Our Top 5 Spices: How Much Is Enough For Benefits?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A spoonful of pepper makes the… Hang on, no, that’s not right…
We know that spices are the spice of life, and many have great health-giving qualities. But…
- How much is the right amount?
- What’s the minimum to get health benefits?
- What’s the maximum to avoid toxicity?
That last one always seems like a scary question, but please bear in mind: everything is toxic at a certain dose. Oxygen, water, you-name-it.
On the other hand, many things have a toxicity so low that one could not physically consume it sufficiently faster than the body eliminates it, to get a toxic build-up.
Consider, for example, the €50 banknote that was nearly withdrawn from circulation because one of the dyes used in it was found to be toxic. However, the note remained in circulation after scientists patiently explained that a person would have to eat many thousands of them to get a lethal dose.
So, let’s address these questions in reverse order:
What’s the maximum to avoid toxicity?
In the case of the spices we’ll look at today, the human body generally* has high tolerance for them if eaten at levels that we find comfortable eating.
*IMPORTANT NOTE: If you have (or may have) a medical condition that may be triggered by spices, go easier on them (or if appropriate, abstain completely) after you learn about that.
Check with your own physician if unsure, because not only are we not doctors, we’re specifically not your doctors, and cannot offer personalized health advice.
We’re going to be talking in averages and generalizations here. Caveat consumator.
For most people, unless you are taking the spice in such quantities that you are folding space and seeing the future, or eating them as the main constituents of your meal rather than an embellishment, you should be fine. Please don’t enter a chilli-eating contest and sue us.
What is the minimum to get health benefits and how much should we eat?
The science of physiology generally involves continuous rather than discrete data, so there’s not so much a hard threshold, as a point at which the benefits become significant. The usefulness of most nutrients we consume, be they macro- or micro-, will tend to have a bell curve.
In other words, a tiny amount won’t do much, the right amount will have a good result, and usefulness will tail off after that point. To that end, we’re going to look at the “sweet spot” of peaking on the graph.
Also note: the clinical dose is the dose of the compound, not the amount of the food that one will need to eat to get that dose. For example, food x containing compound y will not usually contain that compound at 100% rate and nothing else. We mention this so that you’re not surprised when we say “the recommended dose is 5mg of compound, so take a teaspoon of this spice”, for example.
Further note: we only have so much room here, so we’re going to list only the top benefits, and not delve into the science of them. You can see the related main features for more details, though!
The “big 5” health-giving spices, with their relevant active compound:
- Black pepper (piperine)
- Hot pepper* (capsaicin)
- Garlic (allicin)
- Ginger (gingerol)
- Turmeric (curcumin**)
*Cayenne pepper is very high in capsaicin; chilli peppers are also great
**not the same thing as cumin, which is a completely different plant. Cumin does have some health benefits of its own, but not in the same league as the spices above, and there’s only so much we have room to cover today.
Black pepper
- Benefits: antioxidant, anti-cancer, boosts bioavailability of other nutrients, aids digestion
- Dosage: 5–20mg for benefits
- Suggestion: ½ teaspoon of black pepper is sufficient for benefits. However, this writer’s kitchen dictum in this case is “if you can’t see the black pepper in/on the food, add more”—but that’s more about taste!
- Related main feature: Black Pepper’s Anti-Cancer Arsenal (And More)
Hot Pepper
- Benefits: anti-inflammatory, metabolism accelerator
- Dosage: 6mg gives benefits, 500mg is a common dose in capsules
- Suggestion: if not making a spicy dish, consider using a teaspoon of cayenne as part of the seasoning for rice or potatoes
- Related main feature: Capsaicin For Weight Loss And Against Inflammation
Garlic
- Benefits: heart health, blood sugar balancing, anti-cancer
- Dosage: 4–8µg for benefits
- Suggestion: 1–2 cloves daily is generally good. However, cooking reduces allicin content (and so does oxidation after cutting/crushing), so you may want to adjust accordingly if doing those things.
- Related main feature: The Many Health Benefits Of Garlic
Ginger
- Benefits: anti-inflammatory, antioxidant, anti-nausea
- Dosage: 3–4g for benefits
- Suggestion: 1 teaspoon grated raw ginger or ½ a teaspoon powdered ginger, can be used in baking or as part of the seasoning for a stir-fry
- Related main feature: Ginger Does A Lot More Than You Think
Turmeric
- Benefits: anti-inflammatory, anti-cancer
- Dosage: 500–2000mg for benefits
- Suggestion: ¼ teaspoon per day is sufficient for benefits; ½ teaspoon dropped into the water when cooking rice will infuse the rice with turmeric (which is very water-soluble), turn the rice a pretty golden color, and not affect the flavor. Throw in some black pepper as it increases the bioavailability of curcumin up to 2000%
- Related main feature: Why Curcumin (Turmeric) Is Worth Its Weight In Gold
Closing notes
The above five spices are very healthful for most people. Personal physiology can and will vary, so if in doubt, a) check with your doctor b) start at lowest doses and establish your tolerance (or lack thereof).
Enjoy, and stay well!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A new treatment for Huntington’s disease is genuinely promising – but here’s why we still need caution

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Imagine knowing in your 20s or 30s that you carry a gene which will cause your mind and body to slowly unravel. Huntington’s disease is inherited, relentless and fatal, and there is no cure. Families live with the certainty of decline stretching across generations.
Now, a new treatment is being widely reported as a breakthrough.
Last week, gene therapy company uniQure announced that a one-time brain infusion appeared to slow the disease in a small clinical study.
If confirmed, this would not only be a landmark for Huntington’s disease but potentially the first time a gene therapy has shown promise in any adult-onset neurodegenerative disorder.
But the results, which were announced in a press release, are early, unreviewed and based on external comparisons. So, while these findings offer families hope after decades of failure, we need to remain cautious.

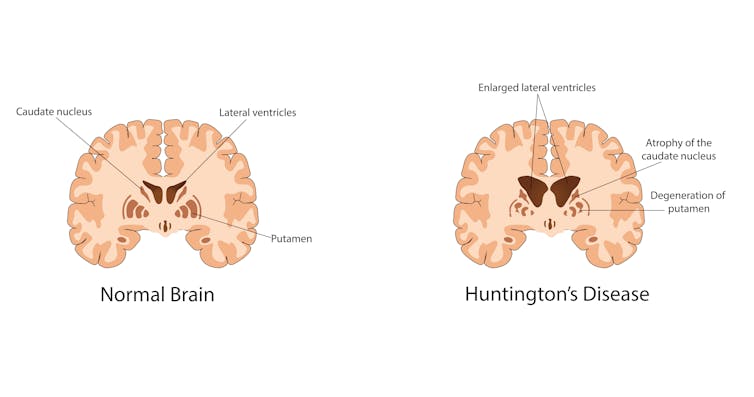
Krisada tepkulmanont/Getty What is Huntington’s disease?
Huntington’s is a rare but devastating disease, affecting around five to ten people in 100,000 in Western countries. That means thousands in Australia and hundreds of thousands worldwide.
Symptoms usually start in mid-life. They include involuntary movements, depression, irritability and progressive decline in thinking and memory. People lose the ability to work, manage money, live independently and eventually care for themselves. Most die ten to 20 years after onset.
The disease is caused by an expanded stretch of certain DNA repeats (CAG) in the huntingtin gene. The number of repeats strongly influences when symptoms begin, with longer expansions usually linked to earlier onset.
While rare, Huntington’s disease is inherited and fatal. Izuchukwu Onyeka/Getty Looking for a treatment
The gene that causes Huntington’s disease was identified in 1993, 32 years ago. Soon afterwards, mouse studies showed that switching off the mutant huntingtin protein even after symptoms had begun could reverse signs and improve behaviour.
This suggested lowering the toxic protein might slow or even partly reverse the disease. Yet for three decades, every attempt to develop a therapy for people has failed to show convincing clinical benefit. Trials of huntingtin-lowering drugs and other approaches did not slow progression.
What is the new treatment?
The one-time gene therapy, called AMT-130, involves brain surgery guided by MRI. Surgeons infuse an engineered virus directly into the caudate and putamen brain regions, which are heavily affected in Huntington’s.
The virus carries a short genetic “microRNA” designed to reduce production of the affected huntingtin protein.
By delivering it straight into the brain, the treatment bypasses the blood–brain barrier. This natural wall usually prevents medicines from entering the central nervous system. That barrier helps explain why so many brain-targeted drugs have failed.
What did they find?
Some 29 patients received treatment, with 12 in each group (one low-dose, and one high-dose) followed for three years. According to uniQure, those given the higher dose declined much slower than expected.
The study compared how much participants’ movement, thinking and daily function declined, compared to a matched external group from a global Huntington’s registry (meaning they weren’t part of the study). The company claimed those given the higher dose had a 75% slowing in their decline.
On a functional scale focused on independence, the company reported a 60% slowing in decline for the higher dose group.
Other tests of movement and thinking also favoured treatment. Nerve-cell damage in spinal fluid was lower for study participants than would be expected for untreated patients.
Why should we be cautious?
These findings are an early snapshot of results reported by the company, not yet peer-reviewed. The study compared treated patients to an external matched control group, not people randomised to placebo at the same time. This design can introduce bias. The numbers are also small – only 12 patients at the three-year mark – so we can’t draw solid conclusions.
The company reports the therapy was generally well tolerated, with no new serious adverse events related to the drug since late 2022. Most problems were related to the neurosurgical infusion itself, and resolved. But in a disease that already causes such severe symptoms, it is often hard to know what counts as a side effect.
The company uniQure has said it plans to seek regulatory approval in 2026 on the basis of this dataset.
Regulators will face difficult decisions: whether to allow access sooner before all the questions and uncertainties are addressed – based on the needs of a community with no effective options – and wait for further data while people are being treated, or to insist on larger trials that confirm results before approval.
What does it mean?
If upheld, these results represent the first convincing signs that a gene-targeted therapy can slow Huntington’s disease. They may also be the first evidence of benefit from a gene therapy in any adult-onset neurodegenerative disorder. That would be a milestone after decades of failure.
But these results do not prove success. Only larger, longer and fully peer-reviewed studies will show whether this treatment truly changes lives. Even if approved, a complex neurosurgical gene therapy may not be easily accessible to all patients.
The company has said the drug’s price would be similar to other gene therapies – which can cost over A$3 million per patient – and will have the added cost of brain surgery.
The takeaway
For families who carry this gene, the hope is profound. But caution is just as important.
We may be witnessing the first credible step toward slowing an inherited adult-onset neurodegenerative disease, or just an early signal that may not hold up.
Ultimately, only time and rigorous science will show whether this treatment delivers the benefits so urgently needed.
Bryce Vissel, Cojoint Professor, School of Clinical Medicine, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Dry Needling for Meralgia Paresthetica?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Could you address dry needling, who should administer it, and could it be a remedy for meralgia paresthetica? If not, could you speak to home-based remedies for meralgia paresthetica? Thank you?❞
We’ll need to take a main feature some time to answer this one fully, but we will say some quick things here:
- Dry needling, much like acupuncture, has been found to help with pain relief.
- Meralgia paresthetica, being a neuropathy, may benefit from some things that benefit people with peripheral neuropathy, such as lion’s mane mushroom. There is definitely not research to support this hypothesis yet though (so far as we could find anyway; there is plenty to support lion’s mane helping with nerve regeneration in general, but nothing specific for meralgia paresthetica).
Some previous articles you might enjoy meanwhile:
- Pinpointing The Usefulness Of Acupuncture
- Science-Based Alternative Pain Relief
- Peripheral Neuropathy: How To Avoid It, Manage It, Treat It
- What Does Lion’s Mane Actually Do, Anyway?
Take care!
Share This Post
-
Rapid Rise in Syphilis Hits Native Americans Hardest
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From her base in Gallup, New Mexico, Melissa Wyaco supervises about two dozen public health nurses who crisscross the sprawling Navajo Nation searching for patients who have tested positive for or been exposed to a disease once nearly eradicated in the U.S.: syphilis.
Infection rates in this region of the Southwest — the 27,000-square-mile reservation encompasses parts of Arizona, New Mexico, and Utah — are among the nation’s highest. And they’re far worse than anything Wyaco, who is from Zuni Pueblo (about 40 miles south of Gallup) and is the nurse consultant for the Navajo Area Indian Health Service, has seen in her 30-year nursing career.
Syphilis infections nationwide have climbed rapidly in recent years, reaching a 70-year high in 2022, according to the most recent data from the Centers for Disease Control and Prevention. That rise comes amid a shortage of penicillin, the most effective treatment. Simultaneously, congenital syphilis — syphilis passed from a pregnant person to a baby — has similarly spun out of control. Untreated, congenital syphilis can cause bone deformities, severe anemia, jaundice, meningitis, and even death. In 2022, the CDC recorded 231 stillbirths and 51 infant deaths caused by syphilis, out of 3,761 congenital syphilis cases reported that year.
And while infections have risen across the U.S., no demographic has been hit harder than Native Americans. The CDC data released in January shows that the rate of congenital syphilis among American Indians and Alaska Natives was triple the rate for African Americans and nearly 12 times the rate for white babies in 2022.
“This is a disease we thought we were going to eradicate not that long ago, because we have a treatment that works really well,” said Meghan Curry O’Connell, a member of the Cherokee Nation and chief public health officer at the Great Plains Tribal Leaders’ Health Board, who is based in South Dakota.
Instead, the rate of congenital syphilis infections among Native Americans (644.7 cases per 100,000 people in 2022) is now comparable to the rate for the entire U.S. population in 1941 (651.1) — before doctors began using penicillin to cure syphilis. (The rate fell to 6.6 nationally in 1983.)
O’Connell said that’s why the Great Plains Tribal Leaders’ Health Board and tribal leaders from North Dakota, South Dakota, Nebraska, and Iowa have asked federal Health and Human Services Secretary Xavier Becerra to declare a public health emergency in their states. A declaration would expand staffing, funding, and access to contact tracing data across their region.
“Syphilis is deadly to babies. It’s highly infectious, and it causes very severe outcomes,” O’Connell said. “We need to have people doing boots-on-the-ground work” right now.
In 2022, New Mexico reported the highest rate of congenital syphilis among states. Primary and secondary syphilis infections, which are not passed to infants, were highest in South Dakota, which had the second-highest rate of congenital syphilis in 2022. In 2021, the most recent year for which demographic data is available, South Dakota had the second-worst rate nationwide (after the District of Columbia) — and numbers were highest among the state’s large Native population.
In an October news release, the New Mexico Department of Health noted that the state had “reported a 660% increase in cases of congenital syphilis over the past five years.” A year earlier, in 2017, New Mexico reported only one case — but by 2020, that number had risen to 43, then to 76 in 2022.
Starting in 2020, the covid-19 pandemic made things worse. “Public health across the country got almost 95% diverted to doing covid care,” said Jonathan Iralu, the Indian Health Service chief clinical consultant for infectious diseases, who is based at the Gallup Indian Medical Center. “This was a really hard-hit area.”
At one point early in the pandemic, the Navajo Nation reported the highest covid rate in the U.S. Iralu suspects patients with syphilis symptoms may have avoided seeing a doctor for fear of catching covid. That said, he doesn’t think it’s fair to blame the pandemic for the high rates of syphilis, or the high rates of women passing infections to their babies during pregnancy, that continue four years later.
Native Americans are more likely to live in rural areas, far from hospital obstetric units, than any other racial or ethnic group. As a result, many do not receive prenatal care until later in pregnancy, if at all. That often means providers cannot test and treat patients for syphilis before delivery.
In New Mexico, 23% of patients did not receive prenatal care until the fifth month of pregnancy or later, or received fewer than half the appropriate number of visits for the infant’s gestational age in 2023 (the national average is less than 16%).
Inadequate prenatal care is especially risky for Native Americans, who have a greater chance than other ethnic groups of passing on a syphilis infection if they become pregnant. That’s because, among Native communities, syphilis infections are just as common in women as in men. In every other ethnic group, men are at least twice as likely to contract syphilis, largely because men who have sex with men are more susceptible to infection. O’Connell said it’s not clear why women in Native communities are disproportionately affected by syphilis.
“The Navajo Nation is a maternal health desert,” said Amanda Singer, a Diné (Navajo) doula and lactation counselor in Arizona who is also executive director of the Navajo Breastfeeding Coalition/Diné Doula Collective. On some parts of the reservation, patients have to drive more than 100 miles to reach obstetric services. “There’s a really high number of pregnant women who don’t get prenatal care throughout the whole pregnancy.”
She said that’s due not only to a lack of services but also to a mistrust of health care providers who don’t understand Native culture. Some also worry that providers might report patients who use illicit substances during their pregnancies to the police or child welfare. But it’s also because of a shrinking network of facilities: Two of the Navajo area’s labor and delivery wards have closed in the past decade. According to a recent report, more than half of U.S. rural hospitals no longer offer labor and delivery services.
Singer and the other doulas in her network believe New Mexico and Arizona could combat the syphilis epidemic by expanding access to prenatal care in rural Indigenous communities. Singer imagines a system in which midwives, doulas, and lactation counselors are able to travel to families and offer prenatal care “in their own home.”
O’Connell added that data-sharing arrangements between tribes and state, federal, and IHS offices vary widely across the country, but have posed an additional challenge to tackling the epidemic in some Native communities, including her own. Her Tribal Epidemiology Center is fighting to access South Dakota’s state data.
In the Navajo Nation and surrounding area, Iralu said, IHS infectious disease doctors meet with tribal officials every month, and he recommends that all IHS service areas have regular meetings of state, tribal, and IHS providers and public health nurses to ensure every pregnant person in those areas has been tested and treated.
IHS now recommends all patients be tested for syphilis yearly, and tests pregnant patients three times. It also expanded rapid and express testing and started offering DoxyPEP, an antibiotic that transgender women and men who have sex with men can take up to 72 hours after sex and that has been shown to reduce syphilis transmission by 87%. But perhaps the most significant change IHS has made is offering testing and treatment in the field.
Today, the public health nurses Wyaco supervises can test and treat patients for syphilis at home — something she couldn’t do when she was one of them just three years ago.
“Why not bring the penicillin to the patient instead of trying to drag the patient in to the penicillin?” said Iralu.
It’s not a tactic IHS uses for every patient, but it’s been effective in treating those who might pass an infection on to a partner or baby.
Iralu expects to see an expansion in street medicine in urban areas and van outreach in rural areas, in coming years, bringing more testing to communities — as well as an effort to put tests in patients’ hands through vending machines and the mail.
“This is a radical departure from our past,” he said. “But I think that’s the wave of the future.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post




Related Posts
-
Your Heart In Their Hands: Surgeon Preferences & Survival Rates
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Unless you are paying entirely out-of-pocket for a heart surgery, you will not usually get final say over which surgeon you get.
The surgeon, however, will have final say over what they actually do when they open you up.
And their preferences, it seems, can make all the difference:
MAG vs SAG
When doing coronary artery bypass grafting, (CABG), surgeons may prefer to do multi-arterial grafting (MAG) or single-arterial grafting (SAG).
Recently, there was a study analysing more than a million Americans who underwent CABG on Medicare over an 18-year period, looking at outcomes for MAG vs SAG.
The superficial news: those who received MAG had much better long-term survival chances than those who received SAG.
However: this may be less to do with the relative merits of the procedures themselves, and more to do with the preferences of the surgeon.
The “eyeball test”
If surgeons look at a patient and think they will not have many years to live after surgery, they may opt for the SAG, as the long-term benefits of the MAG will only manifest in the long-term.
This may seem a little self-defeating (indeed, maybe you won’t live to see the long-term if you don’t get the surgery type with the longer-term survival chances), there can be other factors involved, that may make surgeons more interested in your short-term survival chances.
Or you might just not have enough donor artery tissue available to pick and choose; after all, a person having a coronary artery bypass quite possibly won’t have great arteries in their arm or leg, either.
Or a person could be missing limbs (a common complication, given the comorbidities of both peripheral artery disease, and diabetes).
See also: How To Stay A Step Ahead Of Peripheral Artery Disease
Why it might be ok that things are like this
When factoring in surgeon preference for MAG or SAG as an instrumental variable, no significant difference in long-term survival was observed. This may explain inconsistencies with randomized controlled trials like the Arterial Revascularization Trial (ART), which also found no survival benefit of MAG over SAG.
Also, MAG recipients were generally younger, healthier, and from more resourceful areas, which likely had a further impact on MAG-giving decisions, and/but at the same time, may also have increased survival chances for reasons other than that they got MAG rather than SAG.
Here’s a pop-science article that goes into more detail about this:
Surgeon preferences may explain differences in CABG survival rates
How to look out for yourself, and advocate for yourself
…or your loved one, of course. Now, having a coronary artery bypass surgery of any kind is not a fun activity; it will be dangerous, it’ll be stressful before and after, and the recovery will often not be an easy time either. However, it is possible to learn more about what is going on / what will happen, ask the right questions, and get the best options for you (which may not always be the same as the best options for someone else).
We wrote about that in more detail here:
Nobody Likes Surgery, But Here’s How To Make It Much Less Bad
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Cardio and strength training boost health as you age. But don’t forget balance exercises to reduce your chance of falls
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We all recognise the benefits of regular aerobic or cardiovascular exercise to support our heart and lung health. Being active is also good for our social and mental health. And strength training promotes strong bones and muscles.
But as we age, we also need to train our balance to avoid falls.
Around one in three people aged 65 and over have a fall each year.
Falls are a common cause of disability and loss of independence in older age and can lead to an older person moving from living independently into living in a residential aged care facility. More than 6,000 older Australians die each year from falls.
But many falls are preventable. So exercise that targets balance and strength is crucial.
shurkin_son/Shutterstock How much do we need to do?
International guidelines recommend all older people exercise to prevent falls, even if they’ve never fallen. Prevention is far better than cure.
Other guidelines recommend people aged 65 and over do “functional balance and strength training” on three or more days a week, to improve their ability to do day-to-day activities, stay independent, and prevent falls.
Since balance starts to decline at around age 50, it’s even better to start training balance before the age of 65.
In order to increase our muscle strength, we need to progressively lift heavier weights. Similarly, to boost our balance, we need to practise activities that progressively challenge it. This improves our ability to stay steady in difficult situations and avoid falling.
Functional training means doing a physical activity that imitates everyday activities, such as standing up out of a chair, or stepping onto a step.
When you practise the everyday activities necessary for living independently, you improve your ability to perform them. This reduces the likelihood of falling when doing those activities, and therefore helps you maintain your independence for longer.
What exercises can you do?
The best exercises to challenge our balance system and reduce the risk of falling are performed while standing, rather than seated.
For example, you can stand with your feet close together or on one leg (if it’s safe to do so) while also performing controlled upper-body movements, such as leaning and reaching. This is a functional balance exercise and it can be made progressively more challenging as your balance improves.
Here are some exercises you can practise at home:
Sit to stand
Practise standing up from a seated position ten times every hour or so. See if you can do it without using your arms for support. To increase the balance challenge, place a cushion under the feet.
Heel-raises
Rise up onto your toes and hold the position for a few seconds. Hold on to a bench or wall for support if you need to but gradually remove the support as your balance improves. To increase the balance challenge, try doing this with your eyes closed.
You can make heel-raises progressively harder. Mary Rice/Shutterstock Heel-toe walking
Practise walking along an imaginary line, with one foot placed in front of the other. Hold on to a bench or wall for support if you need to but gradually remove the support as your balance improves.
Stepping in different directions
Practise quickly stepping forwards, sideways and backwards. Being able to move our feet quickly can help avoid a fall if you trip on something. If you are able, more challenging activities include stepping up or jumping onto a box.
Squats and lunges
Squats and lunges improve balance and leg strength. Add some hand weights to increase the challenge.
Squats improve balance and leg strength. LightField Studios/Shutterstock These examples and others can be found on the Safe Exercise at Home website.
Make it regular – and tailor it to your needs
It’s important that balance challenging exercises are performed regularly, at least three times per week. The benefits of exercise are lost if you stop doing them, so ongoing practice is important.
People of all abilities can safely undertake balance training exercise, however extra guidance and support is recommended for people who have physical limitations, are frail, or who are at a higher risk of falls.
For younger or fitter people, agility activities such as rapid stepping, dancing and running are likely to improve co-ordination and balance too.
So next time you are carrying out your exercise routine, ask yourself: what am I doing to improve my balance? Investing in balance training now can help you avoid falls, and lead to greater independence in older age.
Anne Tiedemann, Professor of Physical Activity and Health, University of Sydney; Cathie Sherrington, Professor, Institute for Musculoskeletal Health, School of Public Health, University of Sydney, and Geraldine Wallbank, Study Manager, PhD Candidate, Physiotherapist, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Migraine is more than just a headache. A neurologist explains the 4 stages
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A migraine attack is not just a “bad headache”.
Migraine is a debilitating neurological condition which can cause nausea, vomiting, and sensitivity to light or sound, in addition to severe headaches.
Migraine affects roughly five million Australians, but few people understand the different stages of a migraine attack.
Knowing the four distinct phases can help you recognise the symptoms and manage pain at each stage.
Karolina Grabowska/Pexels Phase 1: Premonitory
The first phase of migraine development is the “premonitory” or “prodrome” phase. It functions like a warning period which begins 24 to 48 hours before a migraine attack fully sets in.
The premonitory phase has a lot to do with the hypothalamus. The hypothalamus is the part of the brain which regulates key functions such as body temperature, appetite, mood and sleep.
When a person experiences a migraine attack, their hypothalamus becomes abnormally activated. The hypothalamus is connected to other parts of the brain with different functions, so this abnormal activation can also disrupt how those parts function.
This can lead to symptoms such as poor concentration, food cravings, irritability and insomnia. If you notice these early signs, you’re more likely to “catch” the start of a migraine attack and be able to treat it early.
Phase 2: Aura
The second phase of a migraine attack is called “aura”. Aura refers to various neurological symptoms which affect your vision, speech or ability to feel sensations. Visual auras, which mainly affect your vision, are the most common kind.
Visual aura symptoms can include seeing flashing lights, swirling shapes or blind spots. A sensory aura can lead to numbness or tingling in your face or limbs. In severe cases, people may even have trouble speaking.
Research suggests a process called cortical spreading depression contributes to aura symptoms. During this process, a wave of electrical activity spreads very slowly through the brain and can impact how certain brain regions function.
Only 30% of people experience migraine with aura.
Phase 3: Headache
The third phase of a migraine attack is the headache. This is when people typically experience a throbbing or pulsating headache, alongside other symptoms like nausea and sensitivity to light and sound.
This phase usually lasts between four and 72 hours if untreated.
When different brain networks become activated during a migraine attack, other symptoms can develop in addition to headache.
When the medulla or “vomit centre” of the brain is abnormally activated, it can lead to nausea and vomiting.
The trigeminal nerve, the nerve which allows you to feel sensations on your face, can also become abnormally activated. This causes the release of chemicals which may be perceived by the brain as pain.
One of these chemicals is a protein called calcitonin gene-related peptide (CGRP). Some injectable types of migraine medication block this protein to reduce pain.
Phase 4: Postdrome
The fourth and final phase is the “postdrome”. It is also known as the “migraine hangover”.
During this recovery phase, your brain is working hard to return to its normal functioning. That is why you may feel even more fatigued or have difficulty concentrating after a migraine attack.
So, how can I manage a migraine attack?
It helps to know the symptoms and stages of migraine development.
If you have predictable symptoms, particularly during the premonitory phase, it’s best to carry pain medications or anti-nausea tablets with you. That way you can treat early symptoms as soon as they arise. It can also be a sign to rest, ideally before the headache phase sets in.
In the aura phase, taking migraine-specific pain medications such as triptans, aspirin or anti-inflammatory pain killers may stop the headache phase from starting.
If you have more than four migraine attacks each month, you may also consider taking preventive medications. These are usually daily tablets which help control the baseline level of head pain you experience. Injectable options are also available.
Finally, don’t ignore the postdrome phase. If you push yourself too hard during this recovery period, you may experience overlapping migraine attacks. This is when one migraine attack starts before the last one resolves itself. Overlapping migraine attacks are much harder to treat.
You may also experience other symptoms related to the migraine attack. These can include dizziness, neck pain, or ringing in the ears. If you have any of these additional symptoms, you should consult your neurologist to check they are not caused by a more serious underlying condition.
And if you are a woman who experiences migraine with aura, speak to your doctor before starting hormone-based contraception. This is because you may need different treatment than someone who does not experience aura symptoms.
By understanding the different phases and symptoms of migraine, you will be better equipped to tackle any future attacks that come.
Lakshini Gunasekera, PhD Candidate in Neurology, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: