The Art Of Letting Go – by Nick Trenton
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may be wondering: is this a basic CBT book? And, for the most part, no, it’s not.
It does touch on some of the time-tested CBT techniques, but a large part of the book is about reframing things in a different way, that’s a little more DBT-ish, and even straying into BA. But enough of the initialisms, let’s give an example:
It can be scary to let go of the past, or of present or future possibilities (bad ones as well as good!). However, it’s hard to consciously do something negative (same principle as “don’t think of a pink elephant”), so instead, look at it as taking hold of the present/future—and thus finding comfort and security in a new reality rather than an old memory or a never-actual imagining.
So, this book has a lot of ideas like that, and if even one of them helps, then it was worth reading.
The writing style is comprehensive, and goes for the “tell them what you’re gonna tell them; tell them; then tell them what you told them” approach, which a) is considered good for learning b) can feel a little like padding nonetheless.
Bottom line: this reviewer didn’t personally love the style, but the content made up for it.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Body Scrubs: Benefits, Risks, and Guidance

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I was wondering whether I should be using a body scrub in the shower, rather than just soap. What should guide me in the choice of a body scrub, and are there any risks to be aware of?❞
Body scrubs are great for giving skin a healthy glow, but are best used sparingly—over-exfoliation leads to the opposite effect (unhappy skin, premature skin aging, etc).
As for contents:
- microplastics are now banned in most places, but you might want to check any products (and their containers!) are BPA-free, pthalate free, etc.
- fragrances in body scrubs are usually a bad idea, and many essential oils have been shown to be endocrine-disruptors, which you do not want:
About the microplastics, harmful artificial chemicals in general, and what constitutes “etc”:
About the fragrances’ (including “natural” essential oils’) endocrine-disrupting shenanigans:
Endocrine-disrupting chemicals: an Endocrine Society scientific statement
So, what might you want to use instead?
If you’re feeling adventurous, you might like to try treating yourself to a pineapple-based mask instead (a muslin cloth soaked in pineapple juice will work just fine; please don’t waterboard yourself though), as the bromelain enzymes (found very generously in pineapple juice) break down dead cells without the need for scrubbing.
Another option is a homemade salt- or sugar-scrub. Put your salt or sugar into a jar, add enough warm water to cover it, leave it for about a day, adding more water if it seems in danger of drying out, until it recrystallizes with a high water content keeping it malleable to the touch; congratulations, you now have a very simple scrub. This should still not be used more than, say, once per week, though.
Last but not least, you might consider investing in a konjac sponge; they gently remove dead skin without damaging living skin. Here’s an example product on Amazon, for your convenience
For more on gentle-yet-effective skincare, you might like to read:
Clean: The New Science of Skin and the Beauty of Doing Less
Enjoy!
Share This Post
-

Stay off My Operating Table – by Dr. Philip Ovadia
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
With heart disease as the #1 killer worldwide, and 88% of adults being metabolically unhealthy (leading cause of heart disease), this is serious!
Rather than taking a “quick fix” advise-and-go approach, Dr. Ovadia puts the knowledge and tools in our hands to do better in the long term.
As a heart surgeon himself, his motto here is:
❝What foods to put on your table so you don’t end up on mine❞
There’s a lot more to this book than the simple “eat the Mediterranean diet”:
- While the Mediterranean diet is generally considered the top choice for heart health, he also advises on how to eat healthily on all manner of diets… Carnivore, Keto, Paleo, Atkins, Gluten-Free, Vegan, you-name-it.
- A lot of the book is given to clearing up common misconceptions, things that sounded plausible but are just plain dangerous. This information alone is worth the price of the book, we think.
- There’s also a section given over to explaining the markers of metabolic health, so you can monitor yourself effectively
- Rather than one-size-fits-all, he also talks about common health conditions and medications that may change what you need to be doing
- He also offers advice about navigating the health system to get what you need—including dealing with unhelpful doctors!
Bottom line: A very comprehensive (yet readable!) manual of heart health.
Get your copy of Stay Off My Operating Table from Amazon today!
Share This Post
-

International Day of Women and Girls in Science
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Today is the International Day of Women and Girls in Science, so we’ve got a bunch of content for the ladies out there. Let’s start with the statement Sima Bahous (the Executive Director of UN Women) made:
❝This year, the sixty-seventh session of the Commission on the Status of Women (CSW67) will consider as its priority theme “Innovation and technological change, and education in the digital age for achieving gender equality and the empowerment of all women and girls”.
This is an unprecedented opportunity for the Commission to develop a definitive agenda for progress towards women’s full and equal participation and representation in STEM. Its implementation will require bold, coordinated, multi-stakeholder action.❞
Here at 10almonds, we are just one newsletter, and maybe we can’t change the world (…yet), but we’re all for this!
We’re certainly all in favour of education in the digital age, and more of our subscribers are women and girls than not (highest of fives from your writer today, also a woman—and I do bring most of the sciency content).
Medical News Today asks “Why Are Women Less Likely To Survive Cardiac Arrest Than Men?”
You can read the full article here, but the short version is:
- People (bystanders and EMS professionals alike!) are less likely to intervene to give CPR when the patient is a woman (we appreciate that “your hands on an unknown woman’s chest” is a social taboo, but there’s a time and a place!)
- People trained to give CPR (volunteers or professionals!) are often less confident about how to do so with female anatomy—training is almost entirely on “male” dummies.
A quick take-away from this is: to give effective CPR, you need to be giving two-inch compressions!
On a side note, do you want to learn how to correctly do chest compressions on female anatomy? This short (1:55) video could save a woman’s life!
As a science-based health and productivity newsletter, we make no apologies if occasional issues sometimes have a slant to women’s health! Heaven help us, the bias in science at large is certainly the opposite:
The list of examples is far too long for us to include here, but two that spring immediately to mind are:
- PCOS (Polycystic ovary syndrome), which affects nearly 1 in 5 women, can lead to infertility, never mind the inconvenience of irregular bleeding, chronic pain, and diabetes (amongst other things), and… nobody knows what causes it, or what to do about it.
- Endometriosis (the lining of the womb starts growing in other places), meanwhile, affects around 1 in 10 women. It causes chronic pain and fatigue, and again, nobody knows what causes it or how to cure it.
Maybe if women in STEM weren’t on the receiving end of rampant systemic misogyny, we’d have more women in science, and some answers by now!
❗️NOT-SO-FUN FACT:
Women make up only 28% of the workforce in science, technology, engineering and math (STEM), and men vastly outnumber women majoring in most STEM fields in college. The gender gaps are particularly high in some of the fastest-growing and highest-paid jobs of the future, like computer science and engineering.
Source: AAUW
The US census suggests change is happening, but is a very long way from equality!
WHAT OUR SUBSCRIBERS SAY:
❝Women are slowly gaining more of a place in academia, and slowly making more of a difference when they get there, and start doing research that reflects ourselves. But I still think that it’s a struggle to get there, and it’s a struggle to be heard and be respected.
It’s a matter of pride, it’s a matter of proving yourself, being in STEM, and [women in STEM] still report being extremely disrespected, not taken seriously all, despite being very very good.
It’s worth noting as well, that we’ve had women in STEM for a while and there are so many things we appreciate nowadays that they were a part of, but they were never given credit for—it’s still a problem today and something we need to more actively fight.❞
Isabella F. Lima, Occupational Psychologist
Are you a woman in STEM, and have a story to tell? We’d love to hear it! Just reply to this email 🙂
Share This Post

Related Posts
-

South Indian-Style Chickpea & Mango Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We have a double-dose of chickpeas today, but with all the other ingredients, this dish is anything but boring. Fun fact about chickpeas though: they’re rich in sitosterol, a plant sterol that, true to its name, sits on cholesterol absorption sites, reducing the amount of dietary cholesterol absorbed. If you are vegan, this will make no difference to you because your diet does not contain cholesterol, but for everyone else, this is a nice extra bonus!
You will need
- 1 can white chickpeas, drained and rinsed
- 1 can black chickpeas (kala chana), drained and rinsed
- 9 oz fresh mango, diced (or canned is fine if that’s what’s available)
- 1½ oz ginger, peeled and grated
- 2 green chilis, finely chopped (adjust per heat preferences)
- 2 tbsp desiccated coconut (or 3 oz grated coconut, if you have it fresh)
- 8 curry leaves (dried is fine if that’s what’s available)
- 1 tsp mustard seeds
- 1 tsp cumin seeds
- 1 tsp black pepper, coarse ground
- ½ tsp MSG or 1 tsp low-sodium salt
- Juice of 1 lime
- Extra virgin olive oil
Method
(we suggest you read everything at least once before doing anything)
1) Heat some oil in a skillet over a medium heat. When it’s hot but not smoking, add the ginger, chilis, curry leaves, mustard seeds, and cumin seeds, stirring well to combine, keep going until the mustard seeds start popping.
2) Add the chickpeas (both kinds), as well as the black pepper and the MSG/salt. Once they’re warm through, take it off the heat.
3) Add the mango, coconut, and lime juice, mixing thoroughly.
4) Serve warm, at room temperature, or cold:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- What Matters Most For Your Heart?
- Can Saturated Fats Be Healthy?
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Antidepressants: Personalization Is Key!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Antidepressants: Personalization Is Key!

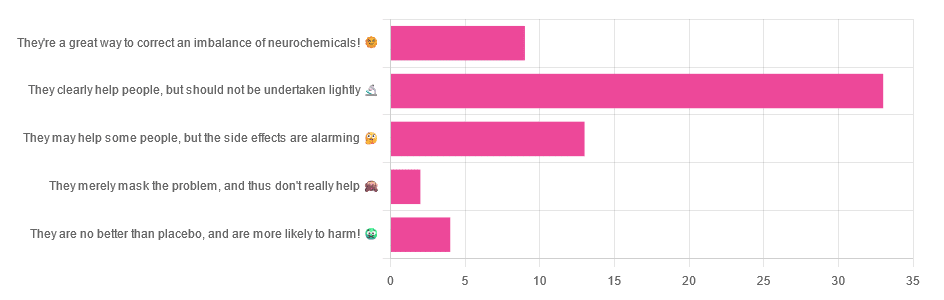
Yesterday, we asked you for your opinions on antidepressants, and got the above-depicted, below-described, set of responses:
- Just over half of respondents said “They clearly help people, but should not be undertaken lightly”
- Just over a fifth of respondents said “They may help some people, but the side effects are alarming”
- Just under a sixth of respondents said “They’re a great way to correct an imbalance of neurochemicals”
- Four respondents said “They are no better than placebo, and are more likely to harm”
- Two respondents said “They merely mask the problem, and thus don’t really help”
So what does the science say?
❝They are no better than placebo, and are more likely to harm? True or False?❞
True or False depending on who you are and what you’re taking. Different antidepressants can work on many different systems with different mechanisms of action. This means if and only if you’re not taking the “right” antidepressant for you, then yes, you will get only placebo benefits:
- Placebo Effect in the Treatment of Depression and Anxiety ← randomly assigned antidepressants are, shockingly, luck of the draw in usefulness
- Antidepressants versus placebo in major depression: an overview ← “wow this science is messy”
- Comparative efficacy and acceptability of 21 antidepressant drugs: a systematic review and network meta-analysis ← “oh look, it makes a difference which antidepressant we give to people”
Rather than dismissing antidepressants as worthless, therefore, it is a good idea to find out (by examination or trial and error) what kind of antidepressant you need, if you indeed do need such.
Otherwise it is like getting a flu shot and being surprised when you still catch a cold!
❝They merely mask the problem, and thus don’t really help: True or False?❞
False, categorically.
The problem in depressed people is the depressed mood. This may be influenced by other factors, and antidepressants indeed won’t help directly with those, but they can enable the person to better tackle them (more on this later).
❝They may help some people, but the side-effects are alarming: True or False?❞
True or False depending on more factors than we can cover here.
Side-effects vary from drug to drug and person to person, of course. As does tolerability and acceptability, since to some extent these things are subjective.
One person’s dealbreaker may be another person’s shrugworthy minor inconvenience at most.
❝They’re a great way to correct an imbalance of neurochemicals: True or False?❞
True! Contingently.
That is to say: they’re a great way to correct an imbalance of neurochemicals if and only if your problem is (at least partly) an imbalance of neurochemicals. If it’s not, then your brain can have all the neurotransmitters it needs, and you will still be depressed, because (for example) the other factors* influencing your depression have not changed.
*common examples include low self-esteem, poor physical health, socioeconomic adversity, and ostensibly bleak prospects for the future.
For those for whom the problem is/was partly a neurochemical imbalance and partly other factors, the greatest help the antidepressants give is getting the brain into sufficient working order to be able to tackle those other factors.
Want to know more about the different kinds?
Here’s a helpful side-by-side comparison of common antidepressants, what type they are, and other considerations:
Mind | Comparing Antidepressants
Want a drug-free approach?
You might like our previous main feature:
The Mental Health First-Aid That You’ll Hopefully Never Need
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Age & Aging: What Can (And Can’t) We Do About It?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How old do you want to be?

We asked you how old you are, and got an interesting spread of answers. This wasn’t too surprising; of course we have a general idea of who our readership is and we write accordingly.
What’s interesting is the gap for “40s”.
And, this wasn’t the case of a broken poll button, it’s something that crops up a lot in health-related sociological research. People who are most interested in taking extra care of their body are often:
- Younger people full of optimism about maintaining this perfectly healthy body forever
- Older people realizing “if I don’t want to suffer avoidable parts of age-related decline, now is the time to address these things”
In between, we often have a gap whereby people no longer have the optimism of youth, but do not yet feel the pressure of older age.
Which is not to say there aren’t 40-somethings who do care! Indeed, we know for a fact we have some subscribers in their 40s (and some in their 90s, too), just, they evidently didn’t vote in this poll.
Anyway, let’s bust some myths…
Aging is inevitable: True or False?
False, probably. That seems like a bold (and fortune-telling) claim, so let’s flip it to deconstruct it more logically:
Aging is, and always will be, unstoppable: True or False?
That has to be “False, probably”. To say “true” now sounds like an even bolder claim. Just like “the moon will always be out of reach”.
- When CPR was first developed, first-aiders were arrested for “interfering with a corpse”.
- Many diseases used to be death sentences that are now “take one of these in the morning”
- If you think this is an appeal to distant history, HIV+ status was a death sentence in the 90s. Now it’s “take one of these in the morning”.
But, this is an appeal to the past, and that’s not always a guarantee of the future. Where does the science stand currently? How is the research and development doing on slowing, halting, reversing aging?
We can slow aging: True or False?
True! There’s a difference between chronological age (i.e., how much time has passed while we’ve been alive) and biological age (i.e., what our diverse markers of aging look like).
Biological age often gets talked about as a simplified number, but it’s more complex than that, as we can age in different ways at different rates, for example:
- Visual markers of aging (e.g. wrinkles, graying hair)
- Performative markers of aging (e.g. mobility tests)
- Internal functional markers of aging (e.g. tests for cognitive decline, eyesight, hearing, etc)
- Cellular markers or aging (e.g. telomere length)
- …and more, but we only have so much room here
There are things we can do to slow most of those, including:
- Good nutrition (e.g. collagen and lutein, to keep specific parts of the body functioning “like those of a younger person” ranging from the joints to the eyes and brain)
- Anti-oxidant activity (e.g. eating anti-oxidant foods, supplementing with anti-oxidants or other things that mitigate oxidative stress, and avoiding foods that hasten oxidative stress which causes many kinds of aging)
- Getting good sleep (not to be underestimated for its restorative importance)
- Taking care of our cognitive health
- Taking care of our mental health (especially: reducing stress)
- Taking care of our mobility (prevention is better than cure!)
In the case of cognitive decline particularly, check out our previous article:
How To Reduce Your Alzheimer’s Risk
It’s too early to worry about… / It’s too late to do anything about… True or False?
False and False!
Many things that affect our health later in life are based on early-life choices and events. So it’s important for young people to take advantage of that. The earlier one adopts a healthy lifestyle, the better, because, and hold onto your hats for the shocker here: aging is cumulative.
However, that doesn’t mean that taking up healthy practices (or dropping unhealthy ones) is pointless later in life, even in one’s 70s and beyond!
Read about this and more from the National Institute of Aging:
What Do We Know About Healthy Aging?
We can halt aging: True or False?
False, for now at least. Our bodies are not statues; they are living organisms, constantly rebuilding themselves, constantly changing, every second of every day, for better or for worse. Every healthy or unhealthy choice you make, every beneficial or adverse experience you encounter, affects your body on a cellular level.
Your body never, ever, stops changing for as long as you live.
But…
We can reverse aging: True or False?
True! Contingently and with limitations, for now at least.
Remember what we said about your body constantly rebuilding itself? That goes for making itself better as well as making itself worse.
- If yesterday you couldn’t touch your toes and today you can, congratulations, you just got younger by a biological marker of aging.
- If you stopped drinking/smoking/eating a certain way last year, and this year your skin has fewer wrinkles, congratulations, you got younger by a biological marker of aging.
- If you’ve been exercising and now your heart rate variability and VO2 max are better than last month, congratulations, you got younger by a biological marker aging.
- If you took supplements that reduce and/or mitigate oxidative stress (e.g. resveratrol, CoQ10, l-theanine, etc), and you took up intermittent fasting, and now your telomeres are longer than they were six months ago, congratulations, you got younger by a biological marker of aging.
But those aren’t really being younger, we’ll still die when our time is up: True or False?
False and True, respectively.
Those kinds of things are really being younger, biologically. What else do you think being biologically younger is?
We may indeed die when our time is up, but (unless we suffer fatal accident or incident first) “when our time is up” is something that is decided mostly by the above factors.
Genetics—the closest thing we have to biological “fate”—accounts for only about 25% of our longevity-related health*.
Genes predispose, but they don’t predetermine.
*Read more: Human longevity: Genetics or Lifestyle? It takes two to tango
(from the Journal of Immunity and Ageing)
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: