

How To Unfatty A Fatty Liver
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Unfatty A Fatty Liver
In Greek mythology, Prometheus suffered the punishment of being chained to a rock, where he would have his liver eaten by an eagle, whereupon each day his liver would grow back, only to be eaten again the next day.
We mere humans who are not Greek gods might not be able to endure quite such punishment to our liver, but it is an incredibly resilient and self-regenerative organ.
In fact, provided at least 51% of the liver is still present and correct, the other 49% will regrow. Similarly, damage done (such as by trying to store too much fat there due to metabolic problems, as in alcoholic or non-alcoholic fatty liver disease) will reverse itself in time, given the chance.
The difference between us and Prometheus
In the myth, Prometheus had his liver regrow overnight every night. But he was a Titan (one of the pre-Olympian gods), and we are not.
In other words: ours don’t recover quite so quickly.
Indeed, the science has good and bad news for us:
❝Liver recolonization models have demonstrated that hepatocytes have an unlimited regenerative capacity. However, in normal liver, cell turnover is very slow.❞
~ Michalopoulos and Bhusan (2020)
Read more: Liver regeneration: biological and pathological mechanisms and implications
If it regenerates, why do people need transplants, and/or die of liver disease?
There are some diseases of the liver that inhibit its regenerative abilities, or (as in the case of cancer) abuse them to our detriment. However, in the case of fatty liver disease, the reason is usually simple:
If the lifestyle factors that caused the liver to become fatty are still there, then its regenerative abilities won’t be able to keep up with the damage that is still being done.
Can we speed it up at all?
Yes! The first and most important thing is to minimize how much ongoing harm you are still doing to it, though.
- If you drink alcohol, stop. According to the WHO, the only amount of alcohol that is safe for you is zero.
- You might like our previous article: How To Reduce Or Quit Alcohol
- Consider your medications, and find out which place a strain on the liver. Many medications are not optional; you’re taking them for an important reason, so don’t quit things without checking with your doctor. Medications that strain the liver include, but are by no means limited to:
- Many painkillers, including acetaminophen/paracetamol (e.g. Tylenol), and ibuprofen
- Some immunosuppressant drugs, including azathioprine
- Some epilepsy drugs, including phenytoin
- Some antibiotics, including amoxicillin
- Statins in general
Note: we are not pharmacists, nor doctors, let alone your doctors.
Check with yours about what is important for you to take, and what alternatives might be safe for you to consider.
Dietary considerations
While there are still things we don’t know about the cause(s) of non-alcoholic fatty liver disease, there is a very strong association with a diet that is:
- high in salt
- high in refined carbohydrates
- e.g. white flour and white flour products such as white bread and white pasta; also the other main refined carbohydrate: sugar
- high in red meat
- high in non-fermented dairy
- high in fried foods.
So, consider minimizing those, and instead getting plenty of fiber, and plenty of lean protein (not from red meat, but poultry and fish are fine iff not fried; beans and legumes are top-tier, though).
Also, hydrate. Most people are dehydrated most of the time, and that’s bad for all parts of the body, and the liver is no exception. It can’t regenerate if it’s running on empty!
Read more: Foods To Include (And Avoid) In A Healthy Liver Diet
How long will it take to heal?
In the case of alcoholic fatty liver disease, it should start healing a few days after stopping drinking. Then, how long it takes to fully recover depends on the extent of the damage; it could be weeks or months. In extreme cases, years, but that is rare. Usually if the damage is that severe, a transplant is needed.
In the case of non-alcoholic fatty liver disease, again it depends on the extent of the damage, but it is usually a quicker recovery than the alcoholic kind—especially if eating a Mediterranean diet.
Read more: How Long Does It Take For Your Liver To Repair Itself?
Take good care of yourself!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Dry Needling for Meralgia Paresthetica?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Could you address dry needling, who should administer it, and could it be a remedy for meralgia paresthetica? If not, could you speak to home-based remedies for meralgia paresthetica? Thank you?❞
We’ll need to take a main feature some time to answer this one fully, but we will say some quick things here:
- Dry needling, much like acupuncture, has been found to help with pain relief.
- Meralgia paresthetica, being a neuropathy, may benefit from some things that benefit people with peripheral neuropathy, such as lion’s mane mushroom. There is definitely not research to support this hypothesis yet though (so far as we could find anyway; there is plenty to support lion’s mane helping with nerve regeneration in general, but nothing specific for meralgia paresthetica).
Some previous articles you might enjoy meanwhile:
- Pinpointing The Usefulness Of Acupuncture
- Science-Based Alternative Pain Relief
- Peripheral Neuropathy: How To Avoid It, Manage It, Treat It
- What Does Lion’s Mane Actually Do, Anyway?
Take care!
Share This Post
-

How we can prepare for future public health emergencies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The U.S. is experiencing an increasing number of disease outbreaks and extreme weather events. While state and national preparedness for public health emergencies has improved in some areas, dangerous gaps remain, says a recent report from Trust for America’s Health.
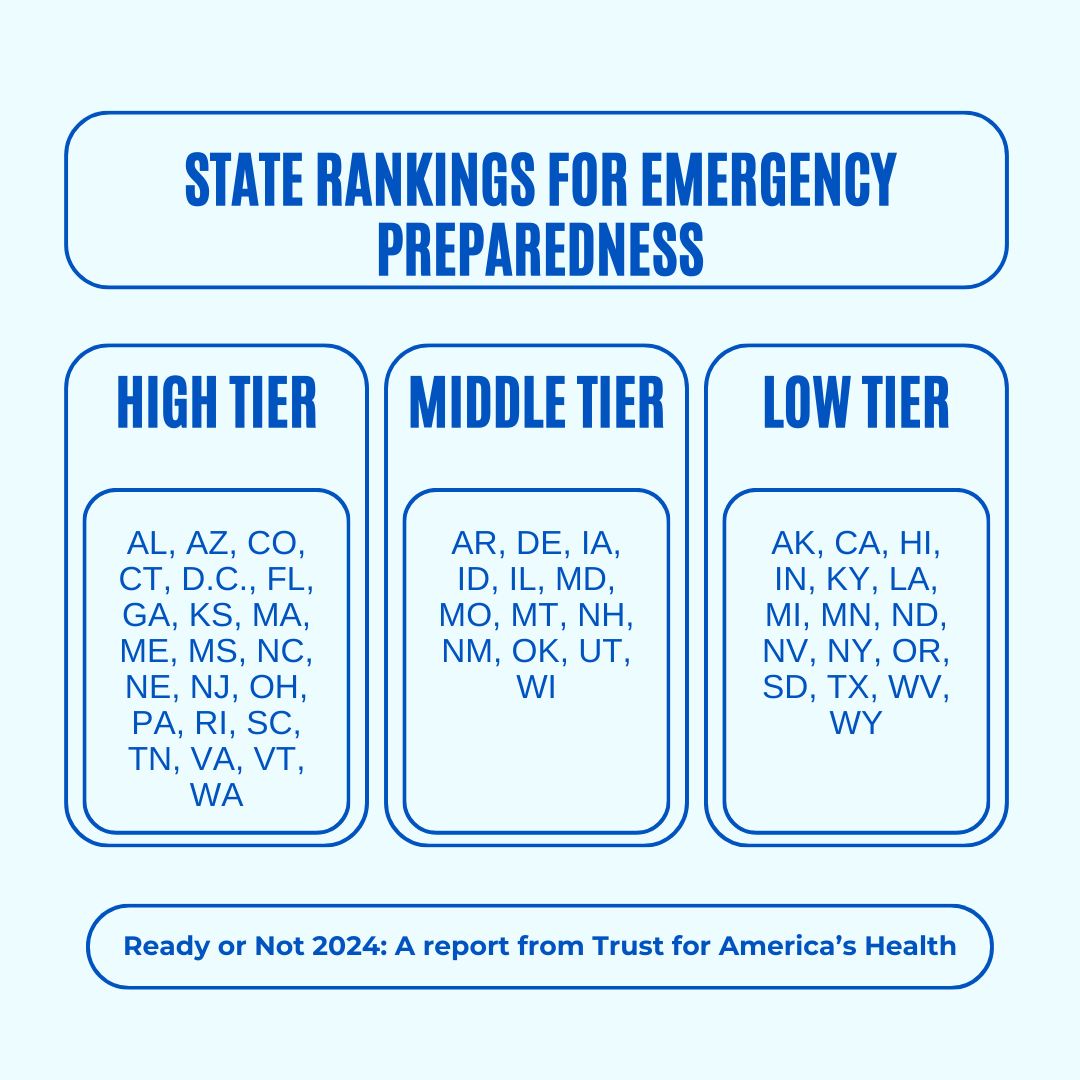
Titled, “Ready or Not 2024: Protecting the Public’s Health from Diseases, Disasters, and Bioterrorism,” the report identifies gaps in national and state preparedness for public health emergencies and provides recommendations for improvement.
Using nine key indicators, the report categorizes all U.S. states and the District of Columbia into three readiness levels: high, medium, and low. The writers hope the report will help policymakers in under-performing states improve public health infrastructure.
Read on to learn more about what the research found and how we can individually prepare for future public health emergencies.
There’s work to be done

The report highlights areas with strong performance as well as those that need improvement.
Some areas with strong performance:
- State public health funding: Most states and the District of Columbia either maintained or increased their public health funding during the 2023 fiscal year.
- Health care labor force preparedness: Most states have started expanding the health care labor force for improved emergency response. As of 2023, 39 states participated in the Nurse Licensure Compact, which allows nurses to work in multiple member states without the need for additional state licenses.
Some areas that need improvement:
- Hospital safety scores: Only 25 percent of acute care hospitals earned the highest patient safety grade in fall 2023. These scores measure health care-associated infection rates, intensive care unit capacity, and other metrics. More high-scoring hospitals would improve preparedness for future public health emergencies.
- Access to paid time off: From March 2018 to March 2023, only 55 percent of U.S. workers used paid time off. Access to paid time off is important for reducing the spread of infectious diseases.
We can all do our part by staying up to date on vaccines
While the report focuses on policy changes that would improve emergency preparedness, Trust for America’s Health’s research identifies one way that we can individually prepare for future public health emergencies: staying up to date on vaccines.
The report found that during the 2022-2023 flu season, only 49 percent of those eligible for the flu vaccine received it. Public health experts are concerned that false claims about COVID-19 vaccines have resulted in overall vaccine hesitancy.
A decline in vaccination rates has led to an uptick in life-threatening, vaccine-preventable diseases, such as measles. Increasing vaccine uptake would prevent the spread of vaccine-preventable diseases and reduce strain on hospital systems during public health crises.
Make sure that you and your children have received all recommended vaccines to prevent severe illness, hospitalization, and death. Learn more about recommended vaccines for adults and children from the CDC.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post
-

Gut Health for Women – by Aurora Bloom
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First things first: though the title says “For Women”, almost all of it applies to men too—and the things that don’t apply, don’t cause a problem. So if you’re cooking for your family that contains one or more men, this is still great.
Bloom gives us a good, simple, practical introduction to gut health. Her overview also covers gut-related ailments beyond the obvious “tummy hurts”. On which note:
A very valuable section of this book covers dealing with any stomach-upsets that do occur… without harming your trillions of tiny friends (friendly gut microbiota). This alone can make a big difference!
The book does of course also cover the things you’d most expect: things to eat or avoid. But it goes beyond that, looking at optimizing and maintaining your gut health. It’s not just dietary advice here, because the gut affects—and is affected by—other lifestyle factors too. Ranges from mindful eating, to a synchronous sleep schedule, to what kinds of exercise are best to keep your gut ticking over nicely.
There’s also a two-week meal plan, and an extensive appendix of resources, not to mention a lengthy bibliography for sourcing health claims (and suggesting further reading).
In short, a fine and well-written guide to optimizing your gut health and enjoying the benefits.
Share This Post



-

What Too Much Exercise Does To Your Body And Brain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Get more exercise” is a common rallying-cry for good health, but it is possible to overdo it. And, this is not just a matter of extreme cases of “exercise addiction”, but even going much above certain limits can already result in sabotaging one’s healthy gains. But how, and where does the line get drawn?
Too Much Of A Good Thing
The famous 150 minutes per week of moderate exercise (or 75 minutes of intense exercise) is an oft-touted figure. This video, on the other hand, springs for 5 hours of moderate exercise or 2.5 hours intense exercise as a good guideline.
We’re advised that going over those guidelines doesn’t necessarily increase health benefits, and on the contrary, may reduce or even reverse them. For example, we are told…
- Light to moderate running reduces the risk of death, but running intensely more than 3 times a week can negate these benefits.
- Extreme endurance exercises, like ultra-marathons, may cause heart damage, heart rhythm disorders, and artery enlargement.
- Women who exercise strenuously every day have a higher risk of heart attacks and strokes compared to those who exercise moderately.
- Excessive exercise in women can lead to the “female athlete triad” (loss of menstruation, osteoporosis, and eating disorders).
- In men, intense exercise can lower libido due to fatigue and reduced testosterone levels.
- Both men and women are at increased risk of overuse injuries (e.g., tendinitis, stress fractures) and impaired immunity from excessive exercise.
- There is a 72-hour window of impaired immunity after intense exercise, increasing the risk of infections.
Exercise addiction is rare, though, with this video citing “around 1 million people in the US suffer from exercise addiction”.
For more on finding the right balance, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Beat Food Addictions!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When It’s More Than “Just” Cravings

This is Dr. Nicole Avena. She’s a research neuroscientist who also teaches at Mount Sinai School of Medicine, as well as at Princeton. She’s done a lot of groundbreaking research in the field of nutrition, diet, and addition, with a special focus on women’s health and sugar intake specifically.
What does she want us to know?
Firstly, that food addictions are real addictions.
We know it can sound silly, like the famous line from Mad Max:
❝Do not, my friends, become addicted to water. It will take hold of you and you will resent its absence!❞
As an aside, it is actually possible to become addicted to water; if one drinks it excessively (we are talking gallons every day) it does change the structure of the brain (no surprise; the brain is not supposed to have that much water!) causing structural damage that then results in dependency, and headaches upon withdrawal. It’s called psychogenic polydipsia:
But back onto today’s more specific topic, and by a different mechanism of addiction…
Food addictions are dopaminergic addictions (as is cocaine)
If you are addicted to a certain food (often sugar, but other refined carbs such as potato products, and also especially refined flour products, are also potential addictive substances), then when you think about the food in question, your brain lights up with more dopamine than it should, and you are strongly motivated to seek and consume the substance in question.
Remember, dopamine functions by expectation, not by result. So until your brain’s dopamine-gremlin is sated, it will keep flooding you with motivational dopamine; that’s why the first bite tastes best, then you wolf down the rest before your brain can change its mind, and afterwards you may be left thinking/feeling “was that worth it?”.
Much like with other addictions (especially alcohol), shame and regret often feature strongly afterwards, even accompanied by notions of “never again”.
But, binge-eating is as difficult to escape as binge-drinking.
You can break free, but you will probably have to take it seriously
Dr. Avena recommends treating a food addiction like any other addiction, which means:
- Know why you want to quit (make a list of the reasons, and this will help you stay on track later!)
- Make a conscious decision to genuinely quit
- Learn about the nature of the specific addiction (know thy enemy!)
- Choose a strategy (e.g. wean off vs cold turkey, and decide what replacements, if any, you will use)
- Get support (especially from those around you, and/but the support of others facing, or who have successfully faced, the same challenge is very helpful too)
- Keep track of your success (build and maintain a streak!)
- Lean into how you will better enjoy life without addiction to the substance (it never really made you happy anyway, so enjoy your newfound freedom and good health!)
Want more from Dr. Avena?
You can check out her column at Psychology Today here:
Psychology Today | Food Junkie ← it has a lot of posts about sugar addiction in particular, and gives a lot of information and practical advice
You can also read her book, which could be a great help if you are thinking of quitting a sugar addiction:
Sugarless: A 7-Step Plan to Uncover Hidden Sugars, Curb Your Cravings, and Conquer Your Addiction
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Cranberries vs Gooseberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cranberries to gooseberries, we picked the gooseberries.
Why?
It wasn’t close:
In terms of macros, cranberries have more carbs while gooseberries have more fiber, so that’s a win for gooseberries. A nominal win as the differences aren’t huge, but clear enough to be a win nevertheless.
In the category of vitamins, cranberries have more vitamin E, while gooseberries have more of vitamins A, B1, B2, B3, B5, B6, B7, B9, and C, winning easily.
Looking at minerals next, cranberries have more manganese, while gooseberries have more calcium, copper, iron, magnesium, phosphorus, potassium, selenium, and zinc, scoring their third win in a row by quite a margin.
In other considerations, cranberries have some special properties that amount to a mixed bag of pros and cons (see details in the “learn more” below), while gooseberries are higher in polyphenols. Since cranberries have good and bad things in this round while gooseberries have just good, we say gooseberries in this round, too.
Adding up the sections makes for a clear overall win for gooseberries, but by all means enjoy either or both, as diversity is best (unless one of the contraindications for cranberries applies, in which case, skip those)!
Want to learn more?
You might like:
Health Benefits Of Cranberries (But: You’d Better Watch Out) ← cranberries’ bonus properties (including: famously very good at decreasing UTI risk) come with some warnings, including that they may increase the risk of kidney stones if you are prone to such, and also that cranberries have anti-clotting effects, which are great for heart health but can be a risk of you’re on blood thinners or have a bleeding disorder.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:



