How to Permanently Loosen a Tight Psoas
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What Is Your Psoas?
Your psoas is a deep muscle in your lower back and hip area that connects your spine to your thigh bone. It helps you bend your hips and spine, making it a hip flexor.
In today’s video, Your Wellness Nerd (the YouTube channel behind the video below) has revealed some great tips on loosening said tight hip flexors!
How to loosen them
First off, the big reveal…your tight psoas is likely stemming from an overlooked cause: your lower back! The video kicks off with a simple technique to loosen up that stiff area in your lower back. All you need is a foam roller.
But, before diving into the exercises, it’s essential to gauge your current flexibility. A basic hip flexor stretch serves as a pre-test.
Note: the goal here isn’t to stretch, but rather to feel how tight you are.
After testing, it’s time to roll…literally. Working through the lower back, use your roller or tennis ball to any find stiff spots and loosen them out; those spots are likely increasing the tension on your psoas.
After some rolling, retest with the hip flexor stretch. Chances are, you’ll feel more mobility and less tightness right away.
Note: this video focuses on chronic psoas issues. If you have sore psoas from a muscular workout, you may want to read our piece on speeding up muscle recovery.
Is That All?
But wait, there’s more! The video also covers two more exercises specifically targeting the psoas. This one’s hard to describe, so we recommend watching the video. However, to provide an overview, you’re doing the “classic couch stretch”, but with a few alterations.
Next, the tennis ball technique zeroes in on specific tight spots in the psoas. By lying on the ball and adjusting its position around the hip area, you can likely release some deeply held tension.
Additionally, some of our readers advocate for acupuncture for psoas relief – we’ve done an acupuncture myth-busting article here for reference.
Other Sources
If you’re looking for some more in-depth guides on stretching your psoas, and your body in general, we’ve made a range of 1-minute summaries of books that specifically target stretching:
- 11 Minutes to Pain-Free Hips (perfect for psoas muscles)
- Stretching Scientifically
- Stretching & Mobility
- Stretching to Stay Young
The final takeaway? If you’re constantly battling tight psoas muscles despite trying different exercises and stretches, it might be time to look at your lower back and your daily habits. This video isn’t just a band-aid fix; it’s about addressing the root cause for long-term relief:
How did you find that video? If you’ve discovered any great videos yourself that you’d like to share with fellow 10almonds readers, then please do email them to us!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Better Than Aspirin vs Cardiovascular Disease

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Using daily low-dose aspirin to reduce cardiac risk (mostly: atherothrombosis) has been a popular American pastime for some decades now, and it does work!
However, there’s a catch:
Low-dose aspirin lowers the risk of atherothrombosis by inhibiting platelet aggregation, but at the cost of increasing bleeding risk (especially gastrointestinal). The tradeoff is further complicated by the fact that aspirin improves nonfatal cardiovascular outcomes but does not significantly reduce cardiovascular or all-cause mortality.
In other words: speaking in statistical generalizations of course, it may improve your recovery from minor cardiac events but is unlikely to help against fatal ones.
We wrote about this here: Aspirin, CVD Risk, & Potential Counter-Risks
The current prevailing professional (amongst cardiologists) consensus is that it may broadly be recommended for secondary prevention of atherosclerotic cardiovascular disease (ASCVD), i.e. if you have a history of CVD, but usually not for primary prevention (i.e. if you have no history of CVD). Note: this means personal history, not family history.
There are some more considerations than just that, though, and a simplified flowchart of those other considerations looks something like this:
- No for primary prevention ( (i.e. you have no history of ASCVD)
- …except in select adults aged 40–70 (not above or below that range) with higher ASCVD risk and/but only if you also have no increased bleeding risk.
- Yes for secondary prevention (i.e. if you already have ASCVD)
- …and if you want more details on this, please see the above-linked article!
yes, but…
For those in the “yes” category, there is now a strong argument for early discontinuation of low-dose aspirin use.
Researchers (Dr. Valeria Paradies et al.) investigated this in an open-label randomized controlled trial across 40 European centers with 1,942 myocardial infarction patients who had complete revascularization and one month of uneventful dual antiplatelet therapy (DAPT). In other words, exactly the people in the “yes” category above.
DAPT, by the way, is what it sounds like and refers to the use of two antiplatelet therapies at once, namely:
- low-dose aspirin
- some kind of P2Y12 inhibitor
The P2Y12 inhibitor is also what it sounds like (it inhibits P2Y12), but that’s not a very useful explanation, so: it blocks the P2Y12 receptor on platelets, so that platelets don’t get activated by passing adenosine diphosphate, so they don’t aggregate (stick together), so your blood doesn’t clot.
When we say “some kind of P2Y12 inhibotor”, we’re not being whimsical, by this we mean there are many kinds, but common kinds include:
- Clopidogrel: widely used, low bleeding risk, variable effect due to genetic metabolism differences
- Prasugrel: more potent, faster onset, higher bleeding risk, often avoided in older patients or those with prior stroke (including any transient ischemic attack)
- Ticagrelor: potent, reversible inhibitor, improves outcomes compared to clopidogrel but can cause breathing difficulties and increases bleeding risk
What they found: looking at various metrics (death, myocardial infarction, stent thrombosis, stroke, or major bleeding), the results showed:
- DAPT was not better than a P2Y12 inhibitor alone (some metrics were slightly better or worse in one group than the other, but the differences were minimal, often around 0.1% difference one way or the other, and if we average out the differences, the result is “no real difference”)
- P2Y12 inhibitor-only patients enjoyed significantly less bleeding (less than half the bleeding of the DAPT patients)
So, with all that in mind, the take-away here seems to be “add aspirin if you’d like to bleed 2x as much“
Now, the researchers are technically arguing only for this decision (“stop the aspirin”) to be made after one month of DAPT first.
Why one month of DAPT first? Because this study started after one month of uneventful DAPT, as their baseline, to screen out any patients who had something go wrong in the first month, which would be confounding.
In other words, while they’re saying “stopping aspirin after one month and continuing P2Y12 inhibitor alone is safe, maintains ischemic protection, and reduces bleeding risk”, this is because that is what their results show, and, being scientists, they can only speak for what the study actually tested, and cannot speak for the first, untested month.
It’s a bit like how antidepressants (for example) are only tested on people who have had depressive symptoms for a given period of time, but that in practical terms, that doesn’t really mean they only becomes safe and affective after that given period of time. It just means, science didn’t have the opportunity of testing it at day 1, so can only speak for “after t period of time”
Back to the study at hand, you can find the paper here: Early Discontinuation of Aspirin after PCI in Low-Risk Acute Myocardial Infarction
Which P2Y12 inhibitor?
Here’s a big (n=28,982) study in patients with established coronary artery disease that doesn’t put P2Y12 inhibitors head-to-head, but did test clopidogrel vs aspirin head-to-head, and found:
- 8% less bleeding in the clopidogrel-only group compared to the aspirin-only group
- but, a high p-score (p=0.64), so this one cannot be strongly claimed, as the difference could be due to other factors
- 14% fewer major adverse cardiovascular or cerebrovascular events* in the clopidogrel-only group compared to the aspirin-only group
- this time, a very low p-score (p=0.0082), meaning this can be very strongly claimed; the researchers are about as sure about it as scientists get about anything)
*i.e. cardiovascular death, myocardial infarction, or stroke
About p-scores (or p-values): this is the probability (p) of something happening by chance. So for example, p=0 means “this result is literally impossible” and p=1 means “this result is absolutely predetermined as definitely what will happen”. Generally speaking, a p-score being under 0.05 is considered statistically significant.
In short: clopidogrel certainly didn’t cause any extra bleeding compared to aspirin (in fact, the clopidogrel group had 8% less bleeding, the scientists are just being cautious about claiming causality with regard to the bleeding), and beat aspirin head-to-head for effectiveness (14% fewer major adverse cardiovascular or cerebrovascular events, and this time, the scientists are very confident about the significance of the association).
You can find this paper here: Clopidogrel versus aspirin for secondary prevention of coronary artery disease: a systematic review and individual patient data meta-analysis
Want to learn more?
On the topic of medications commonly prescribed for cardiac health that may not actually help (and indeed, may harm):
Beta-Blockers: Useless vs Heart Attacks & Worse For Women?
Take care!
Share This Post
- No for primary prevention ( (i.e. you have no history of ASCVD)
-
Oral vaccines could provide relief for people who suffer regular UTIs. Here’s how they work
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In a recent TikTok video, Australian media personality Abbie Chatfield shared she was starting a vaccine to protect against urinary tract infections (UTIs).
Huge news for the UTI girlies. I am starting a UTI vaccine tonight for the first time.
Chatfield suffers from recurrent UTIs and has turned to the Uromune vaccine, an emerging option for those seeking relief beyond antibiotics.
But Uromune is not a traditional vaccine injected to your arm. So what is it and how does it work?

9nong/Shutterstock First, what are UTIs?
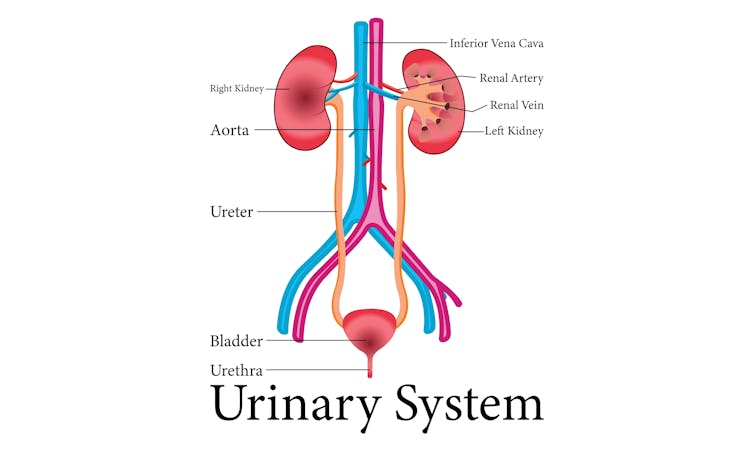
UTIs are caused by bacteria entering the urinary system. This system includes the kidneys, bladder, ureters (thin tubes connecting the kidneys to the bladder), and the urethra (the tube through which urine leaves the body).
The most common culprit is Escherichia coli (E. coli), a type of bacteria normally found in the intestines.
While most types of E. coli are harmless in the gut, it can cause infection if it enters the urinary tract. UTIs are particularly prevalent in women due to their shorter urethras, which make it easier for bacteria to reach the bladder.
Roughly 50% of women will experience at least one UTI in their lifetime, and up to half of those will have a recurrence within six months.
UTIs are caused by bacteria enterning the urinary system. oxo7051/Shutterstock The symptoms of a UTI typically include a burning sensation when you wee, frequent urges to go even when the bladder is empty, cloudy or strong-smelling urine, and pain or discomfort in the lower abdomen or back. If left untreated, a UTI can escalate into a kidney infection, which can require more intensive treatment.
While antibiotics are the go-to treatment for UTIs, the rise of antibiotic resistance and the fact many people experience frequent reinfections has sparked more interest in preventive options, including vaccines.
What is Uromune?
Uromune is a bit different to traditional vaccines that are injected into the muscle. It’s a sublingual spray, which means you spray it under your tongue. Uromune is generally used daily for three months.
It contains inactivated forms of four bacteria that are responsible for most UTIs, including E. coli. By introducing these bacteria in a controlled way, it helps your immune system learn to recognise and fight them off before they cause an infection. It can be classified as an immunotherapy.
A recent study involving 1,104 women found the Uromune vaccine was 91.7% effective at reducing recurrent UTIs after three months, with effectiveness dropping to 57.6% after 12 months.
These results suggest Uromune could provide significant (though time-limited) relief for women dealing with frequent UTIs, however peer-reviewed research remains limited.
Any side effects of Uromune are usually mild and may include dry mouth, slight stomach discomfort, and nausea. These side effects typically go away on their own and very few people stop treatment because of them. In rare cases, some people may experience an allergic reaction.
How can I access it?
In Australia, Uromune has not received full approval from the Therapeutic Goods Administration (TGA), and so it’s not something you can just go and pick up from the pharmacy.
However, Uromune can be accessed via the TGA’s Special Access Scheme or the Authorised Prescriber pathway. This means a GP or specialist can apply for approval to prescribe Uromune for patients with recurrent UTIs. Once the patient has a form from their doctor documenting this approval, they can order the vaccine directly from the manufacturer.
Antibiotics are the go-to treatment for UTIs – but scientists are looking at options to prevent them in the first place. Photoroyalty/Shutterstock Uromune is not covered under the Pharmaceutical Benefits Scheme, meaning patients must cover the full cost out-of-pocket. The cost of a treatment program is around A$320.
Uromune is similarly available through special access programs in places like the United Kingdom and Europe.
Other options in the pipeline
In addition to Uromune, scientists are exploring other promising UTI vaccines.
Uro-Vaxom is an established immunomodulator, a substance that helps regulate or modify the immune system’s response to bacteria. It’s derived from E. coli proteins and has shown success in reducing UTI recurrences in several studies. Uro-Vaxom is typically prescribed as a daily oral capsule taken for 90 days.
FimCH, another vaccine in development, targets something called the adhesin protein that helps E. coli attach to urinary tract cells. FimCH is typically administered through an injection and early clinical trials have shown promising results.
Meanwhile, StroVac, which is already approved in Germany, contains inactivated strains of bacteria such as E. coli and provides protection for up to 12 months, requiring a booster dose after that. This injection works by stimulating the immune system in the bladder, offering temporary protection against recurrent infections.
These vaccines show promise, but challenges like achieving long-term immunity remain. Research is ongoing to improve these options.
No magic bullet, but there’s reason for optimism
While vaccines such as Uromune may not be an accessible or perfect solution for everyone, they offer real hope for people tired of recurring UTIs and endless rounds of antibiotics.
Although the road to long-term relief might still be a bit bumpy, it’s exciting to see innovative treatments like these giving people more options to take control of their health.
Iris Lim, Assistant Professor in Biomedical Science, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Instead Of Chasing 10,000 Steps…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There is a better way:
Make it count
Fun fact: the widely promoted goal originated from a 1964 Japanese pedometer called the “Manpo-kei” (“10,000 steps meter”) as a marketing decision rather than from clinical research, largely because the Japanese kanji for 10,000 looks a bit like a walking person: 万
Walking is indeed very beneficial for many aspects of health (really: most aspects of health), and health benefits rise sharply when increasing from about 2,000 to 4,000 daily steps and continue improving up to 7,000–8,000 steps, after which additional benefits increase more gradually with diminishing returns; for example, although walking 15,000 steps is indeed generally better than 8,000, the extra health gains beyond about 8,000 steps are relatively small compared with the gains achieved at lower step counts.
For this reason, if you’re regularly getting in step counts in the 6,000–8,000 range, chances are you’re already getting most of the benefits.
So, what’s the promised “instead”?
Walking intensity matters: for most of us, how briskly we walk has a greater effect on health than just increasing the number of steps. For example, a leisurely stroll (lovely as it may be) provides fewer cardiovascular, metabolic, and balance benefits than a brisk walk walked at a moderate intensity.
So: instead of simply walking farther, aim to increase your walking pace to make your exercise more effective. A good goal is to try to accumulate 30 minutes of brisk walking each day, be it as one 30-minute walk, two 15-minute walks, or three 10-minute walks.
And if you really want to get optimal, then the best time to do it is after eating, as this greatly improves blood sugar control and digestion.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Share This Post



Related Posts
-
No-Needle Vaccination Against Many Avian/Human Flu Types
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
And other items from this week’s health news:
Intranasal spray provides broad protection
The flu isn’t fun, and kills many people very year. Needles, meanwhile, are often viewed as a necessary evil when it comes to protection against such. However, this newly-developed intranasal spray vaccinates against a wide variety of flu strains (including the bird flu strains currently rife in some parts of the US).
Most flu vaccines only target a few strains and (as you’re probably very aware) must be updated every year, as viruses mutate. They also don’t usually protect well against flu viruses that come from animals, like bird flu. The World Health Organization has called for better, more universal flu vaccines, and this research does just that.
The team used two methods:
- One method added a human gene to the flu virus, helping the immune system recognize and destroy infected cells more easily.
- The other method changed parts of the virus’s genetic code to make it weaker in humans but still easy to produce using current vaccine technology.
Both approaches showed strong results in trials, offering protection against multiple types of flu.
Read in full: Needle-free, live-attenuated influenza vaccines with broad protection against human and avian virus subtypes
Related: Flu vaccines are now available for 2025. What’s on offer and which one should I get?
How pets help in old age
It’s probably not news to you that pets can be a remedy against feelings of loneliness, but there’s more to it than that: daily routines like feeding, walking, and playing with a pet can bring structure to the day, reduce stress, and boost physical activity.
Pets also help a lot of older adults connect with their communities, simply because walking a dog or visiting a pet-friendly place often leads to casual conversations and new friendships, which can otherwise sometimes be thin on the ground.
However, owning a pet inevitably comes with some challenges, so it’s worth bearing them in mind up front. Some people may struggle with caring for pets that need a lot of exercise, or have health issues of their own, for example. It’s therefore especially important to choose a pet that fits your lifestyle and what you’re able to deal with on a daily basis—if indeed a pet is the right option for you at all (it’s not for everyone!).
Read in full: How pets enrich the lives of the elderly
Related: How To Beat Loneliness & Isolation
Beyond statins: a cholesterol-lowering pill that helps reduce heart disease risk
Heart disease is a leading killer in the US, and stroke is also rising up the “most fatal” list in recent years. Many opt to treat high cholesterol levels (which can contribute to hypertension, and thus cardiovascular disease, and thus also vascular dementia and stroke) with statins, but statins have their side effects too, many of which are very serious, and for some people, they may not even be that effective.
So, it might be worth knowing about a new contender: Obicetrapib.
This new drug was tested in a large (n=2,530) clinical trial and was shown to significantly reduce two major causes of heart disease: LDL (“bad”) cholesterol, and lipoprotein(a), also called: Lp(a).
The study participants were people with heart disease or inherited high cholesterol, and after 12 weeks, those taking Obicetrapib had lowered their LDL cholesterol by over 30%, and Lp(a) by about the same amount. This is important because many people cannot reach safe cholesterol levels with current medications, and there are no widely approved treatments for lowering Lp(a) yet.
Read in full: Cholesterol pill helps those at high risk of heart attack and stroke: Study
Related: Lower Cholesterol, Without Statins
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Body Recomposition: How To Get Toned Quickly
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Personal trainer Elisi Wolf explains how to cut straight to it:
As easy as 1-2-3
Many women say they want to “get toned,” which really means they want a body recomposition; looking leaner at the same weight is due to gaining muscle while losing fat—not weight.
Elisi says the sweet spot for effective recomposition is around 25% body fat, allowing for noticeable muscle gain and fat loss simultaneously, ending up with more like 21% body fat as a reasonable healthy end point to the recomposition phase (i.e., the point at which you’ll stop recomposing and start maintaining), though of course you might prefer more or less than that; that’s up to you.
How to do it, her way:
- Calculate maintenance calories: use a calorie calculator and subtract 400 to find your true maintenance; eat this amount for a week to confirm the scale doesn’t change
- Progress your workouts: consistently increase effort by adding weight, improving control (an oft-neglected factor that Elisi focuses on a lot in her training), and/or increasing movement (e.g. daily walks)
- Enjoy a high protein diet: protein is essential for muscle building, fat loss, and satiety; it also burns more energy to digest and keeps you full with fewer calories
About the progression: she recommends to, for example, start with 20 lb hip thrusts and increase weight every second week; eventually, this builds visible muscle without changing calories. Adapt the same model for your preferred exercises, of course.
About the protein: she also notes that we should not just increase protein intake, but also prioritize protein over carbs and fats; it’s not used for energy unless absolutely necessary, so most of it supports muscle gain. She advises that this works whether you still eat meat or enjoy a vegan diet—just ensure your protein intake is high and “clean” (i.e. unprocessed whole foods, or minimally-processed where some kind of processing is necessary—for example, cooking lentils is indeed a process).
About maintenance: once you’ve got to the body composition you want, you should find that your newly recomposed body is actually pretty easy to maintain, because muscle has a thermogenic effect, helping you burn more calories at rest and aiding fat loss (i.e. muscle “costs” calories just by being there—unlike fat, which triggers the body to slow down the metabolism to survive the famine for which we were surely preparing when we put the fat on).
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Can You Gain Muscle & Lose Fat At The Same Time? ← we got this question in our Q&A day a little while ago, and here was our answer. We went for a less numbers-based approach, and a more principles-based approach. Both ways work, so by all means pick whichever method you personally find better suits how you like to do things!
See also: Can We Do Fat Redistribution? ← the answer is “yes” and this article explains how
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Cold Truth About Respiratory Infections
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Pathogens That Came In From The Cold

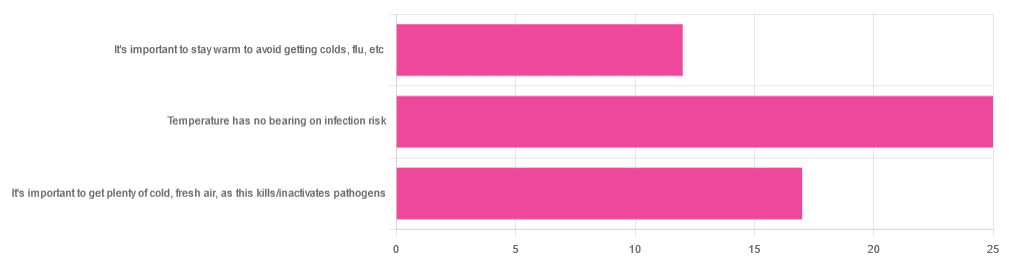
Yesterday, we asked you about your climate-themed policy for avoiding respiratory infections, and got the above-depicted, below-described, set of answers:
- About 46% of respondents said “Temperature has no bearing on infection risk”
- About 31% of respondents said “It’s important to get plenty of cold, fresh air, as this kills/inactivates pathogens”
- About 22% of respondents said “It’s important to stay warm to avoid getting colds, flu, etc”
Some gave rationales, including…
For “stay warm”:
❝Childhood lessons❞
For “get cold, fresh air”:
❝I just feel that it’s healthy to get fresh air daily. Whether it kills germs, I don’t know❞
For “temperature has no bearing”:
❝If climate issue affected respiratory infections, would people in the tropics suffer more than those in colder climates? Pollutants may affect respiratory infections, but I doubt just temperature would do so.❞
So, what does the science say?
It’s important to stay warm to avoid getting colds, flu, etc: True or False?
False, simply. Cold weather does increase the infection risk, but for reasons that a hat and scarf won’t protect you from. More on this later, but for now, let’s lay to rest the idea that bodily chilling will promote infection by cold, flu, etc.
In a small-ish but statistically significant study (n=180), it was found that…
❝There was no evidence that chilling caused any acute change in symptom scores❞
Read more: Acute cooling of the feet and the onset of common cold symptoms
Note: they do mention in their conclusion that chilling the feet “causes the onset of cold symptoms in about 10% of subjects who are chilled”, but the data does not support that conclusion, and the only clear indicator is that people who are more prone to colds generally, were more prone to getting a cold after a cold water footbath.
In other words, people who were more prone to colds remained more prone to colds, just the same.
It’s important to get plenty of cold, fresh air, as this kills/inactivates pathogens: True or False?
Broadly False, though most pathogens do have an optimal operating temperature that (for obvious reasons) is around normal human body temperature.
However, given that they don’t generally have to survive outside of a host body for long to get passed on, the fact that the pathogens may be a little sluggish in the great outdoors will not change the fact that they will be delighted by the climate in your respiratory tract as soon as you get back into the warm.
With regard to the cold air not being a reliable killer/inactivator of pathogens, we call to the witness stand…
Polar Bear Dies From Bird Flu As H5N1 Spreads Across Globe
(it was found near Utqiagvik, one of the northernmost communities in Alaska)
Because pathogens like human body temperature, raising the body temperature is a way to kill/inactivate them: True or False?
True! Unfortunately, it’s also a way to kill us. Because we, too, cannot survive for long above our normal body temperature.
So, for example, bundling up warmly and cranking up the heating won’t necessarily help, because:
- if the temperature is comfortable for you, it’s comfortable for the pathogen
- if the temperature is dangerous to the pathogen, it’s dangerous to you too
This is why the fever response evolved, and/but why many people with fevers die anyway. It’s the body’s way of playing chicken with the pathogen, challenging “guess which of us can survive this for longer!”
Temperature has no bearing on infection risk: True or False?
True and/or False, circumstantially. This one’s a little complex, but let’s break it down to the essentials.
- Temperature has no direct effect, for the reasons we outlined above
- Temperature is often related to humidity, which does have an effect
- Temperature does tend to influence human behavior (more time spent in open spaces with good ventilation vs more time spent in closed quarters with poor ventilation and/or recycled air), which has an obvious effect on transmission rates
The first one we covered, and the third one is self-evident, so let’s look at the second one:
Temperature is often related to humidity, which does have an effect
When the environmental temperature is warmer, water droplets in the air will tend to be bigger, and thus drop to the ground much more quickly.
When the environmental temperature is colder, water droplets in the air will tend to be smaller, and thus stay in the air for longer (along with any pathogens those water droplets may be carrying).
Some papers on the impact of this:
- Cold temperature and low humidity are associated with increased occurrence of respiratory tract infections
- A Decrease in Temperature and Humidity Precedes Human Rhinovirus Infections in a Cold Climate
So whatever temperature you like to keep your environment, humidity is a protective factor against respiratory infections, and dry air is a risk factor.
So, for example:
- If the weather doesn’t suit having good ventilation, a humidifier is a good option
- Being in an airplane is one of the worst places to be for this, outside of a hospital
Don’t have a humidifier? Here’s an example product on Amazon, but by all means shop around.
A crock pot with hot water in and the lid off is also a very workable workaround too
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: