smoking gun that strongly suggests (albeit does not outright prove, in this case) “EPA did this”.
There is one thing that’s not completely bad news for fish oil here, which is that DHA (docosahexaenoic acid), another omega-3 fatty acid, did not show the same negative effects and remains associated with normal brain structure.
But since fish oil contains both EPA and DHA in generous amounts, there’s a limit to how helpful this is:
❝Fish oil supplements are everywhere, and people take them for a range of reasons, often without a clear understanding of their long-term effects
But in terms of neuroscience, we still don’t know whether the brain has resilience or resistance to this supplement. That’s why ours is the first such study in the field.❞
~ Dr. Onder Albaryam, a colleague of Dr. Karakaya, and part of the “et al.” in this study
You can read the paper in full, here: Eicosapentaenoic acid reprograms cerebrovascular metabolism and impairs repair after brain injury, with relevance to chronic traumatic encephalopathy
Want to do better for your brain?
You do have other options!
For example, as well as the difference between EPA and DHA that we talked about above, there are also plant-based omega-3s that just have ALA (and not EPA or DHA) which the body can convert to whatever omega-3 form it needs (just like the fish did, for we too are animals that can do that, and for this reason our liver fats would, if healthy, also be a good source of EPA/DHA if something were to predate on us).
For more on that, check out: Omega-3s: Different Sources, Different Benefits?
Enjoy!
Share This Post
-

How the Brain Connects to Cognitive & Behavioral Change – by Dr. Robert Lavine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From the title, you could be forgiven for expecting this to be a dry book of neurology or perhaps psychology. However! While the author is indeed a neurologist and is usually ears-deep in academia, this work here is actually mostly about brain-hacking.
In other words, it pertains to improving one’s cognitive function by an assortment of means, ranging from nootropics (this book makes the case for supplementing with oxytocin), to cognitive behavioral therapy (CBT), behavioural adjustments (thematically linked to the aforementioned CBT, but also quite distinct in application) and environmental factors (which this book does not consider in great depth, but does cover clearly).
The book is arranged around various problems as the topic headers, with discussion of what’s going wrong and why, and in each case at least one explanation of how it can be corrected.
Legal disclaimers abound throughout, and the book is not offering medical advice per se. However, for those interested—for academic or practical reasons—the pointers are there to get the reader heading in the right direction.
The style, therefore, is accessible and relatively jargon-free, and is content to seem what it really is: a book written by an academic, but for a lay audience.
Bottom line: if you’d like to better understand your brain with an emphasis on the practicalities and how to make it work better, this book can help with that.
Share This Post
-
Does Your Hair Ever Stop Growing?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
…and how long can it grow?
Staying ahead
Because scalp hair usually stops growing after 5–7 years and then sheds, the average maximum length is about 75–105cm, though genetics, hormones, and health can extend or shorten this.
But that’s scalp hair; scalp follicles typically grow hair for 5–7 years at roughly 15cm per year, while eyelash follicles have a much shorter growth phase, limiting lashes to around 1cm.
You may be wondering why different body hair behaves differently: fibroblasts in each follicle determine whether hair becomes scalp hair, eyelashes, or other body hair, controlling growth rate, thickness, shape, and color based on location.
In the case of current world record-holder Xie Quiping, her record-breaking hair length over 5 meters resulted from an unusually long anagen (growth) phase, combined with helpful genetics, good health, and minimal breakage.
As for things that can get in the way:
- Why baldness happens: follicles can shrink and eventually stop producing hair when epithelial stem cells decline, while testosterone-related effects can also interfere with growth signals.
- Why hair turns gray: follicles gradually lose melanocyte stem cells, reducing pigment production and leading to gray or white hair, which in turn is usually more brittle, thus breaks more easily, thus does not usually reach the same lengths as pre-gray hair.
As for whether we can speed up hair growth: technically no, as no known treatment can make hair exceed its biological growth speed. But! Some treatments can reduce hair loss or improve hair condition, which will result in the appearance of quicker-growing hair, since the overall length will increase (due to reduced breakage and reduced shedding).
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The 9 “Healthy” Hair Habits That Are Damaging Your Hair
Take care!
Share This Post



Related Posts
-
Open Your Hips With Better Joint Mechanics (Here’s How)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most people stretch hips incorrectly, and pushing through painful stretches often leads to little or no progress, which can be discouraging to say the least.
Here’s how to cut through all that and get the results you need:
More than just stretching
Effective hip mobility also requires joint capsule activation, muscle tension release, and nervous system safety. These four exercises meet those needs:
- Banded lunge hip mobilization: in a lunge, loop a resistance band across the hip of your lead leg, extend your back leg, and push your front knee outwards without hip rotation or spinal arching. Hold 15–20 seconds, repeat.
- Weighted butterfly stretch: sit with your feet together, knees out, and rest light/moderate dumbbells on each knee to gently press them down; relax fully, hold 2–3 seconds, repeat 8–10 times.
- Seated hinge with barbell: sit on a bench with your knees bent and your hips open; hold a barbell at your shoulders, brace your core, and hinge forward at hips while keeping your spine neutral; you should feel the stretch in your hips, glutes, and groin. Pause 2–3 seconds, repeat 8–12 times.
- Frog stretch with sliders and weight: hold the “frog” position (knees wide, feet out), for 30–60 seconds; add sliders to move your hips up/down, then rest a plate on your hips and hold another 30–60 seconds.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Most Underrated Hip Mobility Exercise (Not Stretching)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
5 Best Bodyweight Exercises For Overall Mobility
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For those who don’t love doing long complicated routines, enjoy the most bang-for-buck minimum effort for maximum results:
Sometimes a little counts for a lot
The top 5 are:
- Primal squat: also called Asian squat, Slav squat, resting squat, sitting squat, deep squat, and probably some more names… this one’s for gaining and maintaining mobile hips, stable ankles, and healthy knees; you can progress this by leaning against a foam roller or ball on a wall, or placing a wedge under your heels; use microdoses throughout the day for lasting benefits (e.g. instead of stooping over to do various, deep squat instead).
- Dead hang: hang passively from a bar to improve shoulder mobility, decompress your spine, and strengthen your wrists; if necessary, you can modify it by keeping toes on ground and increasing weight over time.
- Cossack squat: a wide-stance side squat to stretch adductors and improve hamstring mobility; feet can be flat on the ground (more adductors, harder on ankles) or toes up (more hamstrings, easier on ankles), and you can control the depth so that you can rise back up without sinking into your joints (which would put undue stress on them).
- Single-leg deadlift: stand on one leg and hinge forwards to stretch and contract your hamstring; keep your hips and head aligned; your back leg can be straight or bent; you can use some kind support for balance if necessary, but it’s best to try to progress without that if you can.
- ATG split squat: take a large stride with torso upright, driving hips and knee forwards and downwards to stretch your hip flexors and improve your ankle mobility; tap your back knee to the ground if you can, then press through your front heel to rise.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Secret To Better Squats: Foot, Knee, & Ankle Mobility
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Heal Your Nervous System – by Dr. Linnea Passaler
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book focuses on the oft-overlooked connection between nervous system dysregulation (i.e. sympathetic nervous system dominance, keeping the brain in “may have to fight for my life at any moment” mode) and the many symptoms—mental and physical—that can arise as a result.
While there is a lot of theory explained in here, there’s practicality too, providing the reader with tools to assess our own levels of nervous system dysregulation and what factors affect that.
In particular in that category, a lot of value is delivered in terms of practical guidance on avoiding common pitfalls in the healing journey. Dr. Passaler discusses the four biggest mistakes people make when attempting to heal, and gives clear strategies to sidestep each of them, with exercises to do and habits to implement.
Another thing that sets this book apart from many of its genre is her emphasis on the importance of sequencing healing practices in the right order. By offering a structured approach, the book helps us implement healing practices without getting overwhelmed or hitting the proverbial brick wall and getting frustrated, which makes a big difference.
The style is easy-to-understand pop-science, albeit with a reassuring 20 pages of references at the back.
Bottom line: if you feel like “peace of mind” is something that’s always just out of reach, this book can help you to get where you need to be, physically as well as mentally.
Click here to check out Heal Your Nervous System, and get things into much better order!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: