

The Truth About Handwashing
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Washing Our Hands Of It
In Tuesdays’s newsletter, we asked you how often you wash your hands, and got the above-depicted, below-described, set of self-reported answers:
- About 54% said “More times per day than [the other options]”
- About 38% said “Whenever using the bathroom or kitchen
- About 5% said “Once or twice per day”
- Two (2) said “Only when visibly dirty”
- Two (2) said “I prefer to just use sanitizer gel”
What does the science have to say about this?
People lie about their handwashing habits: True or False?
True and False (since some people lie and some don’t), but there’s science to this too. Here’s a great study from 2021 that used various levels of confidentiality in questioning (i.e., there were ways of asking that made it either obvious or impossible to know who answered how), and found…
❝We analysed data of 1434 participants. In the direct questioning group 94.5% of the participants claimed to practice proper hand hygiene; in the indirect questioning group a significantly lower estimate of only 78.1% was observed.❞
Note: the abstract alone doesn’t make it clear how the anonymization worked (it is explained later in the paper), and it was noted as a limitation of the study that the participants may not have understood how it works well enough to have confidence in it, meaning that the 78.1% is probably also inflated, just not as much as the 94.5% in the direct questioning group.
Here’s a pop-science article that cites a collection of studies, finding such things as for example…
❝With the use of wireless devices to record how many people entered the restroom and used the pumps of the soap dispensers, researchers were able to collect data on almost 200,000 restroom trips over a three-month period.
The found that only 31% of men and 65% of women washed their hands with soap.❞
Source: Study: Men Wash Their Hands Much Less Often Than Women (And People Lie About Washing Their Hands)
Sanitizer gel does the job of washing one’s hands with soap: True or False?
False, though it’s still not a bad option for when soap and water aren’t available or practical. Here’s an educational article about the science of why this is so:
UCI Health | Soap vs. Hand Sanitizer
There’s also some consideration of lab results vs real-world results, because while in principle the alcohol gel is very good at killing most bacteria / inactivating most viruses, it can take up to 4 minutes of alcohol gel contact to do so, as in this study with flu viruses:
In contrast, 20 seconds of handwashing with soap will generally do the job.
Antibacterial soap is better than other soap: True or False?
False, because the main way that soap protects us is not in its antibacterial properties (although it does also destroy the surface membrane of some bacteria and for that matter viruses too, killing/inactivating them, respectively), but rather in how it causes pathogens to simply slide off during washing.
Here’s a study that found that handwashing with soap reduced disease incidence by 50–53%, and…
❝Incidence of disease did not differ significantly between households given plain soap compared with those given antibacterial soap.❞
Read more: Effect of handwashing on child health: a randomised controlled trial
Want to wash your hands more than you do?
There have been many studies into motivating people to wash their hands more (often with education and/or disgust-based shaming), but an effective method you can use for yourself at home is to simply buy more luxurious hand soap, and generally do what you can to make handwashing a more pleasant experience (taking a moment to let the water run warm is another good thing to do if that’s more comfortable for you).
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Parents of neurodivergent kids need support. But those who need it most often wait longer

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Parenting any young child is full of highs and lows.
In addition to these, parents and caregivers of children with neurodevelopmental conditions such as autism and attention-deficit hyperactivity disorder (ADHD) are more likely to face greater levels of strain and higher support needs. They are also more likely than other parents to experience poor mental health.
But our new research found when they experienced mental health concerns, these parents and carers also faced more barriers to accessing support than other parents.
Their children also experienced longer delays getting an initial neurodevelopmental assessment.
What we did
Our research used the Australian Child Neurodevelopment Research Registry to look at mental health concerns in 187 parents and carers of children referred for neurodevelopmental assessments in NSW between 2020 and 2023.
Neurodevelopmental assessments typically include evaluations of a child’s developmental, cognitive, language, social, motor and adaptive functioning. They are helpful for understanding a child’s strengths and challenges. These assessments help identify conditions such as autism, ADHD, communication disorders, and other developmental and learning delays.
Caregivers completed a questionnaire one month before their child’s assessment. They provided information about their own mental health symptoms, and the supports and services they used for themselves and their child.
We then looked at whether caregivers who reported more mental health concerns had different experiences compared to those with fewer concerns. In particular, we looked at whether their children received assessments at different ages, and whether they faced more barriers or accessed different types of supports.
What we found
We found 41.7% of parents and carers reported elevated mental health concerns, including anxiety, depression and ADHD symptoms. This is higher than in the general population, where about one in five adults (22%) experience a mental health condition each year.
These parents and carers reported needing more support and faced more barriers when trying to access supports for their family.
All caregivers noticed developmental delays in their children at around three years of age, replicating our past study. However, children of caregivers with mental health concerns were, on average, a full year older by the time they received a developmental assessment. Their children also had more emotional and behavioural challenges and support needs.
Caregivers with mental health challenges said they needed more support for themselves and their children, but found it hard to access these supports. They also wanted more access to parental respite, and they reported greater difficulty accessing psychological services and behavioural therapies for their children.
Barriers to accessing care included transport difficulties, trouble coordinating appointments, and a lack of knowledge about where to go or who to contact for help.
Our previous research shows families from financially disadvantaged backgrounds have greater difficulties accessing services and experience more barriers to care.
Support needs to extend to families
The new federal program Thriving Kids is being set up to support children with developmental concerns. But our results suggest for it to work well, it needs to take a whole-of-family approach and reach disadvantaged families early.
This means offering evidence-based support when it’s needed most, for both children and their caregivers. For example, some parents may need additional navigation supports to address family system needs. Caregivers may also need to be linked in with mental health supports for themselves.
The importance of integrated, family-focused care has also been highlighted in multiple government reports, including the National Children’s Mental Health and Wellbeing Strategy, the National Guideline for the assessment and diagnosis of autism, and the national ADHD guideline.
What can caregivers do now?
Parents and carers of children with neurodevelopmental conditions are often surprised when they’re advised to look after and prioritise their own needs too. By meeting their own needs, they will be in a better position to support their family.
Caregivers with mental health needs will require different types and amounts of supports for themselves and their children to thrive.
Talking with a health professional, such as your GP, can be a good first step. They can provide support recommendations, help you navigate your child’s care, and may also be able to provide links to parent support groups or respite care. Respite care can involve someone else looking after your child for a short period, so you can rest and have time for yourself.
Clinicians also need to step up
Some simple steps clinicians can take include:
1) Recognising and identifying parental distress
Many parents say they are rarely asked about how they are doing, even though they do a lot of work supporting their children.
Services can go a long way by helping to identify caregiver needs and discuss what supports might be needed.
During developmental assessments, clinicians may notice that caregivers are experiencing stress or mental health concerns. It’s important clinicians consider broader family supports when providing recommendations for the child.
2) Reducing stigma
Caregivers may need to feel safe to express their needs without judgement and to understand that looking after themselves is an important priority.
Clinicians can help by creating a safe space where caregivers can share their concerns, so they are more likely to seek and receive support.
3) Navigating and sharing information
Families often need support navigating care.
Clinicians can provide clear information and pathways to support, including local and online supports and services, parenting programs and caregiver respite services.
Kelsie Boulton, Senior Research Fellow in Child Neurodevelopment, Brain and Mind Centre, University of Sydney and Adam Guastella, Professor and Clinical Psychologist, Michael Crouch Chair in Child and Youth Mental Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
How can I get water out of my ear after swimming?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Swimming is one of the best parts of summer. But long after you’ve cooled down and dried off, you might be left with a niggling feeling – there is still water in your ear.
Your ear may feel full or blocked and sounds may be muffled. You may even hear some gurgling or rustling noises.
While water usually drains naturally, a few tips can help speed things up and prevent swimmer’s ear, a common infection after swimming.

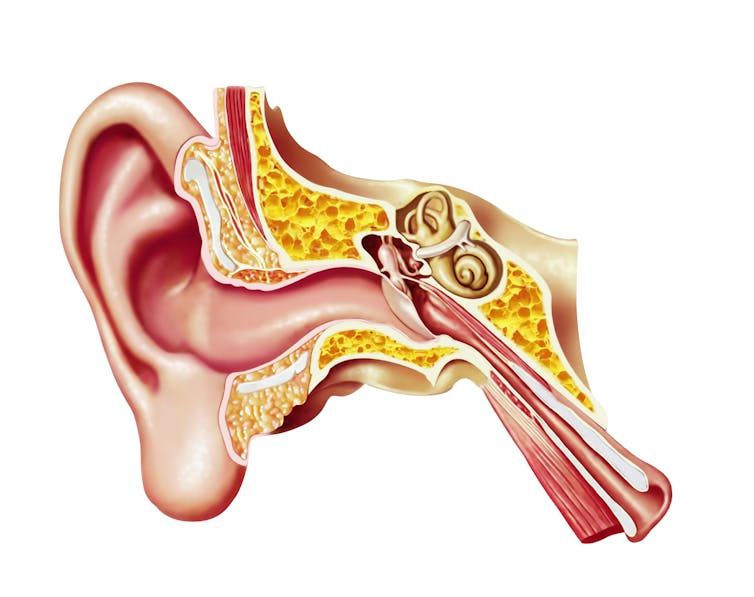
Rhett Noonan/Unsplash Why water gets stuck
You might think your ear canal is a straight tube, but it’s not. It bends twice, and some people’s canals are naturally narrower than others.
The ear canal is lined with hair and wax for protection. It can also develop extra bone growth (exostoses) from years of cold-water swimming, sometimes known as “surfer’s ear”, which can make it even narrower.
When you swim, water can easily get past all these curves and barriers when you dip your head under water or get splashed. But getting it out afterwards can be tricky.
The ear canal bends twice and is naturally narrower in some people. Leonello Calvetti/Stocktreck Images/Getty Try the simplest things first
Wiggle and tilt
Gently tug your earlobe up and down while tipping the blocked ear towards your shoulder. This straightens the ear canal and lets gravity help drain water out.
Lie on your side
Lay on your side on a towel for a few minutes, then roll over to the other side. Gravity will help again. In summer, warmth from the sun and towel can also help water in the ear dry faster.
Cup and pump
Press your slightly cupped palm over your ear to form a seal, then gently push and release to create a vacuum effect. You can also press the tragus (the firm skin in front of your ear canal) over the opening of your ear canal several times to encourage movement and drainage.
The tragus is the small cartilage flap covering the ear canal’s opening. Kindel Media/Pexels Do I need ear drops?
If none of these tips have worked so far, you might need some ear drops designed to dry out your ears.
Typically, these contain alcohol, which helps water evaporate faster. You can get these over the counter from a pharmacy.
But be sure to read the instructions, and don’t use them if you have any ear pain, discharge, an ear infection or a hole in your eardrum (or grommets, which are tiny tubes surgically inserted in the eardrum).
Some people make their own drops, using a solution of rubbing alcohol and white vinegar in equal proportions. This makes the ear canal more acidic, which can help prevent bacteria and fungal growth.
Be cautious when you use your own drops (again, don’t use them if you think you have a hole in your eardrum) and only use a few drops in each ear.
What not to do
Never put anything in your ears – even fingers or the tip of a towel can push water, wax and anything else trapped in your ear deeper and worsen the problem.
You might also scratch the delicate canal skin, increasing infection risk.
Avoid cotton buds and stick to the tips above.
Is trapped water dangerous?
Many people find the feeling annoying. But warm, moist places are also ideal for bacteria and fungi, so water trapped in the ear canal can lead to swimmer’s ear (otitis externa).
Symptoms include pain when moving the outer ear (the bit you can see), itchiness, discharge, redness or swelling, and sometimes fever.
Around one in ten people experience it at some point in their lives, most often during summer, and kids aged 7–14 are at higher risk.
If you suspect you have swimmer’s ear, it is important to see a medical professional as you will likely need treatment (typically antibiotic drops and pain relief).
Avoid swimming after storms or in polluted water, which carries more bacteria.
Freshwater sources such as rivers and lakes pose greater risk than salty ocean water, while properly chlorinated pools are generally pretty safe.
How to avoid it and when to seek help
If you don’t like the feeling after swimming – or you frequently get water trapped in your ears – invest in a swim cap or some ear plugs. Audiologists can help you find or customise earplugs to fit your ears.
Prioritise drying out ears once you are finished swimming, and use some of the tips above. For kids, making it into a game can help.
If an ear feels painful, inflamed or looks swollen, there might be an ear infection and it’s best to seek advice and attention from your GP.
If you still feel like you have water in your ears after two to three days, it’s best to also get it checked out.
Peter Carew, Senior Lecturer in Audiology, The University of Melbourne; Murdoch Children’s Research Institute
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Disordered Mind – by Dr. Eric Kandel
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We don’t generally include author bios in these reviews, but it’s worth mentioning that Dr. Kandel won the Nobel Prize in Physiology/Medicine, for studies related to the topics in this book.
The premise in this book is as per the subtitle: what unusual brains tell us about ourselves. He assumes that the reader has a “usual” brain, but if you don’t, then all is not lost, and in fact he probably talks about your brain in the book too.
Examining the brains of people with conditions ranging from autism to Alzheimer’s, schizophrenia to Parkinson’s, or even such common things as depression and anxiety and addiction, tells us a lot about what in our brain (anatomically and physiologically) is responsible for what, and how those things can be thrown out of balance.
By inference, that also tells us how to keep things from being thrown out of balance. Even if the genetic deck is stacked against you, there are still things that can be done to avoid actual disease. After all, famously, “genes load the gun, but lifestyle pulls the trigger”.
Dr. Kandel writes in a clear and lucid fashion, such that even the lay reader can quite comfortably learn about such things as prion-folding and inhibitory neurons and repressed transcription factors and more.
Bottom line: if you’d like to understand more about what goes wrong and how and why and what it means for your so-far-so-good healthy brain, this is the book for that.
Click here to check out The Disordered Mind, and understand more!
Share This Post




Related Posts
-

Best Salt for Neti Pots?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
❓ Q&A With 10almonds Subscribers!
Q: What kind of salt is best for neti pots?
A: Non-iodised salt is usually recommended, but really, any human-safe salt is fine. By this we mean for example:
- Sodium chloride (like most kitchen salts),
- Potassium chloride (as found in “reduced sodium” kitchen salts), or
- Magnesium sulfate (also known as epsom salts).
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What’s the difference between osteoarthritis and rheumatoid arthritis?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Arthritis – an umbrella term for around 100 conditions that damage the joints – affects 4.1 million Australians. This is expected to rise by 31% to 5.4 million by 2040 and cost the Australian health-care system an estimated $12 billion each year.
The two most common types, osteoarthritis and rheumatoid arthritis, can both cause joint pain, swelling and stiffness. Both are more common in women. Neither can be cured.
But their causes, risk factors and treatments are different – here’s what you need to know.
Douglas Olivares/Shutterstock. What is osteoarthritis?
Osteoarthritis is the most common form of arthritis. It affects 2.1 million Australians, mostly older people. About a third of Australians aged 75 and older have the condition.
It can affect any joint but is most common in the knees, hips, fingers, thumbs and big toes.
The main symptom is pain, especially during movement. Other symptoms may include swelling, stiffness and changes to the shape of joints.
The main risk factors are ageing and obesity, as well as previous injuries or surgery. For osteoarthritis in the hands, genetics also play a big role.
Signs of osteoarthritis can appear on knee scans from around age 45 and become more common with age.
However, this type of arthritis not simply the “wear and tear” of ageing. Osteoarthritis is a complex disease that affects the whole joint. This includes the cartilage (“shock-absorbing” connective tissue protecting your bones), bones, ligaments (connective tissue holding bones and body parts in place) and joint lining.
Osteoarthritis can change the shape of joints such as knuckles. joel bubble ben/Shutterstock How is it diagnosed?
Diagnosis is based on symptoms (such as pain and restricted movement) and a physical exam.
The disease generally worsens over time and cannot be reversed. But the severity of damage does not always correlate with pain levels.
For this reason, x-rays and MRI scans are usually unhelpful. Some people with early osteoarthritis experience severe pain, but the damage won’t show up on a scan. Others with advanced and visible osteoarthritis may have few symptoms or none at all.
What about rheumatoid arthritis?
Unlike osteoarthritis, rheumatoid arthritis is an autoimmune disease. This means the immune system attacks the joint lining, causing inflammation and damage.
Common symptoms include pain, joint swelling and stiffness, especially in the morning.
Rheumatoid arthritis is less common than osteoarthritis, affecting around 514,000 Australians. It mostly impacts the wrists and small joints in the hands and feet, though larger joints such as the elbows, shoulders, knees and ankles can also be involved.
It can also affect other organs, including the skin, lungs, eyes, heart and blood vessels. Fortunately, disease outside the joint has become less common in recent years, likely due to better and earlier treatment.
Rheumatoid arthritis often develops earlier than osteoarthritis but can occur at any age. Onset is most frequent in those aged 35–64. Smoking increases your risk.
How is it diagnosed?
As with osteoarthritis, your doctor will diagnose rheumatoid arthritis based on your symptoms and a physical exam.
Some other tests can be useful. Blood tests may pick up specific antibodies that indicate rheumatoid arthritis, although you can still have the condition with negative results.
X-rays may also reveal joint damage if the disease is advanced. If there is uncertainty, an ultrasound or MRI can help detect inflammation.
The Conversation, CC BY-SA How is osteoarthritis treated?
No treatment can stop osteoarthritis progressing. However many people manage their symptoms well with advice from their doctor and self-care. Exercise, weight management and pain medicines can help.
Exercise has been shown to be safe for osteoarthritis of the knee, hip and hand. Many types of exercise are effective at reducing pain, so you can choose what suits you best.
For knee osteoarthritis, managing weight through diet and/or exercise is strongly recommended. This may be because it reduces pressure on the joint or because losing weight can reduce inflammation. Anti-obesity medicines may also reduce pain.
Exercise can help manage weight and is safe and effective at managing joint pain. gelog67/Shutterstock Topical and oral anti-inflammatories are usually recommended to manage pain. However, opioids (such as tramadol or oxycodone) are not, due to their risks and limited evidence they help.
In some cases antidepressants such as duloxetine may also be considered as a treatment for pain though, again, evidence they help is limited.
What about rheumatoid arthritis?
Treatments for rheumatoid arthritis focus on preventing joint damage and reducing inflammation.
It’s essential to get an early referral to a rheumatologist, so that treatment with medication – called “disease-modifying anti-rheumatic drugs” – can begin quickly.
These medicines suppress the immune system to stop inflammation and prevent damage to the joint.
With no cure, the overall goal is to achieve remission (where the disease is inactive) or get symptoms under control.
Advances in treatment
There is an increasing interest in prevention for both types of arthritis.
A large international clinical trial is currently investigating whether a diet and exercise program can prevent knee osteoarthritis in those with higher risk – in this case, women who are overweight and obese.
For those already affected, new medicines in early-stage clinical trials show promise in reducing pain and improving function.
There is also hope for rheumatoid arthritis with Australian researchers developing a new immunotherapy. This treatment aims to reprogram the immune system, similar to a vaccine, to help people achieve long-term remission without lifelong treatment.
Giovanni E. Ferreira, NHMRC Emerging Leader Research Fellow, Institute of Musculoskeletal Health, University of Sydney and Rachelle Buchbinder, Professor of Clinical Epidemiology and Rheumatologist, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
In Vermont, Where Almost Everyone Has Insurance, Many Can’t Find or Afford Care
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
RICHMOND, Vt. — On a warm autumn morning, Roger Brown walked through a grove of towering trees whose sap fuels his maple syrup business. He was checking for damage after recent flooding. But these days, his workers’ health worries him more than his trees’.
The cost of Slopeside Syrup’s employee health insurance premiums spiked 24% this year. Next year it will rise 14%.
The jumps mean less money to pay workers, and expensive insurance coverage that doesn’t ensure employees can get care, Brown said. “Vermont is seen as the most progressive state, so how is health care here so screwed up?”
Vermont consistently ranks among the healthiest states, and its unemployment and uninsured rates are among the lowest. Yet Vermonters pay the highest prices nationwide for individual health coverage, and state reports show its providers and insurers are in financial trouble. Nine of the state’s 14 hospitals are losing money, and the state’s largest insurer is struggling to remain solvent. Long waits for care have become increasingly common, according to state reports and interviews with residents and industry officials.
Rising health costs are a problem across the country, but Vermont’s situation surprises health experts because virtually all its residents have insurance and the state regulates care and coverage prices.
For more than 15 years, federal and state policymakers have focused on increasing the number of people insured, which they expected would shore up hospital finances and make care more available and affordable.
“Vermont’s struggles are a wake-up call that insurance is only one piece of the puzzle to ensuring access to care,” said Keith Mueller, a rural health expert at the University of Iowa.
Regulators and consultants say the state’s small, aging population of about 650,000 makes spreading insurance risk difficult. That demographic challenge is compounded by geography, as many Vermonters live in rural areas, where it’s difficult to attract more health workers to address shortages.
At least part of the cost spike can be attributed to patients crossing state lines for quicker care in New York and Massachusetts. Those visits can be more expensive for both insurers and patients because of long ambulance rides and charges from out-of-network providers.
Patients who stay, like Lynne Drevik, face long waits. Drevik said her doctor told her in April that she needed knee replacement surgeries — but the earliest appointment would be in January for one knee and the following April for the other.
Drevik, 59, said it hurts to climb the stairs in the 19th-century farmhouse in Montgomery Center she and her husband operate as an inn and a spa. “My life is on hold here, and it’s hard to make any plans,” she said. “It’s terrible.”
Health experts say some of the state’s health system troubles are self-inflicted.
Unlike most states, Vermont regulates hospital and insurance prices through an independent agency, the Green Mountain Care Board. Until recently, the board typically approved whatever price changes companies wanted, said Julie Wasserman, a health consultant in Vermont.
The board allowed one health system — the University of Vermont Health Network — to control about two-thirds of the state’s hospital market and allowed its main facility, the University of Vermont Medical Center in Burlington, to raise its prices until it ranked among the nation’s most expensive, she said, citing data the board presented in September.
Hospital officials contend their prices are no higher than industry averages.
But for 2025, the board required the University of Vermont Medical Center to cut the prices it bills private insurers by 1%.
The nonprofit system says it is navigating its own challenges. Top officials say a severe lack of housing makes it hard to recruit workers, while too few mental health providers, nursing homes, and long-term care services often create delays in discharging patients, adding to costs.
Two-thirds of the system’s patients are covered by Medicare or Medicaid, said CEO Sunny Eappen. Both government programs pay providers lower rates than private insurance, which Eappen said makes it difficult to afford rising prices for drugs, medical devices, and labor.
Officials at the University of Vermont Medical Center point to several ways they are trying to adapt. They cited, for example, $9 million the hospital system has contributed to the construction of two large apartment buildings to house new workers, at a subsidized price for lower-income employees.
The hospital also has worked with community partners to open a mental health urgent care center, providing an alternative to the emergency room.
In the ER, curtains separate areas in the hallway where patients can lie on beds or gurneys for hours waiting for a room. The hospital also uses what was a storage closet as an overflow room to provide care.
“It’s good to get patients into a hallway, as it’s better than a chair,” said Mariah McNamara, an ER doctor and associate chief medical officer with the hospital.
For the about 250 days a year when the hospital is full, doctors face pressure to discharge patients without the ideal home or community care setup, she said. “We have to go in the direction of letting you go home without patient services and giving that a try, because otherwise the hospital is going to be full of people, and that includes people that don’t need to be here,” McNamara said.
Searching for solutions, the Green Mountain Care Board hired a consultant who recommended a number of changes, including converting four rural hospitals into outpatient facilities, in a worst-case scenario, and consolidating specialty services at several others.
The consultant, Bruce Hamory, said in a call with reporters that his report provides a road map for Vermont, where “the health care system is no match for demographic, workforce, and housing challenges.”
But he cautioned that any fix would require sacrifice from everyone, including patients, employers, and health providers. “There is no simple single policy solution,” he said.
One place Hamory recommended converting to an outpatient center only was North Country Hospital in Newport, a village in Vermont’s least populated region, known as the Northeast Kingdom.
The 25-bed hospital has lost money for years, partly because of an electronic health record system that has made it difficult to bill patients. But the hospital also has struggled to attract providers and make enough money to pay them.
Officials said they would fight any plans to close the hospital, which recently dropped several specialty services, including pulmonology, neurology, urology, and orthopedics. It doesn’t have the cash to upgrade patient rooms to include bathroom doors wide enough for wheelchairs.
On a recent morning, CEO Tom Frank walked the halls of his hospital. The facility was quiet, with just 14 admitted patients and only a couple of people in the ER. “This place used to be bustling,” he said of the former pulmonology clinic.
Frank said the hospital breaks even treating Medicare patients, loses money treating Medicaid patients, and makes money from a dwindling number of privately insured patients.
The state’s strict regulations have earned it an antihousing, antibusiness reputation, he said. “The cost of health care is a symptom of a larger problem.”
About 30 miles south of Newport, Andy Kehler often worries about the cost of providing health insurance to the 85 workers at Jasper Hill Farm, the cheesemaking business he co-owns.
“It’s an issue every year for us, and it looks like there is no end in sight,” he said.
Jasper Hill pays half the cost of its workers’ health insurance premiums because that’s all it can afford, Kehler said. Employees pay $1,700 a month for a family, with a $5,000 deductible.
“The coverage we provide is inadequate for what you pay,” he said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:






