You Are Not a Before Picture – by Alex Light
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s that time of year, and many of us are looking at what we’ll do in the coming days, weeks, and months to level-up our health. So… Is this a demotivational book?
Quite the opposite! It’s rather a case of an often much-needed reminder to ensure that our plans are really our own, and really are what’s best for us. Why wouldn’t they be, you ask?
Much of diet culture (ubiquitous! From magazine covers to movie stars to the models advertising anything from health insurance to water filters) has us reaching for “body goals” that are not possible without a different skeleton and genes and compromises and post-production edits.
Alex Light—herself having moved from the fashion and beauty industry into health education—sets out in a clear, easy-reading manner, how we can look after ourselves, not be neglectful of our bodies, and/but also not get distracted into unhelpful, impossible, castles-in-the-air.
Bottom line: you cannot self-hate your way into good health, and good health will always be much more attainable than a body that’s just not yours. This book can help you sort out which is which.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What Weston Price Got Right (And Wrong)

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Weston Price: What Stood The Test of Time?

This is Dr. Weston Price, a dentist. You may guess from the photo, or perhaps already knew, his work is not new in 2023. We usually feature current health experts here, but we’re taking a day to do a blast from the past, because his ideas endure today, and inform a lot of people’s health views. So, he’s a good one to at least know about.
What was his deal?
Dr. Price (1870–1948) wanted to study focal infection theory—the idea that repairing root canals allowed bacterial infections that caused everything from heart disease to arthritis. His solution was that the teeth should be extracted instead.
This theory was popular in the 1920s, was challenged in the 1930s, ignored in the 1940s (the world was a bit busy), and by broad medical consensus anyway, rejected in the 1950s. But, while it was being challenged in the 1930s, Dr. Price decided to find more evidence for its support.
The result was his famous world tour of peoples living traditional lifestyles without the influence of “modern” diet. His findings, and the conclusions he drew from them, extended to far more than just dental health.
What did he find?
Dr. Price found that people living traditional lifestyles, with their traditional diets based on locally-sourced foods, had much better overall health. Of course, he was a dentist and not a general practitioner, so aside from examining their teeth, he largely relied on self-reported diagnoses of illness, or lack thereof.
In short: he found that people in places without modern medical institutions had fewer diagnoses of disease. From this, he concluded that incidence of disease was much lower.
There was also an unexamined element of survivorship bias—an undiagnosed disease is more likely to be fatal, and he questioned only living people, which skewed the stats rather. Nor did he examine infant mortality rate nor adult life expectancy, both of which were not great.
Was it all useless, then?
Actually no! He did hit upon some observations that have stood the test of time:
- He correctly concluded that modern diets with sugar and white flour were ruinous to the health.
- He correctly concluded that locally-sourced food, and grass-fed in the case of pastoral farming, tended to have much more nutritional value than the mass-produced results of intensive farming.
- He correctly concluded that many modern preservation methods robbed foods of their nutrients.
- He correctly concluded that many grains and seeds are more nutritions when fermented/soaked/sprouted.
About that “locally-sourced food”: the reason locally-sourced food tends to be more nutritious is that it has required less in the way of preservation for a long trip around the world, and will also tend to be fresher.
On the other hand, this does mean a lot of the foods that Dr. Price recommends are very much subject to availability. It may well be true that the Inuit people do not eat a lot of fruit and veg (which mostly do not grow there), but if you live in Nevada, maybe locally-sourced whale fat is just as difficult to find.
One person’s “this fatty organ meat contains the vitamin C we need” may be another person’s “that’s great; I have an apple tree in my garden though”.
Want to learn more?
Dr. Price’s most influential work is his magnum opus, “Nutrition and Physical Degeneration”. It’s a fascinating book in its historical context, but do be warned, it was written by a rich white man in 1939 and the writing is as racist as you might expect. Even when making favourable comparisons, the tone is very much “and here is what these savages are doing well”.
If you don’t fancy reading all that, here are two other sources about Weston Price’s work and conclusions, presented for balance:
- The Weston A. Price Foundation (Official Website)
- Weston Price’s Appalling Legacy (Science-Based Medicine.org)
Enjoy!
Share This Post
-

GABA Against Stress/Anxiety
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A Neurotransmitter Less Talked-About
GABA is taken by many people as a supplement, mostly as a mood modifier, though its health claims go beyond the recreational—and also, we’re of the opinion that mental health is also just health, and if it works, it works. We’ll explore some of the claims and science behind them today…
What is GABA?
GABA stands for gamma-aminobutyric acid, and it’s a neurotransmitter. It’s a lot less talked-about than for example dopamine or serotonin, but it’s very important nonetheless.
We make it ourselves inside our body, and we can also get it from our food, or supplement it, and some drugs will also have an effect on its presence and/or activity in our body.
What foods is it found in?
- Animals, obviously (just like in human brains*)
- Fermented foods (many kinds)
- Yeast
- Tea
- Tomatoes
- Mulberries
For more details, see:
γ-Aminobutyric acid found in fermented foods and beverages: current trends
*However, we do not recommend eating human brains, due to the risk of CJD and prion diseases in general.
What claims are made about it and are they true?
For brevity, we’ll give a little spoiler up-front: all the popular claims for it appear to be valid, though there’s definitely room for a lot more human trials (we skipped over a lot of rodent studies today!).
So we’ll just drop some of its main benefits, and human studies to back those.
Reduction of stress and anxiety
GABA decreases task-related stress and anxiety within 30 minutes of being taken, both in subjective measures (i.e., self-reports) and in objective clinical physiological measures:
Cognitive enhancement
It’s not a does-everything nootropic like some, but it does have clear benefits to episodic memory:
❝GABA intake might help to distribute limited attentional resources more efficiently, and can specifically improve the identification and ordering of visual events that occur in close temporal succession❞
One of the things that makes this one important is that it also deals with the often-asked question of “does GABA pass the blood-brain barrier”:
❝The present findings do give further credence to the idea that oral ingestion does allow GABA to reach the brain and exert direct effects on cognition, which in the present case were specific to temporal attention.❞
Read more:
Supplementation of gamma-aminobutyric acid (GABA) affects temporal, but not spatial visual attention
Potential for more
We take care to give good quality sources, so the following study comes with a big caveat that it has since been retracted. Why was it retracted, you wonder?
It’s about the sample; they cite “30 healthy adults”, but neglected tp mention that this figure was initially 46. What happened to the other 16 participants is unclear, but given that this was challenged and the challenge not answered, it was sufficient for the journal (Nature) to pull the study, in case of deliberate sample bias.
However! Running the numbers in their results section, a probability of 0.03 is very compelling unless the disappearance of 16 subjects was outright fraudulent (which we regrettably cannot know either way).
Here’s the study (so take it with a pinch of salt, considering the above), and taken at face value, it shows how GABA supplementation improves accurate reactions to fast-moving visual and auditory stimuli:
RETRACTED ARTICLE: γ-Aminobutyric acid (GABA) administration improves action selection processes: a randomised controlled trial
…so, hopefully this experiment will be repeated, without disappearing participants!
The sweet spot
You may be wondering how something that slows a person down (having a relaxing effect) can also speed a person up. This has to do with what it is and isn’t affecting; think of it like a “focus mode” on your computer or other device that greys-out everything else a bit so that you can focus on what you’re doing.
It’s in some ways (by different neurochemical pathways, though) a similar effect to the “relaxed alertness” created by l-theanine supplementation.
There’s also a sweet spot whereby GABA is toning some things down just the right amount, without adversely affecting performance in areas we don’t want slowed down. For the science of this, see:
Is it safe?
GABA is “Generally Recognized As Safe”. However:
- you should speak with your pharmacist if you are taking any medications for blood pressure or epilepsy, as GABA supplementation may cause them to work too well.
- you should absolutely not take GABA with alcohol or opioids as (dose-dependent for all the substances involved, and also depending on your metabolic base rate and other factors) its acute depression of the CNS can mean you relax and slow down too much, and you may find yourself not breathing often enough to sustain life.
Aside from that, it is considered safe up to at least 1g/kg/day*. Given that popular doses are 120–750mg, and most people weigh more than 750g, this is very safe for most people:
United States Pharmacopeia (USP) Safety Review of Gamma-Aminobutyric Acid (GABA)
Where can I get it?
We don’t sell it, but for your convenience, here’s an example product on Amazon
Enjoy!
Share This Post
-

Insomnia? High blood pressure? Try these!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Your Questions, Our Answers!
Q: Recipes for insomnia and high blood pressure and good foods to eat for these conditions?
A: Insomnia can be caused by many things, and consequently can often require a very multi-vector approach to fixing it. But, we’ll start by answering the question you asked (and probably address the rest of dealing with insomnia in another day’s edition!):
- First, you want food that’s easy to digest. Broadly speaking, this means plant-based. If not plant-based, fish (unless you have an allergy, obviously) is generally good and certainly better than white meat, which is better than red meat. In the category of dairy, it depends so much on what it is, that we’re not going to try to break it down here. If in doubt, skip it.
- You also don’t want blood sugar spikes, so it’s good to lay off the added sugar and white flour (or white flour derivatives, like white pasta), especially in your last meal of the day.
- Magnesium supports healthy sleep. A fine option would be our shchi recipe, but using collard greens rather than cabbage. Cabbage is a wonderful food, but collard greens are much higher in magnesium. Remember to add plenty of mushrooms (unless you don’t like them), as they’re typically high in magnesium too.
As for blood pressure, last month we gave tips (and a book recommendation) for heart health. The book, Dr. Monique Tello’s “Healthy Habits for Your Heart: 100 Simple, Effective Ways to Lower Your Blood Pressure and Maintain Your Heart’s Health”, also has recipes!
Here’s one from the “mains” section:
Secret Ingredient Baltimore-Style Salmon Patties with Not-Oily Aioli
❝This is a family favorite, and no one knows that it features puréed pumpkin! Most salmon cake recipes all for eggs and bread crumbs as binders, but puréed pumpkin and grated carrot work just as well, lend a beautiful color, and add plenty of fiber and plant nutrients. Canned salmon is way cheaper than fresh and has just as much omega-3 PUFAs and calcium. Serve this alongside a salad (the Summer Corn, Tomato, Spinach, and Basil Salad would go perfectly) for a well-rounded meal.❞
Serves 4 (1 large patty each)
Secret Ingredient Baltimore-Style Salmon Patties:
- 1 (15-oz) can pink salmon, no salt added
- ½ cup puréed pumpkin
- ½ cup grated carrot (I use a handheld box grater)
- 2 tablespoons minced chives (Don’t have chives? Minced green onions or any onions will do)
- 2 teaspoons Old Bay Seasoning
- 1 tablespoon olive oil
- ½ large lemon, sliced, for serving
Not-Oily Aioli:
- ½ cup plain low-fat Greek yogurt
- Juice and zest from ½ large lemon
- 1 clove garlic, crushed and minced fine
- 2 tablespoons chopped fresh dill
- For the patties: mix all the ingredients for the salmon patties together in a medium bowl
- Form patties with your hands and set on a plate or tray (you should have 4 burger-sized patties)
- Heat oil in a large skillet over medium heat.
- Set patties in a skillet and brown for 4 minutes, then carefully flip.
- Brown the other side, then serve hot.
- For the Aioli: mix all the ingredients for the aioli together in a small bowl.
- Plop a dollop alongside or on top of each salmon patty and serve with a spice of lemon.
Per serving: Calories: 367 | Fat: 13.6g | Saturated Fat: 4.4g | Protein: 46g | Sodium: 519mg | Carbohydrates: 13.2g | Fiber: 1.3g | Sugars: 9g | Calcium: 505mg | Iron: 1mg | Potassium 696mg
Notes from the 10almond team:
- If you want to make it plant-based, substitute cooked red lentils (no salt added) for the tinned salmon, and plant-based yogurt for the Greek yogurt
- We recommend adding more garlic. Seriously, who uses 1 clove of garlic for anything, let alone divided between four portions?
- The salads mentioned are given as recipes elsewhere in the same book. We strongly recommend getting her book, if you’re interested in heart health!
Do you have a question you’d like to see answered here? Hit reply or use the feedback widget at the bottom; we’d love to hear from you!
Share This Post

Related Posts
-

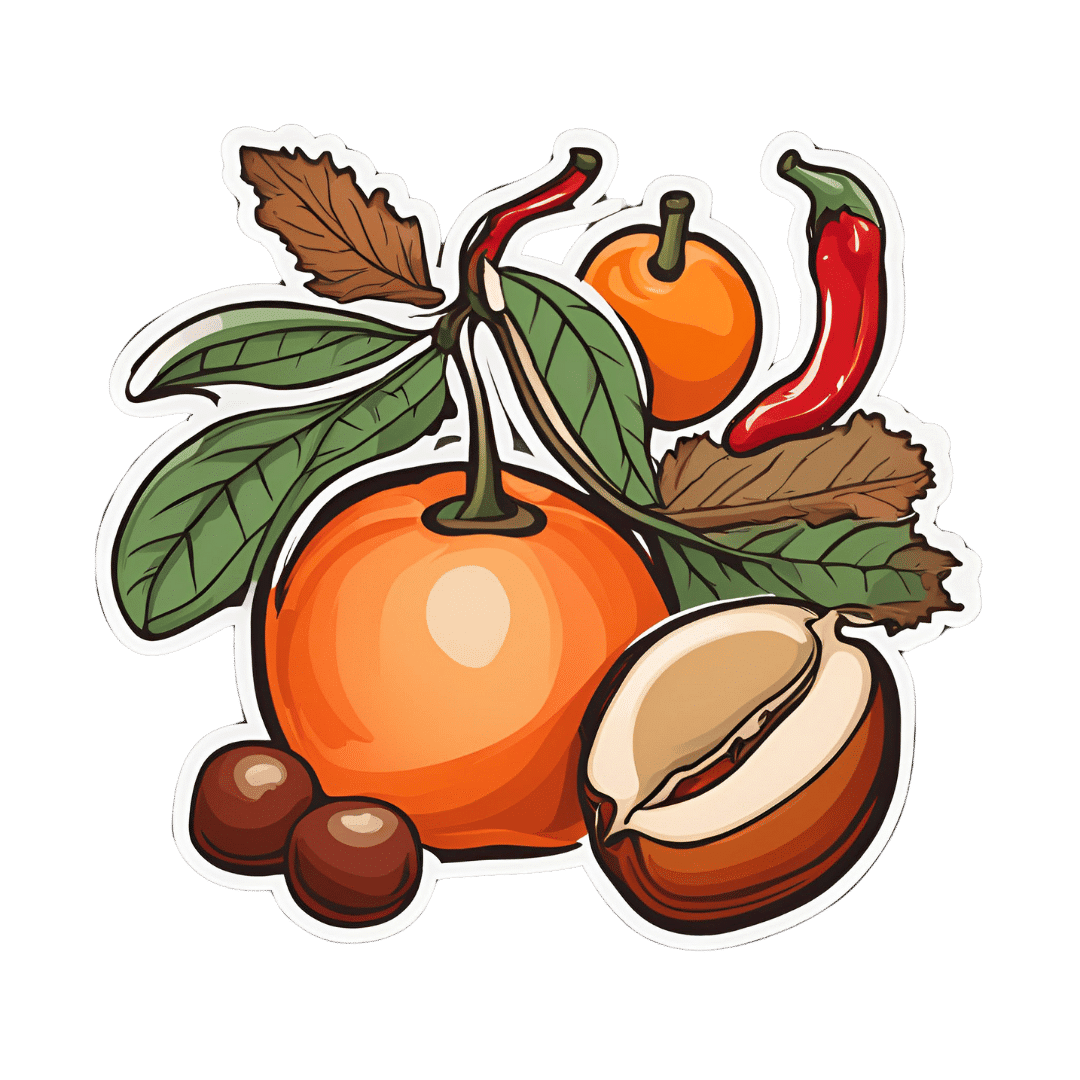
Chili Chestnut, Sweet Apricot, & Whipped Feta Toasts
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a delightful breakfast or light lunch option, full of gut-healthy ingredients and a fair list of healthy polyphenols too.
You will need
- ½ baguette, sliced into ½” slices; if making your own, feel free to use our Delicious Quinoa Avocado Bread recipe. If buying shop-bought, a sourdough baguette will likely be the healthiest option, and tasty too.
- 4 oz feta cheese; if you are vegan, a plant-based version will work in culinary terms, but will have a different (less gut-healthy) nutritional profile, as plant-based cheeses generally use a lot of coconut oil and potato starch, and are not actually fermented.
- 1 tbsp yogurt; your preference what kind; live-cultured with minimal additives is of course best—and this time, plant-based is also just as good, healthwise, since they are fermented and contain more or less the same beneficial bacteria, and have a good macro profile too.
- 4 oz precooked chestnuts, finely chopped
- 6 dried apricots, finely chopped
- ¼ bulb garlic, grated
- 2 tsp harissa paste
- 1 tsp black pepper, coarse ground
- ¼ tsp MSG or ½ tsp low-sodium salt
- Extra virgin olive oil, for frying
- Optional garnish: finely chopped chives
Method
(we suggest you read everything at least once before doing anything)
1) Combine the feta and yogurt in a small, high-speed blender and process into a smooth purée. If it isn’t working, add 1 tbsp kettle-hot water and try again.
2) Heat the oil in a skillet over a medium heat; add the garlic and when it starts to turn golden, add the chestnuts and harissa, as well as the black pepper and MSG/salt. Stir for about 2 minutes, and then stir in the apricots and take it off the heat.
3) Toast the baguette slices under the grill. If you’re feeling bold about the multitasking, you can start this while still doing the previous step, for optimal timing. If not, simply doing it in the order presented is fine.
4) Assemble: spread the whipped feta over the toast; add the apricot-chestnut mixture, followed by the finely chopped chives if using, and serve immediately:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Making Friends With Your Gut (You Can Thank Us Later)
- Apricots vs Peaches – Which is Healthier?
- Why You Should Diversify Your Nuts!
- Capsaicin For Weight Loss And Against Inflammation
- The Many Health Benefits Of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- Sea Salt vs MSG – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Reading As A Cognitive Exercise
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Reading, Better
It is relatively uncontroversial to say that reading is good for cognitive health, but we don’t like to make claims without science if we can help it, so let’s get started:
There was a 2021 study, which found that even when controlling for many other factors, including highest level of education, socioeconomic status, and generalized pre-morbid intelligence:
❝high reading activity, as defined by almost daily reading, was associated with lower odds of cognitive decline, compared to low reading activity❞
Source: Can reading increase cognitive reserve?
However, not all reading is the same. And this isn’t just about complexity or size of vocabulary, either. It’s about engagement.
And that level of engagement remains the key factor, no matter how quickly or slowly someone reads, as the brain tends to automatically adjust reading speed per complexity, because the brain’s “processing speed” remains the same:
Read more: Cognitive coupling during reading
Everyone’s “processing speed” is different (and is associated with generalized intelligence and executive functions), though as a general rule of thumb, the more we practice it, the faster our processing speed gets. So if you balked at the notion of “generalized intelligence” being a factor, be reassured that this association goes both ways.
So is the key to just read more?
That’s a great first step! But…
The key factor still remains: engagement.
So what does that mean?
It is not just the text that engages you. You must also engage the text!
This is akin to the difference between learning to drive by watching someone else do it, and learning by getting behind the wheel and having a go.
When it comes to reading, it should not be a purely passive thing. Sure, if you are reading a fiction book at bedtime, get lost in it, by all means. But when it comes to non-fiction reading, engage with it actively!
For example, I (your writer here, hi), when reading non-fiction:
- Read at what is generally considered an unusually fast pace, but
- Write so many notes in the margins of physical books, and
- Write so many notes using the “Notes” function on my Kindle
And this isn’t just like a studious student taking notes. Half the time I am…
- objecting to content (disagreeing with the author), or
- at least questioning it, or which is especially important, or
- noting down questions that came to my mind as a result of what I am reading.
This latter is a bit like:
- when you are reading 10almonds, sometimes you will follow our links and go off down a research rabbit-hole of your own, and that’s great!
- sometimes you will disagree with something and write to tell us, and that’s great too (when this happens, one or the other or all of us will learn something, and yes, we have published corrections before now)!
- sometimes what you read here will prompt a further question, and you’ll send that to us, and guess what, also great! We love questions.
Now, if your enjoyment of 10almonds is entirely passive, don’t let us stop you (we know our readers like quick-and-easy knowledge, and that’s good too), it’s just, the more you actively engage with it, the more you’ll get out of it.
This, by the way, was also a lifelong habit of Leonardo da Vinci, which you can read about here:
How to Think Like Leonardo da Vinci: Seven Steps to Genius Every Day – by Michael J. Gelb
a very good book that we reviewed last year
How you read (i.e. what medium) matters too!
Are you reading this on a desktop/laptop, or a mobile device? That difference could matter more than the difference between paper and digital, according to this study from 2020 that found…
❝The cumulation of evidence from this and previous studies suggests that reading on a tablet affords different interactions between the reader and the text than reading on a computer screen.
Reading on a tablet might be more similar to reading on paper, and this may impact the attentional processes during reading❞
What if my mind wanders easily?
You can either go with it, or train to improve focus.
Going with it: just make sure you have more engaging reading to get distracted by. It’s all good.
Training focus: this is trickier, but worthwhile, as executive function (you will remember from earlier) was an important factor too, and training focus is training executive function.
As for one way to do that…
If you’d like a primer for getting going with that, then you may enjoy our previous main feature:
No-Frills, Evidence-Based Mindfulness
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Five Key Traits Of Healthy Aging
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Five Keys Of Aging Healthily
Image courtesy of Peter Prato. This is Dr. Daniel Levitin. He’s a neuroscientist, and his research focuses on aging, the brain, health, productivity, and creativity. Also music, and he himself is an accomplished musician also, but we’re not going to be focusing on that today.
We’re going to be looking at the traits that, according to science, promote healthy longevity in old age. In other words, the things that increase our healthspan, from the perspective of a cognitive scientist.
What does he say we should do?
Dr. Levitin offers us what he calls the “COACH” traits:
- Curiosity
- Openness
- Associations
- Conscientiousness
- Healthy practices
By “associations”, he means relationships. However, that would have made the acronym “CORCH”, and decisions had to be made.
Curiosity
Leonardo da Vinci had a list of seven traits he considered most important.
We’ll not go into those today (he is not our featured expert of the day!), but we will say that he agreed with Dr. Levitin on what goes at the top of the list: curiosity.
- Without curiosity, we will tend not to learn things, and learning things is key to keeping good cognitive function in old age
- Without curiosity, we will tend not to form hypotheses about how/why things are the way they are, so we will not exercise imagination, creativity, problem-solving, and other key functions of our brain
- Without curiosity, we will tend not to seek out new experiences, and consequently, our stimuli will be limited—and thus, so will our brains
Openness
Being curious about taking up ballroom dancing will do little for you, if you are not also open to actually trying it. But, openness is not just a tag-on to curiosity; it deserves its spot in its own right too.
Sometimes, ideas and opportunities come to us unbidden, and we have to be able to be open to those too. This doesn’t mean being naïve, but it does mean having at least a position of open-minded skepticism.
Basically, Dr. Levitin is asking us to be the opposite of the pejorative stereotype of “an old person stuck in their ways”.
Associations
People are complex, and so they bring complexities to our lives. Hopefully, positively stimulating ones. Without them to challenge us (again, hopefully in a positive way), we can get very stuck in a narrow field of experience.
And of course, having at least a few good friends has numerous benefits to health. There’s been a lot of research on this; 5 appears to be optimal.
- More than that, and the depth tends to tail off, and/or stresses ensue from juggling too many relationships
- Fewer than that, and we might be only a calendar clash away from loneliness
Friends provide social stimulation and mutual support; they’re good for our mental health and even our physiological immunity (counterintuitively, by means of shared germs).
And, a strong secure romantic relationship is something that has been found time and again to extend healthy life.
Note: by popular statistics, this benefit is conferred upon men partnered with women, men partnered with men, women partnered with women, but not women partnered with men.
There may be a causative factor that’s beyond the scope of this article which is about cognitive science, not feminism, but there could also be a mathematical explanation for this apparent odd-one-out:
Since women tend to live longer than men (who are also often older than their female partners), women who live the longest are often not in a relationship—precisely because they are widows. So these long-lived widows will tend to skew the stats, through no fault of their husbands.
On the flipside of this, for a woman to predecease her (statistically older and shorter-lived) husband will often require that she die quite early (perhaps due to accident or illness unrelated to age), which will again skew the stats to “women married to men die younger”, without anything nefarious going on.
Conscientiousness
People who score highly in the character trait “conscientiousness” will tend to live longer. The impact is so great, that a child’s scores will tend to dictate who dies in their 60s or their 80s, for example.
What does conscientiousness mean? It’s a broad character trait that’s scored in psychometric tests, so it can be things that have a direct impact on health, such as brushing one’s teeth, or things that are merely correlated, such as checking one’s work for typos (this writer does her best!).
In short, if you are the sort of person who attends to the paperwork for your taxes on time, you are probably also the sort of person who remembers to get your flu vaccination and cancer screening.
Healthy practices
This means “the usual things”, such as:
- Healthy diet (Mediterranean Diet consistently scores up top)
- Good exercise (especially the tendency to keep moving in general)
- Good sleep (7–9 hours, no compromises)
- Not drinking (or at least only very moderate consumption, but the only safe amount is zero)
- Not smoking (just don’t; there is no wiggle room on this one)
Want to learn more?
You can check out his book, which we reviewed all so recently, and you can also enjoy this video, in which he talks about matters concerning healthy aging from a neuroscientist’s perspective, ranging from heart health and neurodegeneration, to the myth of failing memory, to music and lifespan and more:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: