Tips For Avoiding/Managing Rheumatoid Arthritis
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Avoiding/Managing Rheumatoid Arthritis
Arthritis is the umbrella term for a cluster of joint diseases involving inflammation of the joints, hence “arthr-” (joint) “-itis” (suffix used to denote inflammation). These are mostly, but not all, autoimmune diseases, in which the body’s immune system mistakenly attacks our own joints.
Inflammatory vs Non-Inflammatory Arthritis
Arthritis is broadly divided into inflammatory arthritis and non-inflammatory arthritis.
You may be wondering: how does one get non-inflammatory inflammation of the joints?
The answer is, in “non-inflammatory” arthritis, such as osteoarthritis, the damage comes first (by general wear-and-tear) and inflammation generally follows as part of the symptoms, rather than the cause. So the name can be a little confusing. In the case of osteo- and other “non-inflammatory” forms of arthritis, you definitely still want to keep your inflammation at bay as best you can, but it’s not as absolutely critical a deal as it is for “inflammatory” forms of arthritis.
We’ll tackle the beast that is osteoarthritis another day, however.
Today we’re going to focus on…
Rheumatoid Arthritis
This is the most common of the autoimmune forms of arthritis. Some quick facts:
- It affects a little under 1% of the global population, but the older we get, the more likely it becomes
- Early onset of rheumatoid arthritis is most likely to show up around the age of 50 (but it can show up at any age)
- However, incidence (not onset) of rheumatoid arthritis peaks in the 70s age bracket
- It is 2–4 times more common in women than in men
- Approximately one third of people stop work within two years of its onset, and this increases thereafter.
Well, that sounds gloomy.
Indeed it’s not fun. There’s a lot of stiffness and aching of joints (often with swelling too), loss of joint function can be common, and then there are knock-on effects like fatigue, weakness, and loss of appetite.
Beyond that it’s an autoimmune disorder, its cause is not known, and there is no known cure.
Is there any good news?
If you don’t have rheumatoid arthritis at the present time, you can reduce your risk factors in several ways:
- Having an anti-inflammatory diet. Get plenty of fiber, greens, and berries. Fatty fish is great too, as are oily nuts. On the other side of things, high consumption of salt, sugar, alcohol, and red meat are associated with a greater risk of developing rheumatoid arthritis.
- Not smoking. Smoking is bad for pretty much everything, including your chances of developing rheumatoid arthritis.
- Not being obese. This one may be more a matter of correlation than causation, because of the dietary factors (if one eats an anti-inflammatory diet, obesity is less likely), but the association is there.
There are other risk factors that are harder to control, such as genetics, age, sex, and having a mother who smoked.
See: Genetic and environmental risk factors for rheumatoid arthritis
What if I already have rheumatoid arthritis?
If you already have rheumatoid arthritis, it becomes a matter of symptom management.
First, reduce inflammation any (reasonable) way you can. We did a main feature on this before, so we’ll just drop that again here:
Next, consider the available medications. Your doctor may or may not have discussed all of the options with you, so be aware that there are more things available than just pain relief. To talk about them all would require a whole main feature, so instead, here’s a really well-compiled list, along with explanations about each of them, up to date as of this year:
Rheumatoid Arthritis Medication List (And What They Do, And How)
Finally, consider other lifestyle adjustments to manage your symptoms. These include:
- Exercise—gently, though! You do not want to provoke a flare-up, but you do want to maintain your mobility as best you can. There’s a use-it-or-lose-it factor here. Swimming and yoga are great options, as is tai chi. You may want to avoid exercises that involve repetitive impacts to your joints, like running.
- Rest—while keeping mobility going. Get good sleep at night (this is important), but don’t make your bed your new home, or your mobility will quickly deteriorate.
- Hot & cold—both can help, and alternating them can reduce inflammation and stiffness by improving your body’s ability to respond appropriately to these stimuli rather than getting stuck in an inappropriate-response state of inflammation.
- Mobility aids—if it helps, it helps. Maybe you only need something during a flare-up, but when that’s the case, you want to be as gentle on your body as possible while keeping moving, so if crutches, handrails etc help, then by all means get them and use them.
- Go easy on the use of braces, splints, etc—these can offer short-term relief, but at a long term cost of loss of mobility. Only you can decide where to draw the line when it comes to that trade-off.
You can also check out our previous article:
Managing Chronic Pain (Realistically!)
Take good care of yourself!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Aspirin, CVD Risk, & Potential Counter-Risks

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Aspirin Pros & Cons

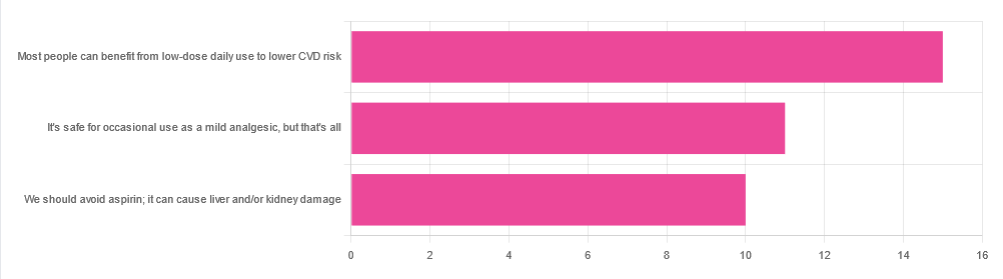
In Tuesday’s newsletter, we asked your health-related opinion of aspirin, and got the above-depicted, below-described set of responses:
- About 42% said “Most people can benefit from low-dose daily use to lower CVD risk”
- About 31% said “It’s safe for occasional use as a mild analgesic, but that’s all”
- About 28% said “We should avoid aspirin; it can cause liver and/or kidney damage”
So, what does the science say?
Most people can benefit from low-dose daily aspirin use to lower the risk of cardiovascular disease: True or False?
True or False depending on what we mean by “benefit from”. You see, it works by inhibiting platelet function, which means it simultaneously:
- decreases the risk of atherothrombosis
- increases the risk of bleeding, especially in the gastrointestinal tract
When it comes to balancing these things and deciding whether the benefit merits the risk, you might be asking yourself: “which am I most likely to die from?” and the answer is: neither
While aspirin is associated with a significant improvement in cardiovascular disease outcomes in total, it is not significantly associated with reductions in cardiovascular disease mortality or all-cause mortality.
In other words: speaking in statistical generalizations of course, it may improve your recovery from minor cardiac events but is unlikely to help against fatal ones
The current prevailing professional (amongst cardiologists) consensus is that it may be recommended for secondary prevention of ASCVD (i.e. if you have a history of CVD), but not for primary prevention (i.e. if you have no history of CVD). Note: this means personal history, not family history.
In the words of the Journal of the American College of Cardiology:
❝Low-dose aspirin (75-100 mg orally daily) might be considered for the primary prevention of ASCVD among select adults 40 to 70 years of age who are at higher ASCVD risk but not at increased bleeding risk (S4.6-1–S4.6-8).
Low-dose aspirin (75-100 mg orally daily) should not be administered on a routine basis for the primary prevention of ASCVD among adults >70 years of age (S4.6-9).
Low-dose aspirin (75-100 mg orally daily) should not be administered for the primary prevention of ASCVD among adults of any age who are at increased risk of bleeding (S4.6-10).❞
~ Dr. Donna Arnett et al. (those section references are where you can find this information in the document)
Read in full: Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology
Or if you’d prefer a more pop-science presentation:
Many older adults still use aspirin for CVD prevention, contrary to clinical guidance
Aspirin can cause liver and/or kidney damage: True or False?
True, but that doesn’t mean we must necessarily abstain, so much as exercise caution.
Aspirin is (at recommended doses) not usually hepatotoxic (toxic to the liver), but there is a strong association between aspirin use in children and the development of Reye’s syndrome, a disease involving encephalopathy and a fatty liver. For this reason, most places have an official recommendation that aspirin not be used by children (cut-off age varies from place to place, for example 12 in the US and 16 in the UK, but the key idea is: it’s potentially dangerous for those who are not fully grown).
Aspirin is well-established as nephrotoxic (toxic to the kidneys), however, the toxicity is sufficiently low that this is not expected to be a problem to otherwise healthy adults taking it at no more than the recommended dose.
For numbers, symptoms, and treatment, see this very clear and helpful resource:
An evidence based flowchart to guide the management of acute salicylate (aspirin) overdose
Take care!
Share This Post
-

Can “Light Activity” Really Help Against Osteoporosis?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It is well-known, at least amongst health-conscious people of a certain age, that exercise plays a role in the prevention of osteoporosis.
Furthermore, it’s generally considered that resistance training is the most beneficial, as putting weight on bones forces them to become stronger. This may seem like a dangerous endeavor, akin to “putting stress on this teacup will force it to become stronger”, which clearly has a false logic to it, but the fact is that (contrary to popular belief that they are a sort of inorganic mineral scaffold) our bones are a living, ever-changing part of our body. Yes, there’s a lot of inorganic mineral mass in there, but there are a lot of living cells too, and those cells are continuously breaking down our bones and rebuilding, bit by tiny bit.
So, exercise—and the stress that exercise puts on our bones—is part of what tells those cells how to go about doing their jobs.
For more about this process, see: Which Osteoporosis Medication, If Any, Is Right For You? ← this is because some of the meds work by slowing down the cells that break down cells, and other meds work by accelerating the bone-building process
And as for resistance training, see: Resistance Is Useful! (Especially As We Get Older)
But won’t exercise increase the risk of breaking already-weakened bones?
Yes, yes it will. Which creates a very unfortunate catch-22:
- don’t exercise and your bones will deteriorate more rapidly, which wouldn’t happen if you maintained them with exercise
- do exercise and you might fracture something while exercising, which wouldn’t have happened relaxing on your couch
However, this risk can be mitigated somewhat by being judicious about our choice of exercise. The trick is to engage in exercise that will involve resistance (and thus moderate physical stress, cueing the bones to get stronger), but won’t involve the kinds of movements that are most likely to result in a fracture (which include but are not limited to: heavy impacts and rapid changes of direction).
For more on this, see: Osteoporosis & Exercises: Which To Do (And Which To Avoid)
So, how about walking and other “light exercise”?
We’ll first mention some now-older research (published January 2024), that we wrote about back when it was new, and that yes, walking does help. The study by Dr. Tiina Savikangas et al. looked at 299 people in their 70s (just over half being women) and found that, over the course of a year, bone mineral density loss was inversely correlated with moderate exercise as recorded by an accelerometer (as found in most fitness-tracking wearables and smartphones).
In other words: those who got more minutes of exercise, kept more bone mineral density.
You can read more about that here: One More Resource Against Osteoporosis!
Now, that was about moderate exercise, as measured by an accelerometer (i.e. the participants each wore a smartwatch or similar accelerometer-based fitness tracker).
More recently, a new research review by the International Osteoporosis Foundation Rehabilitation Working Group looked at a huge amount of data from many studies, and found:
- Physical activity—especially weight-bearing and resistance training—improves bone mineral density and helps reduce fracture risk in both younger and older populations.
- Sedentary behavior—independent of overall activity levels—has harmful effects on bone health, increasing fracture risk, particularly in frail or pre-frail individuals.
- Light-intensity activity can yield measurable benefits when it replaces sedentary time, especially in older adults and postmenopausal women.
- Early and continuous promotion of physical activity, aligned with World Health Organization (WHO) guidelines, provides an effective strategy for maintaining skeletal health and preventing osteoporotic fractures.
You can find the paper itself here: The Impact of Sedentary Behavior and Physical Activity on Bone Health: A Narrative Review from the Rehabilitation Working Group of the International Osteoporosis Foundation
That second item is perhaps the most relevant to take into account, because it shows that while light activity will not yield the same results as moderate weight-bearing or resistance training exercise, it’s a world better than sedentary behavior, because sedentary behavior essentially tells your bones “we don’t need you”, and in many cases, especially resource-intensive biological processes (as bone turnover is), the body will not use valuable resources to maintain something that doesn’t seem to be needed.
So, it’s less about the light activity for its own sake, and more about not being sedentary.
You may be wondering: does this distinction matter? And the answer is, it might do; it depends on your lifestyle. For example, your writer here sits down for a total of about 1 hour per day (and lies in bed for about 8 hours, of which, about 7.5 hours sleeping). However, that does not mean that the remaining 15 hours per day are spent actively exercising. Indeed, a good many of the remaining hours are spent standing at my desk. Which is not enough to stress my bones even moderately, but is enough that my body is aware of the need to maintain a structure capable of maintaining a whole-body upright posture, and thus, my bones are maintained more than they would if I spent the same time sitting.
See also: Stand Up For Your Health (Or Don’t) ← this is about reducing the damage done by sitting, including if for whatever reason you have to spend a lot of time sitting, including if you physically cannot stand and/or cannot walk.
You can also build in not just “movement breaks”, but also active exercise in small, manageable chunks that add to to disproportionate benefits: How Useful Is “Exercise Snacking”, Really?
Want to learn more?
Here’s an excellent book we reviewed a little while back:
Yoga for Osteoporosis – by Dr. Loren Fishman ← the title makes it seem like any one of a thousand other “gentle exercise” books, but actually this one has an incredible wealth of science, clear explanations, and there’s far more going on in here than one could ever reasonably expect of book with this title, so if this topic (avoiding/reversing osteoporosis) is at all relevant to you personally, we very strongly recommend this specific book.
Take care!
Share This Post
-
Red Cabbage vs Spinach – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing red cabbage to spinach, we picked the spinach.
Why?
We recently compared [white] cabbage to spinach, and spinach won, so it was interesting to see whether it being red cabbage would tip the scales. It didn’t.
In terms of macros, these are once again very similar: mostly water, small amounts of carbs and protein, and enough fiber to hold them together. Nominally, red cabbage has very slightly more carbs and spinach has very slightly more protein, but the numbers are so low in both cases as to render this category still a tie in our regard, for all practical purposes. A purist argument could be made to call it a win for spinach, though.
In the category of vitamins, it’s only slightly less imbalanced than it was for white cabbage vs spinach; red cabbage has more of vitamins B5, B5, and C, while spinach has more of vitamins A, B1, B2, B3, B7, B9, E, K, and choline; a clear win for spinach.
When it comes to minerals, cabbage is once again not higher in any minerals, and spinach has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Another easy win for spinach.
With regard to phytochemicals, red cabbage fared better than white cabbage did, but spinach still has a much higher polyphenol content (mostly flavonols), and on the flipside, spinach has a much higher oxalate content (that’s not a problem for most people, but bad if you have certain kidney issues). So this category could be swung any which way depending on the state of your kidneys. For simplicity, we’ll record this round as a tie, but its constituent parts are worth bearing in mind.
Adding up the sections makes for an overall win for spinach, but by all means enjoy either or both; diversity is good, and cabbage of any kind is always a nutritional powerhouse; it just looks bad standing next to spinach!
Want to learn more?
You might like:
21 Most Beneficial Polyphenols & What Foods Have Them
Enjoy!
Share This Post
Related Posts
-
Doctor Explains: 15 Signs Of Hypothyroidism
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Siobhan Deshauer explains the signs (and in some cases, symptoms) that can point to this oft-underdiagnosed condition:
Watch out for these
We’ll not keep them a secret, the signs/symptoms are…
- Goiter: enlarged thyroid gland, visible in the neck and may cause difficulty swallowing or breathing.
- Dry skin: due to reduced production of skin oils, leading to rough, cracked skin.
- Asteatotic eczema: cracked, mosaic-like dry skin often called “crazy paving.”
- Palmoplantar keratoderma: thickening and buildup of skin on hands and feet due to improper shedding.
- Hair thinning: hair becomes dull, brittle, and sheds excessively, including scalp, eyebrows, and body hair.
- Brittle or thickened nails: poor quality nail growth, vertical ridges, and nails prone to splitting or lifting.
- Queen Anne’s sign: loss of the outer third of the eyebrows.
- Myxedema: swelling, especially around the eyes, hands, and feet, caused by buildup of gelatinous material in the skin.
- Obstructive sleep apnea: enlarged tongue due to myxedema can block the airway during sleep.
- Carpal tunnel syndrome: swelling compresses the median nerve, causing numbness and tingling in the hands.
- Facial palsy: rare nerve compression causing one-sided facial droop.
- Cold intolerance: feeling unusually cold due to slowed metabolism.
- Myxedema coma: a severe, life-threatening form of hypothyroidism causing confusion, low body temperature, and organ shutdown. This may seem a strange (and rather severe) one to sandwich in between “feeling a bit cold” and “skin discoloration”, but we’re just reporting on what’s in the video!
- Carotenemia: yellow-orange discoloration of the skin, especially palms and soles, due to impaired conversion of beta-carotene.
- Depression: reduced neurotransmitters like serotonin and dopamine, leading to mood changes and mental fog.
- Menstrual changes: heavier, longer, or irregular periods caused by hormonal imbalance.
- Chronic fatigue: constant tiredness and low energy.
- Constipation: slowed digestion due to decreased metabolism.
- Unexplained weight gain: often mild to moderate, caused by a slower metabolic rate.
For more on each of these plus visual illustrations where appropriate, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Three Rs To Boost Thyroid-Related Energy Levels
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Mind Over Mood – by Dr. Dennis Greenberger & Dr. Christine Padesky
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes we’ve reviewed books about mental health, and said something to the effect of “however, no, it’s not just a book about CBT”. Well, this one is!
Cognitive Behavioral Therapy (CBT) is a very useful tool—or rather, set of tools—for managing one’s own mental health. It’s not a cure-all and it has its limitations, but it’s also the industry gold standard for a reason (the reason is: it has a huge evidence-base for actually working).
Its strengths are: managing mood disturbances that are related to automatic negative thoughts/beliefs, by applying the tools to see through the illusions presented by depression, anxiety, anger, shame, etc.
This book is an introduction to CBT, guide to applying CBT in your life, and a workbook for then actually doing so. To this end, you’ll get the most out of the book if you do actually do the exercises.
The style is comprehensive, with a lot of lengthy examples that were a little lengthy for this reviewer’s personal preferences, but the result is arguably a deeper dive into the potential applications for CBT than we might have got if the examples had been a few lines each for simplicity.
Bottom line: if you’re comfortable that you already know how to use CBT to manage your moods, then you can skip this book. But if you’d like an “everything in one” explainer/guide/workbook, then this one is certainly worthy of consideration.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Getting antivirals for COVID too often depends on where you live and how wealthy you are
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Medical experts recommend antivirals for people aged 70 and older who get COVID, and for other groups at risk of severe illness and hospitalisation from COVID.
But many older Australians have missed out on antivirals after getting sick with COVID. It is yet another way the health system is failing the most vulnerable.
CGN089/Shutterstock Who missed out?
We analysed COVID antiviral uptake between March 2022 and September 2023. We found some groups were more likely to miss out on antivirals including Indigenous people, people from disadvantaged areas, and people from culturally and linguistically diverse backgrounds.
Some of the differences will be due to different rates of infection. But across this 18-month period, many older Australians were infected at least once, and rates of infection were higher in some disadvantaged communities.
How stark are the differences?
Compared to the national average, Indigenous Australians were nearly 25% less likely to get antivirals, older people living in disadvantaged areas were 20% less likely to get them, and people with a culturally or linguistically diverse background were 13% less likely to get a script.
People in remote areas were 37% less likely to get antivirals than people living in major cities. People in outer regional areas were 25% less likely.
Dispensing rates by group. Grattan Institute Even within the same city, the differences are stark. In Sydney, people older than 70 in the affluent eastern suburbs (including Vaucluse, Point Piper and Bondi) were nearly twice as likely to have had an antiviral as those in Fairfield, in Sydney’s south-west.
Older people in leafy inner-eastern Melbourne (including Canterbury, Hawthorn and Kew) were 1.8 times more likely to have had an antiviral as those in Brimbank (which includes Sunshine) in the city’s west.
Why are people missing out?
COVID antivirals should be taken when symptoms first appear. While awareness of COVID antivirals is generally strong, people often don’t realise they would benefit from the medication. They wait until symptoms get worse and it is too late.
Frequent GP visits make a big difference. Our analysis found people 70 and older who see a GP more frequently were much more likely to be dispensed a COVID antiviral.
Regular visits give an opportunity for preventive care and patient education. For example, GPs can provide high-risk patients with “COVID treatment plans” as a reminder to get tested and seek treatment as soon as they are unwell.
Difficulty seeing a GP could help explain low antiviral use in rural areas. Compared to people in major cities, people in small rural towns have about 35% fewer GPs, see their GP about half as often, and are 30% more likely to report waiting too long for an appointment.
Just like for vaccination, a GP’s focus on antivirals probably matters, as does providing care that is accessible to people from different cultural backgrounds.
Care should go those who need it
Since the period we looked at, evidence has emerged that raises doubts about how effective antivirals are, particularly for people at lower risk of severe illness. That means getting vaccinated is more important than getting antivirals.
But all Australians who are eligible for antivirals should have the same chance of getting them.
These drugs have cost more than A$1.7 billion, with the vast majority of that money coming from the federal government. While dispensing rates have fallen, more than 30,000 packs of COVID antivirals were dispensed in August, costing about $35 million.
Such a huge investment shouldn’t be leaving so many people behind. Getting treatment shouldn’t depend on your income, cultural background or where you live. Instead, care should go to those who need it the most.
Getting antivirals shouldn’t depend on who your GP is. National Cancer Institute/Unsplash People born overseas have been 40% more likely to die from COVID than those born here. Indigenous Australians have been 60% more likely to die from COVID than non-Indigenous people. And the most disadvantaged people have been 2.8 times more likely to die from COVID than those in the wealthiest areas.
All those at-risk groups have been more likely to miss out on antivirals.
It’s not just a problem with antivirals. The same groups are also disproportionately missing out on COVID vaccination, compounding their risk of severe illness. The pattern is repeated for other important preventive health care, such as cancer screening.
A 3-step plan to meet patients’ needs
The federal government should do three things to close these gaps in preventive care.
First, the government should make Primary Health Networks (PHNs) responsible for reducing them. PHNs, the regional bodies responsible for improving primary care, should share data with GPs and step in to boost uptake in communities that are missing out.
Second, the government should extend its MyMedicare reforms. MyMedicare gives general practices flexible funding to care for patients who live in residential aged care or who visit hospital frequently. That approach should be expanded to all patients, with more funding for poorer and sicker patients. That will give GP clinics time to advise patients about preventive health, including COVID vaccines and antivirals, before they get sick.
Third, team-based pharmacist prescribing should be introduced. Then pharmacists could quickly dispense antivirals for patients if they have a prior agreement with the patient’s GP. It’s an approach that would also work for medications for chronic diseases, such as cardiovascular disease.
COVID antivirals, unlike vaccines, have been keeping up with new variants without the need for updates. If a new and more harmful variant emerges, or when a new pandemic hits, governments should have these systems in place to make sure everyone who needs treatment can get it fast.
In the meantime, fairer access to care will help close the big and persistent gaps in health between different groups of Australians.
Peter Breadon, Program Director, Health and Aged Care, Grattan Institute
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: