The Prediabetes Diet Plan – by Hillary Wright
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, who this is not for: if you are diabetic (or perhaps cook for a loved one who is) and that has been the case for some time, then while technically the same dietary approach will indeed be generally good, the fact is that you probably know everything in this book already by now (assuming you have researched the topic, as people in such situations tend to do).
However, if you’ve just received a prediabetes diagnosis and are now at the point of “Ahhhh I know nothing about this and had better learn quickly”, then this book is indeed for you, as it explains everything you’ll need to know, from a scientific standpoint and with practical pointers.
The author, a registered dietician nutritionist (RDN), also has a Master’s of Health Education, and it shows in how well she communicates the necessary information here; it’s very simple without omitting important information, and jargon-free without “dumbing down”.
The “Diet Plan” part of the title might lead you to expect there will be a lot of recipes and then perhaps a 28-day meal plan; no, there are no recipes, and there is a 3-day meal plan.
You may be wondering: how does one do a meal plan without recipes? And the answer is that it’s about food groups, portions, and assumed general knowledge (for example, one can say “avocado toast” and not include a recipe for such and the reader will still usually be comfortable making their own).
Bottom line: this is a very respectable guide to the science of avoiding/reversing prediabetes.
Click here to check out The Prediabetes Diet Plan, and get planning!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Estrogen & Progesterone Affect Your Pain

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s been long-established that pain perception in women and men is quite different—on average, at least, since the datasets are usually somewhat overlapping.
If that last statement is confusing, think of it like height: on average, men are taller than women, but the datasets of “men’s height” and “women’s height” will be overlapping, because indeed some women are taller than some men.
So it is with pain also: women generally have heightened pain sensitivity compared to men, although reporting of that pain can vary a lot depending on the circumstances and experimental methodology.
An additional consideration is that women are overrepresented when it comes to people with chronic pain (i.e., more women have chronic pain than men).
In some cases, this is because a given chronic condition (as for example many autoimmune diseases) predominantly affects women for reasons that are often not well-explored, and in other cases, the reason is more obvious (for example, you will not find many men with endometriosis).
See also: What you need to know about endometriosis
Researchers, namely, Dr. Élora Midavaine et al., have found another common reason for the disparity in pain perception:
From estrogen to opioids
It turns out that the main female sex hormones, estrogen and progesterone, can suppress pain by prompting immune cells near the spinal cord to produce opioids.
The immune cells in question are immune-regulatory T-cells (colloquially called “Tregs” by scientists who don’t want to have to say/write that in full every time), whose main job is usually simply reducing inflammation. In other words, they’re the immune cells that tell your other immune cells to kindly chill a little bit and not overdo it.
In this case, the estrogen and progesterone stimulate the Tregs to produce the opioids (specifically, enkephalin) to block the pain signals before they reach the brain.
You may be thinking: but hang on, wouldn’t this mean that women experience less pain than men?
And the answer is: it depends!
A while back we wrote an article about how Alzheimer’s Sex Differences May Not Be What They Appear, and it’s a similar principle in this case: the female sex hormones are protective… Until they’re not!
In other words: in menopause, for example. And just like Alzheimer’s, chronic pain increasingly affects people the older we get, so the majority of people experiencing it at any time will tend to be postmenopausal. Symptoms get brushed off with “well, you are older now”, and while yes indeed many things may be age-related, in some cases their pathogenesis can be very clearly traced to “this hormone was doing the job for you, and now your levels of that hormone are very low, so you no longer get that protection”.
You can find the paper itself here: Meningeal regulatory T cells inhibit nociception in female mice ← yes, it’s a mouse study, but all the systems exist the same way in humans, so there is no reason to assume it would be different for us. Just, scientists can’t persuade an ethics board to let them knock out humans’ Tregs with toxins and then do nerve damage to measure the pain processing.
Takeaway idea: if you are postmenopausal and suffer chronic pain, then it’s an extra reason you might want to consider bioidentical HRT if you haven’t already.
See also: What You Should Have Been Told About The Menopause Beforehand
Want to learn more?
We’ve written quite a bit about pain management, including:
- Before You Reach For That Tylenol…
- How To Stop Pain Spreading
- How To Dial Down Your Pain
- Managing Chronic Pain (Realistically!)
- Get The Right Help For Your Pain
- The 7 Approaches To Pain Management
- Science-Based Alternative Pain Relief (When Painkillers Aren’t Helping, These Things Might)
Take care!
Share This Post
-
Grapes vs Mango – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing grapes to mango, we picked the mango.
Why?
In terms of macros, grapes have more carbs while mangos have more fiber and protein, winning.
In the category of vitamins, grapes have more of vitamins B1, B2, and K, while mangos have more of vitamins A, B3, B5, B6, B7, B9, C, and E, winning easily again.
Looking at minerals, grapes have more calcium, iron, manganese, and potassium, while mangos have more copper, magnesium, phosphorus, selenium, and zinc, winning for a third time in a row.
In other considerations, grapes do have more polyphenols, so that is a point in their favor.
Adding up the sections makes for a clear overall win for mangos, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
Can We Drink To Good Health? ← while there are polyphenols such as resveratrol in red wine that per se would boost heart health, there’s so little per glass that you may need 100–1000 glasses per day to get the dosage that provides benefits in mouse studies.
If you’re not a mouse, you might even need more than that!
To this end, many people prefer resveratrol supplementation ← link is to an example product on Amazon, but there are plenty more so feel free to shop around 😎
Enjoy!
Share This Post
-

General Tso’s Chickpeas
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A fiber-rich, heart-healthy take on a classic:
You will need
- 1 can chickpeas, drained
- ¾ cup vegetable stock; ideally you made this yourself from vegetable cuttings that you kept in the freezer for this purpose, but failing that, you should be able to get low-sodium stock cubes at your local supermarket.
- ¼ cup arrowroot starch (cornstarch will do at a pinch, but arrowroot is better and has no flavor of its own)
- 3 tbsp coconut oil
- 2 tbsp grated fresh ginger
- ¼ bulb garlic, minced
- 2 tbsp honey (or maple syrup if you prefer, and if you don’t like sweetness, reduce this to 1 tbsp or even omit entirely, though it won’t be quite so “General Tso” if you do, but it’s your meal!)
- 2 tbsp tomato paste
- 2 tsp hot sauce
- 1 tsp black pepper, coarse ground
- 3 green onions, sliced
Method
(we suggest you read everything at least once before doing anything)
1) Coat the chickpeas in the arrowroot starch by tossing them together in a bowl
2) Heat the coconut oil in a skillet on a medium-high heat, and when hot, add the chickpeas, stirring for 3 minutes
3) Add the remaining ingredients in the order we gave (except the vegetable stock, which goes in last), stirring for 5 more minutes, or until the sauce thickens
4) Serve with the carb of your choice; we recommend our Tasty Versatile Rice Recipe

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Eat More (Of This) For Lower Blood Pressure
- Honey vs Maple Syrup – Which is Healthier?
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Share This Post



Related Posts
-
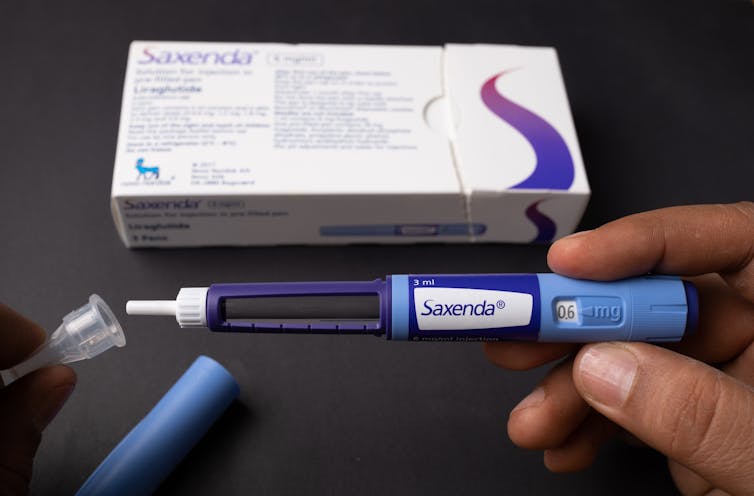
Ozempic’s cousin drug liraglutide is about to get cheaper. But how does it stack up?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fourteen years ago, the older drug cousin of semaglutide (Ozempic and Wegovy) came onto the market. The drug, liraglutide, is sold under the brand names Victoza and Saxenda.
Patents for Victoza and Saxenda have now expried. So other drug companies are working to develop “generic” versions. These are likely be a fraction of current cost, which is around A$400 a month.
So how does liraglutide compare with semaglutide?
Halfpoint/Shutterstock How do these drugs work?
Liraglutide was not originally developed as a weight-loss treatment. Like semaglutide (Ozempic), it originally treated type 2 diabetes.
The class of drugs liraglutide and semaglutide belong to are known as GLP-1 mimetics, meaning they mimic the natural hormone GLP-1. This hormone is released from your small intestines in response to food and acts in several ways to improve the way your body handles glucose (sugar).
How do they stop hunger?
Liraglutide acts in several regions of the unconscious part of your brain, specifically the hypothalamus, which controls metabolism, and parts of the brain stem responsible for communicating your body’s nutrient status to the hypothalamus.
Its actions here appear to reduce hunger in two different ways. First, it helps you to feel full earlier, making smaller meals more satisfying. Second, it alters your “motivational salience” towards food, meaning it reduces the amount of food you seek out.
Liraglutide’s original formulation, designed to treat type 2 diabetes, was marketed as Victoza. Its ability to cause weight loss was evident soon after it entered the market.
Shortly after, a stronger formulation, called Saxenda, was released, which was intended for weight loss in people with obesity.
How much weight can you lose with liraglutide?
People respond differently and will lose different amounts of weight. But here, we’ll note the average weight loss users can expect. Some will lose more (sometimes much more), others will lose less, and a small proportion won’t respond.
The first GLP-1 mimicking drug was exenatide (Bayetta). It’s still available for treating type 2 diabetes, but there are currently no generics. Exenatide does provide some weight loss, but this is quite modest, typically around 3-5% of body weight.
For liraglutide, those using the drug to treat obesity will use the stronger one (Saxenda), which typically gives about 10% weight loss.
Semaglutide, with the stronger formulation called Wegovy, typically results in 15% weight loss.
The newest GLP-1 mimicking drug on the market, tirzepatide (Mounjaro for type 2 diabetes and Zepbound for weight loss), results in weight loss of around 25% of body weight.
What happens when you stop taking them?
Despite the effectiveness of these medications in helping with weight loss, they do not appear to change people’s weight set-point.
So in many cases, when people stop taking them, they experience a rebound toward their original weight.
People often regain weight when when they stop taking the drug. Mohammed_Al_Ali/Shutterstock What is the dose and how often do you need to take it?
Liraglutide (Victoza) for type 2 diabetes is exactly the same drug as Saxenda for weight loss, but Saxenda is a higher dose.
Although the target for each formulation is the same (the GLP-1 receptor), for glucose control in type 2 diabetes, liraglutide has to (mainly) reach the pancreas.
But to achieve weight loss, it has to reach parts of the brain. This means crossing the blood-brain barrier – and not all of it makes it, meaning more has to be taken.
All the current formulations of GLP-1 mimicking drug are injectables. This won’t change when liraglutide generics hit the market.
However, they differ in how frequently they need to be injected. Liraglutide is a once-daily injection, whereas semaglutide and tirzepatide are once-weekly. (That makes semaglutide and tirzepatide much more attractive, but we won’t see semaglutide as a generic until 2033.)
What are the side effects?
Because all these medicines have the same target in the body, they mostly have the same side effects.
The most common are a range of gastrointestinal upsets including nausea, vomiting, bloating, constipation and diarrhoea. These occur, in part, because these medications slow the movement of food out of the stomach, but are generally managed by increasing the dose slowly.
Recent clinical data suggests the slowing in emptying of the stomach can be problematic for some people, and may increase the risk of of food entering the lungs during operations, so it is important to let your doctor know if you are taking any of these drugs.
Because these are injectables, they can also lead to injection-site reactions.
Gastrointestinal side effects are most common. Halfpoint/Shutterstock During clinical trials, there were some reports of thyroid disease and pancreatitis (inflammation of the pancreas). However, it is not clear that these can be attributed to GLP-1 mimicking drugs.
In animals, GLP-1 mimicking drugs drugs have been found to negatively alter the growth of the embryo. There is currently no controlled clinical trial data on their use during pregnancy, but based on animal data, these medicines should not be used during pregnancy.
Who can use them?
The GLP-1 mimicking drugs for weight loss (Wegovy, Saxenda, Zepbound/Mounjaro) are approved for use by people with obesity and are meant to only be used in conjunction with diet and exercise.
These drugs must be prescribed by a doctor and for obesity are not covered by the Pharmaceutical Benefits Scheme, which is one of the reasons why they are expensive. But in time, generic versions of liraglutide are likely to be more affordable.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Pain Clinics Made Millions From ‘Unnecessary’ Injections Into ‘Human Pin Cushions’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
McMINNVILLE, Tenn. — Each month, Michelle Shaw went to a pain clinic to get the shots that made her back feel worse — so she could get the pills that made her back feel better.
Shaw, 56, who has been dependent on opioid painkillers since she injured her back in a fall a decade ago, said in both an interview with KFF Health News and in sworn courtroom testimony that the Tennessee clinic would write the prescriptions only if she first agreed to receive three or four “very painful” injections of another medicine along her spine.
The clinic claimed the injections were steroids that would relieve her pain, Shaw said, but with each shot her agony would grow. Shaw said she eventually tried to decline the shots, then the clinic issued an ultimatum: Take the injections or get her painkillers somewhere else.
“I had nowhere else to go at the time,” Shaw testified, according to a federal court transcript. “I was stuck.”
Shaw was among thousands of patients of Pain MD, a multistate pain management company that was once among the nation’s most prolific users of what it referred to as “tendon origin injections,” which normally inject a single dose of steroids to relieve stiff or painful joints. As many doctors were scaling back their use of prescription painkillers due to the opioid crisis, Pain MD paired opioids with monthly injections into patients’ backs, claiming the shots could ease pain and potentially lessen reliance on painkillers, according to federal court documents.
Now, years later, Pain MD’s injections have been proved in court to be part of a decade-long fraud scheme that made millions by capitalizing on patients’ dependence on opioids. The Department of Justice has successfully argued at trial that Pain MD’s “unnecessary and expensive injections” were largely ineffective because they targeted the wrong body part, contained short-lived numbing medications but no steroids, and appeared to be based on test shots given to cadavers — people who felt neither pain nor relief because they were dead.
Four Pain MD employees have pleaded guilty or been convicted of health care fraud, including company president Michael Kestner, who was found guilty of 13 felonies at an October trial in Nashville, Tennessee. According to a transcript from Kestner’s trial that became public in December, witnesses testified that the company documented giving patients about 700,000 total injections over about eight years and said some patients got as many as 24 shots at once.
“The defendant, Michael Kestner, found out about an injection that could be billed a lot and paid well,” said federal prosecutor James V. Hayes as the trial began, according to the transcript. “And they turned some patients into human pin cushions.”
The Department of Justice declined to comment for this article. Kestner’s attorneys either declined to comment or did not respond to requests for an interview. At trial, Kestner’s attorneys argued that he was a well-intentioned businessman who wanted to run pain clinics that offered more than just pills. He is scheduled to be sentenced on April 21 in a federal court in Nashville.
According to the transcript of Kestner’s trial, Shaw and three other former patients testified that Pain MD’s injections did not ease their pain and sometimes made it worse. The patients said they tolerated the shots only so Pain MD wouldn’t cut off their prescriptions, without which they might have spiraled into withdrawal.
“They told me that if I didn’t take the shots — because I said they didn’t help — I would not get my medication,” testified Patricia McNeil, a former patient in Tennessee, according to the trial transcript. “I took the shots to get my medication.”
In her interview with KFF Health News, Shaw said that often she would arrive at the Pain MD clinic walking with a cane but would leave in a wheelchair because the injections left her in too much pain to walk.
“That was the pain clinic that was supposed to be helping me,” Shaw said in her interview. “I would come home crying. It just felt like they were using me.”
‘Not Actually Injections Into Tendons at All’
Pain MD, which sometimes operated under the name Mid-South Pain Management, ran as many as 20 clinics in Tennessee, Virginia, and North Carolina throughout much of the 2010s. Some clinics averaged more than 12 injections per patient each month, and at least two patients each received more than 500 shots in total, according to federal court documents.
All those injections added up. According to Medicare data filed in federal court, Pain MD and Mid-South Pain Management billed Medicare for more than 290,000 “tendon origin injections” from January 2010 to May 2018, which is about seven times that of any other Medicare biller in the U.S. over the same period.
Tens of thousands of additional injections were billed to Medicaid and Tricare during those same years, according to federal court documents. Pain MD billed these government programs for about $111 per injection and collected more than $5 million from the government for the shots, according to the court documents.
More injections were billed to private insurance too. Christy Wallace, an audit manager for BlueCross BlueShield of Tennessee, testified that Pain MD billed the insurance company about $40 million for more than 380,000 injections from January 2010 to March 2013. BlueCross paid out about $7 million before it cut off Pain MD, Wallace said.
These kinds of enormous billing allegations are not uncommon in health care fraud cases, in which fraudsters sometimes find a legitimate treatment that insurance will pay for and then overuse it to the point of absurdity, said Don Cochran, a former U.S. attorney for the Middle District of Tennessee.
Tennessee alone has seen fraud allegations for unnecessary billing of urine testing, skin creams, and other injections in just the past decade. Federal authorities have also investigated an alleged fraud scheme involving a Tennessee company and hundreds of thousands of catheters billed to Medicare, according to The Washington Post, citing anonymous sources.
Cochran said the Pain MD case felt especially “nefarious” because it used opioids to make patients play along.
“A scheme where you get Medicare or Medicaid money to provide a medically unnecessary treatment is always going to be out there,” Cochran said. “The opioid piece just gives you a universe of compliant people who are not going to question what you are doing.”
“It was only opioids that made those folks come back,” he said.
The allegations against Pain MD became public in 2018 when Cochran and the Department of Justice filed a civil lawsuit against the company, Kestner, and several associated clinics, alleging that Pain MD defrauded taxpayers and government insurance programs by billing for “tendon origin injections” that were “not actually injections into tendons at all.”
Kestner, Pain MD, and several associated clinics have each denied all allegations in that lawsuit, which is ongoing.Scott Kreiner, an expert on spine care and pain medicine who testified at Kestner’s criminal trial, said that true tendon origin injections (or TOIs) typically are used to treat inflamed joints, like the condition known as “tennis elbow,” by injecting steroids or platelet-rich plasma into a tendon. Kreiner said most patients need only one shot at a time, according to the transcript.
But Pain MD made repeated injections into patients’ backs that contained only lidocaine or Marcaine, which are anesthetic medications that cause numbness for mere hours, Kreiner testified. Pain MD also used needles that were often too short to reach back tendons, Kreiner said, and there was no imaging technology used to aim the needle anyway. Kreiner said he didn’t find any injections in Pain MD’s records that appeared medically necessary, and even if they had been, no one could need so many.
“I simply cannot fathom a scenario where the sheer quantity of TOIs that I observed in the patient records would ever be medically necessary,” Kreiner said, according to the trial transcript. “This is not even a close call.”
Jonathan White, a physician assistant who administered injections at Pain MD and trained other employees to do so, then later testified against Kestner as part of a plea deal, said at trial that he believed Pain MD’s injection technique was based on a “cadaveric investigation.”
According to the trial transcript, White said that while working at Pain MD he realized he could find no medical research that supported performing tendon origin injections on patients’ backs instead of their joints. When he asked if Pain MD had any such research, White said, an employee responded with a two-paragraph letter from a Tennessee anatomy professor — not a medical doctor — that said it was possible to reach the region of back tendons in a cadaver by injecting “within two fingerbreadths” of the spine. This process was “exactly the procedure” that was taught at Pain MD, White said.
During his own testimony, Kreiner said it was “potentially dangerous” to inject a patient as described in the letter, which should not have been used to justify medical care.
“This was done on a dead person,” Kreiner said, according to the trial transcript. “So the letter says nothing about how effective the treatment is.”
Over-Injecting ‘Killed My Hand’
Pain MD collapsed into bankruptcy in 2019, leaving some patients unable to get new prescriptions because their medical records were stuck in locked storage units, according to federal court records.
At the time, Pain MD defended the injections and its practice of discharging patients who declined the shots. When a former patient publicly accused the company of treating his back “like a dartboard,” Pain MD filed a defamation lawsuit, then dropped the suit about a month later.
“These are interventional clinics, so that’s what they offer,” Jay Bowen, a then-attorney for Pain MD, told The Tennessean newspaper in 2019. “If you don’t want to consider acupuncture, don’t go to an acupuncture clinic. If you don’t want to buy shoes, don’t go to a shoe store.”
Kestner’s trial told another story. According to the trial transcript, eight former Pain MD medical providers testified that the driving force behind Pain MD’s injections was Kestner himself, who is not a medical professional and yet regularly pressured employees to give more shots.
One nurse practitioner testified that she received emails “every single workday” pushing for more injections. Others said Kestner openly ranked employees by their injection rates, and implied that those who ranked low might be fired.
“He told me that if I had to feed my family based on my productivity, that they would starve,” testified Amanda Fryer, a nurse practitioner who was not charged with any crime.
Brian Richey, a former Pain MD nurse practitioner who at times led the company’s injection rankings, and has since taken a plea deal that required him to testify in court, said at the trial that he “performed so many injections” that his hand became chronically inflamed and required surgery.
“‘Over injecting killed my hand,’” Richey said on the witness stand, reading a text message he sent to another Pain MD employee in 2017, according to the trial transcript. “‘I was in so much pain Injecting people that didnt want it but took it to stay a patient.’”
“Why would they want to stay there?” a prosecutor asked.
“To keep getting their narcotics,” Richey responded, according to the trial transcript.
Throughout the trial, defense attorney Peter Strianse argued that Pain MD’s focus on injections was a result of Kestner’s “obsession” with ensuring that the company “would never be called a pill mill.”
Strianse said that Kestner “stayed up at night worrying” about patients coming to clinics only to get opioid prescriptions, so he pushed his employees to administer injections, too.
“Employers motivating employees is not a crime,” Strianse said at closing arguments, according to the court transcript. “We get pushed every day to perform. It’s not fraud; it’s a fact of life.”
Prosecutors insisted that this defense rang hollow. During the trial, former employees had testified that most patients’ opioid dosages remained steady or increased while at Pain MD, and that the clinics did not taper off the painkillers no matter how many injections were given.
“Giving them injections does not fix the pill mill problem,” federal prosecutor Katherine Payerle said during closing arguments, according to the trial transcript. “The way to fix being a pill mill is to stop giving the drugs or taper the drugs.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Dioscorea Villosa: Hormones, Arthritis, & Skin
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
On A Wild Yam Chase?
We recently came across a supplement blend that had wild yam extract as a minor ingredient. Our plucky (and usually very knowledgable) researcher had never heard of its use before, so she set about doing her thing. This is what she found…
What health claims are made?
Wild yam extract (Dioscorea villosa) is traditionally sold and used for:
- Balancing hormones
- Combating arthritis
- Anti-aging effects for the skin
Does it balance hormones?
First, as a quick catch-up, we’ll drop a previous article of ours for your convenience:
What Does “Balance Your Hormones” Even Mean?
We couldn’t find almost any studies into wild yam extract’s hormone-balancing effects, but we did find one study, and:
❝Symptom scores showed a minor effect of both placebo and active treatment on diurnal flushing number and severity and total non-flushing symptom scores, and on nocturnal sweating after placebo, but no statistical difference between placebo and active creams.
This study suggests that short-term treatment with topical wild yam extract in women suffering from menopausal symptoms is free of side-effects, but appears to have little effect on menopausal symptoms❞
…which is a very thorough, polite, sciencey way of saying “wow, this does so many different kinds of nothing”
On the one hand, this was a small study (n=23). On the other hand, it was also literally the only study we could find.
Does it combat arthritis?
Maybe! We again didn’t find much research into this but we did find two in vitro studies that suggests that diosgenin (which can be derived from wild yam extract) helps:
- Diosgenin inhibits IL-1β-induced expression of inflammatory mediators in human osteoarthritis chondrocytes
- Diosgenin, a plant steroid, induces apoptosis in human rheumatoid arthritis synoviocytes with cyclooxygenase-2 overexpression
And we also found a rodent study that found that wild yam extract specifically helped against “acetic acid-induced writhing and formalin-induced pain“, and put that down to anti-inflammatory properties:
So, none of these studies tell us much about whether it would be helpful for humans—with or without arthritis, and hopefully without “acetic acid-induced writhing and formalin-induced pain”.
However, they do suggest that it would be reasonable to test in humans next.
You might prefer:
- Tips For Avoiding/Managing Osteoarthritis
- Tips For Avoiding/Managing Rheumatoid Arthritis
- How to Prevent (or Reduce) Inflammation
Does it keep skin young?
Again, research is thin on the ground, but we did find some! A study with wild-yam-derived diosgenin found that it didn’t make anything worse, and otherwise performed a similar role to vitamin A:
Read: Novel effects of diosgenin on skin aging
That was on rats with breast cancer though, so its applicability to healthy humans may be tenuous (while in contrast, simply getting vitamin A instead is a known deal).
Summary
- Does it balance hormones? It probably does little to nothing in this regard
- Does it combat arthritis? It probably has anti-inflammatory effects, but we know of no studies in humans. There are much more well-established anti-inflammatories out there.
- Does it keep the skin young? We know that it performs a role similar to vitamin A for rats with breast cancer, and didn’t make anything worse for them. That’s the extent of what we know.
Where can I get some?
In the unlikely event that the above research review has inspired you with an urge to buy wild yam extract, here is an example product for your convenience.
Some final words…
If you are surprised that we’re really not making any effort to persuade you of its merits, please know that (outside of the clearly-marked sponsor section, which helps us keep the lights on, so please do visit those) we have no interest in selling you anything. We’re genuinely just here to inform 🙂
If you are wondering why we ran this article at all if the supplement has negligible merits, it’s because science is science, knowledge is knowledge, and knowing that something has negligible merit can be good knowledge to have!
Also, running articles like this from time to time helps you to know that when we do sing the praises of something, it’s with good reason
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: