

Lower Your Cortisol! (Here’s Why & How)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cortisol, or “the stress hormone” to its friends, is produced by your adrenal glands, and is generally considered “not fun”.
It does serve a purpose, of course, just like almost everything else our body does. It serves as part of the “fight or flight” response, for example, and helps you to wake up in the morning.
While you do need some cortisol (and a small percentage of people have too little), most of us have too much.
Why? Simply put, modern life is not what 200,000* years of human evolution prepared us for:
- Agriculture (which allowed us to settle down and cease being nomadic) happened during the last 6% of those 200,000 years.
- The Industrial Revolution and the onset of modern capitalism happened during only during the last 0.1% of those 200,000 years.
*the 200,000 years figure is conservative and doesn’t take into account the 200,000,000 years of pre-hominid mammalian evolution. Doing so, on the basis of the mammalian brain & physiology being what’s important here, means our modern stressors have been around for <0.0001% of the time we have.
So guess what, our bodies haven’t caught up. As far as our bodies are concerned, we are supposed to be enjoying the sunshine of grassy plains and the shade of woodland while eating fruit.
- When the alarm clock goes off, our body panics and prepares us to either flee or help fight the predator, because why else would we have been woken so?
- When we have a pressing deadline for work, our brain processes this as “if we don’t do this, we will literally starve and die”.
- When people are upset or angry with us, there’s a part of our brain that fears exile from the tribe and resultant death.
…and so on.
Health Risks of High Cortisol
The long-term stressors are the biggest issue for health. Unless you have a heart condition or other relevant health problem, almost anyone can weather a brief unpleasant surprise. But if something persists? That prompts the body to try to protect you, bless it. The body’s attempts backfire, because…
- One way it does this by making sure to save as much food as possible in the form of body fat
- It’ll also increase your appetite, to make sure you eat anything you can while you still can
- It additionally tries to protect you by keeping you on the brink of fight-or-flight readiness, e.g:
- High blood pressure
- High blood sugar levels
- Rapid mood changes—gotta be able to do those heel-turns as necessary and react quickly to any possible threat!
Suffice it to say, these things are not good for your long-term health.
That’s the “Why”—now here’s the “How”:
Lowering your cortisol levels mostly means lowering your stress and/or lowering your stress response. We previously gave some powerful tools for lowering anxiety, which for these purposes amounts to the same thing.
However, we can also make nutritional and lifestyle changes that will reduce our cortisol levels, for example:
- Reduce (ideally: eliminate from your lifestyle) caffeine
- Reduce (ideally: eliminate from your lifestyle) alcohol
- Yes, really. While many understandably turn to alcohol specifically to help manage stress, it only makes it worse long-term.
- Additionally, alcohol directly stimulates cortisol production, counterintuitive as that may be.
Read: Alcohol, Aging, and the Stress Response ← full article (with 37 sources of its own) from the NYMC covering how alcohol stimulates cortisol production and what that means for us
As well as reductions/eliminations, are some things you can add into your lifestyle that will help!
We’ve written previously about some:
Read: Ashwagandha / Read: L-Theanine / Read: CBD Oil
Other things include, no surprises here:
- The Mediterranean diet (nutritious and delicious): https://10almonds.com/mediterranean-diet
- Get 7–9 hours (good quality!) sleep per night: https://10almonds.com/time-pillow-talk
- Get regular exercise (the regularity matters most!): https://10almonds.com/keep-on-keeping-on
Progressive Relaxation
We’ll give this one its own section because we’ve not talked about it before. Maybe you’re familiar. If not, then in a nutshell: progressive relaxation means progressively tensing and then relaxing each part of your body in turn.
Why does this work? Part of it is just a physical trick involving biofeedback and the natural function of muscles to contract and relax in turn, but the other part is even cleverer:
It basically tricks the most primitive part of your brain, the limbic system, into thinking you had a fight and won, telling it “thank you very much for the cortisol but we don’t need it anymore”.
Take a Hike! Or a Stroll… You Do You!
Last but not least: go connect with your roots. Spend time in the park, or at least the garden. Have a picnic, if the weather suits. Go somewhere you can spend time around leafy green things under a blue sky (we realize the blue sky may be subject to availability in some locations, but do what you can!).
Remember also: just as your body’s responses will be tricked by the alarm clock or the housework, they will also be easily tricked by blue and green stuff around you. If a sunny garden isn’t available in your location, a picture of one as your desktop background is the next best thing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Breast Milk’s Benefits That Are (So Far) Not Replicable

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Simply The Breast 🎶

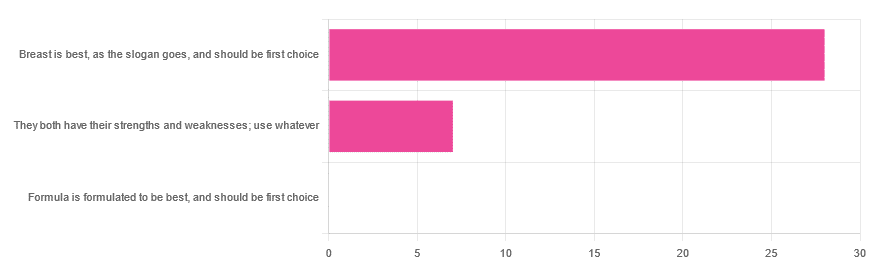
In Wednesday’s newsletter, we asked you for your opinion on breast vs formula milk (for babies!), and got the above-depicted, below-described, set of responses:
- 80% said “Breast is best, as the slogan goes, and should be first choice”
- 20% said “They both have their strengths and weaknesses; use whatever”
- 0% said “Formula is formulated to be best, and should be first choice”
That’s the first time we’ve ever had a possible poll option come back with zero votes whatsoever! It seems this topic is relatively uncontentious amongst our readership, so we’ll keep things brief today, but there is still a little mythbusting to be done.
So, what does the science say?
[Breast milk should be the first choice] at least for the few few weeks and months for the benefit of baby’s health as breast milk has protective factors formula does not: True or False?
True! The wording here was taken from one of our readers’ responses, by the way (thank you, Robin). There are a good number of those protective factors, the most well-known of which is passing on immune cells and cell-like things; in other words, immune-related information being passed from parent* to child.
*usually the mother, though in principle it could be someone else and in practice sometimes it is; the only real requirements are that the other person be healthy, lactating, and willing.
As for immune benefits, see for example:
Perspectives on Immunoglobulins in Colostrum and Milk
And for that matter, also:
(Colostrum is simply the milk that is produced for a short period after giving birth; the composition of milk will tend to change later)
In any case, immunoglobulin A is a very important component in breast milk (colostrum and later), as well as lactoferrin (has an important antimicrobial effect and is good for the newborn’s gut), and a plethora of cytokines:
As for that about the gut, lactoferrin isn’t the only breast milk component that benefits this, by far, and there’s a lot that can’t be replicated yet:
Human Breast Milk and the Gastrointestinal Innate Immune System
As long as your infant/child is nutritiously fed, it shouldn’t matter if it comes from breast or formula: True or False?
False! Formula milk will not convey those immune benefits.
This doesn’t mean that formula-feeding is neglectful; as several people who commented mentioned*, there are many reasons a person may not be able to breastfeed, and they certainly should not be shamed for that.
*(including the reader whose words we borrowed for this True/False item; the words we quoted above were prefaced with: “Not everyone is able to breastfeed for many different reasons”)
But, while formula milk is a very good second choice, and absolutely a respectable choice if breast milk isn’t an option (or an acceptable option) for whatever reason, it still does not convey all the health benefits of breast milk—yet! The day may come when they’ll find a way to replicate the immune benefits, but today is not that day.
They both have their strengths and weaknesses: True or False?
True! But formula’s strengths are only in the category of convenience and sometimes necessity—formula conveys no health benefits that breast milk could not do better, if available.
For many babies, formula means they get to eat, when without it they would starve due to non-availability of breast milk. That’s a pretty important role!
Note also: this is a health science publication, not a philosophical publication, but we’d be remiss not to mention one thing; let’s bring it in under the umbrella of sociology:
The right to bodily autonomy continues to be the right to bodily autonomy even if somebody else wants/needs something from your body.
Therefore, while there are indeed many good reasons for not being able to breastfeed, or even just not being safely* able to breastfeed, it is at the very least this writer’s opinion that nobody should be pressed to give their reason for not breastfeeding; “no” is already a sufficient answer.
*Writer’s example re safety: when I was born, my mother was on such drugs that it would have been a very bad idea for her to breastfeed me. There are plenty of other possible reasons why it might be unsafe for someone one way or another, but “on drugs that have a clear ‘do not take while pregnant or nursing’ warning” is a relatively common one.
All that said, for those who are willing and safely able, the science is clear: breast is best.
Want to read more?
The World Health Organization has a wealth of information (including explanations of its recommendations of, where possible, exclusive breastfeeding for the first 6 months, ideally continuing some breastfeeding for the first 2 years), here:
World Health Organization | Breastfeeding
Take care!
Share This Post
-
Is there a right way to talk to your baby? A baby brain expert explains ‘parentese’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You might have seen those heartwarming and often funny viral videos where parents or carers engage in long “talks” with young babies about this and that – usually just fun chit chat of no great consequence.
They’re often very sweet, and it’s lovely to see the babies’ faces lighting up at the sound of their mother or carer’s voice, or seeming to talk back. In one, the baby appears to reply in an accent strikingly similar to their carer’s:
So, what’s going on when we chat like this to babies? And is it better to chat to them in the tone and pace we’d use when talking to other adults, or is it OK to talk in a slower, higher pitched, sing-song voice?
Here’s what the research shows so far.

2p2play/Shutterstock Talking to your baby matters
When you speak with your baby, they are exposed to a rich tapestry of sounds and movements. Can babies make sense of all this input?
Well, by the time they’re born babies are already highly experienced with their mother’s voice as well as other language sounds they’ve heard while in utero.
In fact, research shows newborns prefer listening to the language they heard in utero rather than an unfamiliar language.
They also prefer to hear the story their mother read aloud regularly in the final weeks of pregnancy, compared to a different story – regardless of who is reading it.
So, although newborns are yet to understand the meaning of these words, they are already tuned in to the importance of language.
Given the vast exposure that most young babies have with their parent’s voice, passively listening to mum or dad talking is likely to be comforting.
Time spent together in close physical contact with a highly familiar person producing familiar sounds creates a safe, secure space rich in learning opportunities.
Babies can learn a lot about conversational style from just listening to and watching the way their parent communicates.
In fact, babies mimic their parents’ gestures, which can help build their vocabulary over time. The social context influences language skills.
Time spent in close physical contact with a familiar person producing familiar sounds creates a safe learning space for baby. Photo by Josh Willink/Pexels What if I run out of things to say?
If you’re not a fan of monologuing to your baby, don’t worry. They’re not missing out.
In fact, constant exposure to long monologues by a parent is unlikely to provide the baby with a particularly supportive language environment for developing their understanding or production of words.
Adult language is extremely complex. It takes a lot of experience with language before a string of sounds like “Yourdadlikeschocolatemoltenlavacake” can be interpreted as individual words linked to people, objects, or concepts.
One of the most effective ways to support early word recognition and promote attention to the structure of language is for the adult to use a simplified way of speaking to the baby.
“Parentese” is characterised by the use of higher pitch sounds, elongated vowels, and a slower pace of speaking. Real words are presented in a sing-song, happy voice.
Parentese draws the baby’s attention to words, and highlights how information in speech chunks together. Babies have been found to prefer to listen to this style of speaking compared to standard speech.
Time spent talking together in face-to-face interactions best supports language development. Tomsickova Tatyana/Shutterstock Speaking ‘parentese’
Parentese is not the same thing as “baby talk”. Baby talk involves the use of nonsense words, and the modelling of incorrect speech sounds and grammar. A baby is not being supported to learn the word “water” if they are repeatedly presented with a nonsense label like “waa waa” for their drink.
One US study found that when parents were trained to use parentese with their infants at six and ten months, the infants showed an increase in babbling and said more words at 14 months, compared to infants of parents who did not receive this training.
Other research has shown consistent use of parentese in the early years can help build the complexity of children’s language skills at five years of age.
Learning to talk is not simply the product of hearing lots of words. In the first weeks of life, infants are already beginning to produce coos and murmurs that both parents and outside observers judge to be intentional vocalisations.
Try responding to these sounds by imitating them and then interpreting what your baby might be trying to say. This enables them to take a turn as a social partner in the conservation.
When even very young babies take turns in conversations with an adult, the quality of their vocalisations increases.
At the youngest ages, time spent talking together in face-to-face interactions best supports language development.
With age, babies become increasingly interested in the objects in their environment.
Try responding to your baby’s sounds by imitating them and interpreting what they might be trying to say. Halfpoint/Shutterstock So, what should I do?
An effective way to boost language learning from about nine months of age is to notice what’s captured your baby’s attention and talk about that.
Try labelling and describing what your baby is looking at, playing with, pointing at, or babbling towards.
Research by colleagues and I found encouraging parents to engage in 15 minutes of this kind of talk a day with their 11-month-olds for a month was effective in promoting vocabulary growth at 15 and 18 months.
Overall, a rich language environment is created by engaging with your baby in a wide range of activities – via games, songs, and reading aloud – not just having focused conversations.
Jane Herbert, Associate Professor in Developmental Psychology, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
3 bathroom items you shouldn’t really share, according to an expert
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Imagine you’re away from home but forgot to pack your towel, razor or toothbrush.
Should you use other people’s?
Here’s why it’s probably best not to make a habit of it.
Peng Liu/Unsplash Microbes can stay active for a while
Many disease-causing bacteria, viruses or fungi live on cloth, plastic and metal objects in your bathroom. These so-called pathogenic microbes can remain viable on these surfaces for extended periods. That is, they’re able to cause infection for days, months or years.
For example, the fungus Aspergillus can remain viable for more than a month on cloth and plastic. Some bacteria can survive on these surfaces for years. And many viruses can remain viable for hours to months on some materials such as ceramics, metals, cloth and plastics.
But what is the risk from particular items such as used towels, razors and toothbrushes?
Scientists haven’t run randomised controlled trials (the gold standard study design) to determine the risk. This would be when one group in a study is chosen at random to, say, shave their legs with someone’s used razor, and the infection rates of known pathogens compared with those randomised to a control group who didn’t.
But there are other studies that give us some clues.
Can I share towels? If you play footy, maybe not
Less robust studies suggest an increased risk of picking up a skin infection from used towels.
One report from the United States was of an outbreak of antibiotic resistant Staphylococcus aureas (or Staph, for short) in a group of high-school football players. Players who shared a towel were eight times more likely to pick up an infection.
Staph can cause the skin condition impetigo. But in rare cases it can lead to life-threatening septic shock and organs failing.
In this case, the risk of transmitting Staph was probably elevated due to potential cuts and grazes from playing a contact sport.
Another study, also from the US, followed 150 households for 12 months. Each household had a single child infected with Staph.
When household members shared towels, the risk of Staph transmission increased significantly.
You might think that microbes are washed off in the shower. While washing with soap and water reduces the number of microbes on the skin it does not completely eliminate them. And the warm, moist conditions of the average bathroom encourage microbial growth.
Even if you don’t develop an infection, becoming colonised by pathogens (when there is no damage) can be problematic.
That’s because you may be exposed to antibiotic resistant species, increasing the risk of developing antibiotic resistant infections later. These are more time consuming and expensive to treat.
How about a toothbrush? Think of the viruses
Microbes can remain viable on hard objects, such as toothbrushes. And toothbrushes can cause gums to bleed. So sharing them is discouraged as this can transmit blood-borne viruses such as hepatitis C.
Not everyone who is in a risk category for hepatitis C infection has been tested. And people can be infectious without having symptoms.
Anything that has come into contact with saliva (such as your toothbrush) may also transmit pathogens. These include herpes simplex virus type 1 (HSV-1), which causes cold sores, and Epstein-Barr virus, which causes glandular fever.
A person with no signs of HSV-1 infection can still shed viruses and cause infection.
One review found toothbrushes were contaminated with potentially pathogenic species of bacteria such as Staph, E. coli and Pseudomonas. HSV-1 was also found in sufficient numbers to cause infection. This virus can remain viable for two to six days on plastic objects.
Surely a razor’s OK? Not if you hate warts
Microbes can remain viable on hard objects such as razors too. And it’s hard to avoid nicks when using a razor. So there’s a risk of transmitting blood-borne viruses if you share.
Razors, towels and other personal hygiene items can also spread human papillomaviruses that cause warts. So it’s no wonder dermatologists recommend each person has their own items.
Who’s at risk?
If you have cuts or grazes, this provides a portal of entry for microbes, putting you at increased risk of infection. Remember those footy players who shared towels.
Reduced immune function also increases the risk of infection. We see this in:
- babies, whose immune system is still developing
- elderly people, whose immune function declines in later life
- people taking immune suppressing medications, such as cancer drugs, oral corticosteroids and drugs taken after an organ transplant
- people with type 2 diabetes, because increased blood glucose levels damage the function of immune cells and associated molecules.
However, the overall risk of contracting an infection is low on any one occasion. And if you’re sharing a towel, razor or toothbrush with a partner, you’ll be in regular close contact and sharing microbes anyway.
But it’s still a good idea to avoid making a habit of sharing other people’s used bathroom items.
Thea van de Mortel, Professor Emerita, Nursing, School of Nursing and Midwifery, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post








Related Posts
-

In Plain English…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Time!
This is the bit whereby each week, we respond to subscriber questions/requests/etc
Have something you’d like to ask us, or ask us to look into? Hit reply to any of our emails, or use the feedback widget at the bottom, and a Real Human™ will be glad to read it!
Q: Love to have someone research all the additives in our medicines, (risk of birth control and breast cancer) and what goes in all of our food and beverages. So much info out there, but there are so many variations, you never know who to believe.
That’s a great idea! There are a lot of medicines and food and beverages out there, so that’s quite a broad brief, but! We could well do a breakdown of very common additives, and demystify them, sorting them into good/bad/neutral, e.g:
- Ascorbic acid—Good! This is Vitamin C
- Acetic acid—Neutral! This is vinegar
- Acetylsalicylic acid—Good or Bad! This is aspirin (a painkiller and blood-thinning agent, can be good for you or can cause more problems than it solves, depending on your personal medical situation. If in doubt, check with your doctor)
- Acesulfame K—Generally Neutral! This is a sweetener that the body can’t metabolize, so it’s also not a source of potassium (despite containing potassium) and will generally do nothing. Unless you have an allergy to it, which is rare but is a thing.
- Sucralose—Neutral! This is technically a sugar (as is anything ending in -ose), but the body can’t metabolize it and processes it as a dietary fiber instead. We’d list it as good for that reason, but honestly, we doubt you’re eating enough sucralose to make a noticeable difference to your daily fiber intake.
- Sucrose—Bad! This is just plain sugar
Sometimes words that sound the same can ring alarm bells when they need not, for example there’s a big difference between:
- Potassium iodide (a good source of potassium and iodine)
- Potassium cyanide (the famous poison; 300mg will kill you; half that dose will probably kill you)
- Cyanocobalamine (Vitamin B12)
Let us know if there are particular additives (or particular medications) you’d like us to look at!
While for legal reasons we cannot give medical advice, talking about common contraindications (e.g., it’s generally advised to not take this with that, as one will stop the other from working, etc) is definitely something we could do.
For example! St. John’s Wort, very popular as a herbal mood-brightener, is on the list of contraindications for so many medications, including:
- Antidepressants
- Birth control pills
- Cyclosporine, which prevents the body from rejecting transplanted organs
- Some heart medications, including digoxin and ivabradine
- Some HIV drugs, including indinavir and nevirapine
- Some cancer medications, including irinotecan and imatinib
- Warfarin, an anticoagulant (blood thinner)
- Certain statins, including simvastatin
Q: As I am a retired nurse, I am always interested in new medical technology and new ways of diagnosing. I have recently heard of using the eyes to diagnose Alzheimer’s. When I did some research I didn’t find too much. I am thinking the information may be too new or I wasn’t on the right sites.
(this is in response to last week’s piece on lutein, eyes, and brain health)
We’d readily bet that the diagnostic criteria has to do with recording low levels of lutein in the eye (discernible by a visual examination of macular pigment optical density), and relying on the correlation between this and incidence of Alzheimer’s, but we’ve not seen it as a hard diagnostic tool as yet either—we’ll do some digging and let you know what we find! In the meantime, we note that the Journal of Alzheimer’s Disease (which may be of interest to you, if you’re not already subscribed) is onto this:
See also:
- Journal of Alzheimer’s Disease (mixture of free and paid content)
- Journal of Alzheimer’s Disease Reports (open access—all content is free)
Q: As to specific health topics, I would love to see someone address all these Instagram ads targeted to women that claim “You only need to ‘balance your hormones’ to lose weight, get ripped, etc.” What does this mean? Which hormones are they all talking about? They all seem to be selling a workout program and/or supplements or something similar, as they are ads, after all. Is there any science behind this stuff or is it mostly hot air, as I suspect?
Thank you for asking this, as your question prompted yesterday’s main feature, What Does “Balancing Your Hormones” Even Mean?
That’s a great suggestion also about addressing ads (and goes for health-related things in general, not just hormonal stuff) and examining their claims, what they mean, how they work (if they work!), and what’s “technically true but may
be misleading* cause confusion”*We don’t want companies to sue us, of course.
Only, we’re going to need your help for this one, subscribers!
See, here at 10almonds we practice what we preach. We limit screen time, we focus on our work when working, and simply put, we don’t see as many ads as our thousands of subscribers do. Also, ads tend to be targeted to the individual, and often vary from country to country, so chances are good that we’re not seeing the same ads that you’re seeing.
So, how about we pull together as a bit of a 10almonds community project?
- Step 1: add our email address to your contacts list, if you haven’t already
- Step 2: When you see an ad you’re curious about, select “share” (there is usually an option to share ads, but if not, feel free to screenshot or such)
- Step 3: Send the ad to us by email
We’ll do the rest! Whenever we have enough ads to review, we’ll do a special on the topic.
We will categorically not be able to do this without you, so please do join in—Many thanks in advance!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
These Women Had Their Breasts Removed To Thwart Cancer. Then Came the Pain.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Three weeks after Sophia Bassan’s mastectomy, she felt a stabbing pain beneath her right armpit. In the following months, painful shocks radiated through her chest and back. Her body became so sensitive that at times she couldn’t wear a shirt or lift a fork to her mouth.
Bassan slept sitting up because it hurt to lie down, and she would flinch at the slightest touch.
“I remember thinking I was losing my mind,” said Bassan, 43. “One time I was in so much pain that I had to take off my top, and then my cat’s tail brushed against my back. I screamed.”
Mastectomies are lifesaving surgeries that remove a patient’s breasts to treat breast cancer, which affects 1 in 8 American women over their lifetimes, according to the American Cancer Society. Some women also undergo mastectomies as a preventive measure after a genetic test shows they have an increased risk for breast cancer.
In the months following surgery, many women are afflicted by post-mastectomy pain syndrome, or PMPS, which spans from uncomfortable to disabling and can last years.
Yet PMPS is inconsistently diagnosed and treated, leaving women like Bassan in agony as they hunt for relief and struggle to find doctors who take their pain seriously, according to a KFF Health News review of peer-reviewed research studies and interviews with pain specialists, surgeons, patients, and patient advocates.
Another problem is that PMPS is poorly defined, which contributes to the wide range of estimates for how common it is, reaching as high as more than 50% of mastectomy patients, according to studies. Even the low-end estimates, around 10%, would amount to tens of thousands of women.
PMPS care could improve if lawmakers pass the Advancing Women’s Health Coverage Act, which was introduced in October to ensure insurance coverage after breast cancer treatment, including preventive mastectomies. The bill, which does not mention PMPS by name, covers complications including chronic pain. More research would help, but pain research has long been fractured across several medical specialties and, more recently, has been undermined by the administration of President Donald Trump, who last year proposed deep cuts to research funding at the National Institutes of Health. After Congress rejected those cuts earlier this year, the White House slowed the release of NIH grant money, hindering ongoing and future scientific research.
“I’ve known women who’ve had chronic pain — itching, burning, stabbing pain — for years after mastectomies,” said Kathy Steligo, an author of multiple books on breast cancer who said she has spoken with hundreds of patients. “Of all the problems, that is probably the one least talked about by surgeons.”
Four mastectomy patients interviewed by KFF Health News told similar stories. In separate interviews, patients said their presurgery consultations did not raise the possibility of post-mastectomy pain syndrome, although each said they had signed forms that may have disclosed the chance of this complication. All said that they felt blindsided by the chronic pain, and some said their doctors dismissed their symptoms.
“Women don’t know about this, and when they have complications, the doctors act like it is so rare, like they’re so baffled,” Bassan said. “But this is statistically predictable.”
Jennifer Drubin Clark, 42, struggled with pain after her mastectomy in 2018, and it worsened after reconstructive breast surgery in 2019.
But her surgeon seemed to focus only on the appearance of her breast implants, she said.
“I couldn’t play the piano. I wanted to blow-dry my hair, but I couldn’t hold my arm above my head for more than two seconds. I couldn’t hold my kids,” Clark said. “Everything made me cry.”
After a mastectomy, Sophia Bassan developed painful shocks that radiated through her chest and back. She is one of thousands of women afflicted by post-mastectomy pain syndrome, or PMPS. (Amy Maxmen/KFF Health News) Pain Often Dismissed
Breast cancer survival rates have steadily increased since the 1980s thanks to improved cancer screening, genetic testing, better treatments, and a rise in mastectomy surgeries.
Post-mastectomy pain syndrome is a consequence of that success, according to recent research papers from anesthesiologists at Baylor University in Texas and surgeons in Chicago and New York. Both papers called for an increased focus on PMPS so that breast cancer patients can not only live longer but live well.
“In the past, when concern was predominantly on patient survival, this pain was often considered acceptable,” plastic surgeons Jonathan Bank and Maureen Beederman wrote in a 2021 paper, adding that mastectomies and other breast surgeries “should be considered truly successful only if patients are pain-free.”
Treatment for post-mastectomy pain has a long way to go, said anesthesiologist Sean Mackey, who leads the pain medicine division at Stanford University. Mackey said this “undertreated” condition has no consistent definition for diagnosis, no standardized screening, and no treatment approved by the Food and Drug Administration.
Even the name is a misnomer, Mackey said, since the same pain can arise among women who’ve had other procedures, including lumpectomies and lymph node surgeries.
“The condition was historically dismissed,” Mackey said. “Basically women were told: ‘You’re lucky to be alive. Some pain is expected. Suck it up and deal with it.’”
“That attitude has been slow to change,” he said.
With no clear treatment for PMPS, Bassan and others have experimented with options such as nerve stimulation machines. “Doctors act like it is so rare, like they’re so baffled,” Bassan says of PMPS. “But this is statistically predictable.” (Amy Maxmen/KFF Health News) Bank, a New York surgeon who founded a clinic focused on post-mastectomy pain, said the pain is believed to be triggered by nerves that are severed during surgery and then left that way.
The nerves can be sutured back together to minimize pain, Bank said, but most breast surgeons haven’t been trained to do this. So it is not surprising, he said, that some patients say their surgeons were dismissive of their pain after mastectomies.
“When doctors don’t have an answer or don’t know the solution, the easiest thing to do is say there is no problem,” Bank said.
PMPS has been documented among cancer patients since the 1970s. Although the condition does not have an official definition, many researchers describe it as frequent pain in the chest, shoulder, arm, or armpit lasting at least three months after surgery.
Mastectomies intended to prevent breast cancer have become more common among women with elevated risks, including genetic mutations and a family history of the disease.
Bassan’s grandmother died of breast cancer when she was 40. After her father died of cancer in 2023, a genetic test showed that she was at risk. Grieving and afraid, Bassan sought a preventive mastectomy without hesitation, she said.
Bassan said she was also inspired by actor Angelina Jolie, who disclosed her own preventive mastectomy in a 2013 column in The New York Times. Her account had such a significant impact on rates of genetic testing and preventive mastectomies that medical researchers have studied what they call the “Angelina Jolie effect.”
“I was really swayed by that,” Bassan said. “She made it sound, in a way, quite effortless.”
Bassan stands beside a painting of her grandmother, who died of breast cancer at 40. With a family history of breast cancer and a genetic test showing she was at risk, Bassan decided to undergo a preventive mastectomy. (Amy Maxmen/KFF Health News) The aftermath of Bassan’s surgery was far worse than she expected. Using a computer for hours triggered paralyzing pain, so she lost her job and has been out of work for more than a year. Prescription pills dulled the pain but left her in a fog, she said. Desperate, she consulted with multiple doctors until one suggested a nerve stimulation machine, which provided fleeting relief.
About nine months after her mastectomy, a breast reconstruction surgery lessened Bassan’s pain, although she said it still returns in occasional waves. Even though her surgeries were covered by insurance, Bassan estimated her pain has cost her more than $200,000 in lost wages and drained savings.
“I did not expect to pay this price to have this surgery,” Bassan said. “I don’t know if it was worth it.”
Other women have no real choice.
No ‘Gold Standard’ Solution
Jeni Golomb, 48, was diagnosed with stage 2 cancer in both breasts in 2023 and had a double mastectomy as soon as she could.
Doctors made boilerplate disclosures of possible complications, Golomb said, but she never heard the words “post-mastectomy pain syndrome” until after she had it.
Golomb now manages her chronic pain by taking 1,500 milligrams a day of gabapentin, an anti-seizure drug that can also be used to treat nerve pain. Golomb said she expects to take the drug for years. If she misses a dose, her pain comes roaring back.
“It was the worst pain I ever felt,” Golomb said. “I labored to 10 centimeters, unmedicated, with one of my children, and that was not as bad as this. It was excruciating.”
Gabapentin has proved effective at helping some mastectomy patients with stubborn pain, while others have responded to electrodes implanted in their spinal column, according to the Baylor study, published in 2024.
But that study also said there is “no current gold standard” for how to treat post-mastectomy pain and a scarcity of high-level evidence for what treatments are effective.
Baylor anesthesiologist Krishna Shah, who co-authored the report, said many patients eventually find a helpful treatment, but it often takes “a bit of trial and error” to identify what works for each.
And sometimes they never find it.
Susan Dishell, 67, said that after her 2017 mastectomy for breast cancer and reconstruction surgery, she struggled for five years with pain in both shoulders, plus a burning sensation that her medical records identified as nerve pain.
Another surgery swapped out her breast implants to erase her shoulder pain in 2022, Dishell said, but doctors warned her then that her other pain was unlikely to improve.
Since then, she has tried prescription drugs, steroid injections, CBD oil, acupuncture, physical therapy, and chiropractor treatments.
None of it worked, she said, so she stopped trying.
“I have not slept through the night since I’ve had this,” Dishell said. “But it’s OK. It’s not the most terrible price to pay to not have breast cancer.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Getting Your Messy Life In Order
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Getting Your Messy Life In Order
We’ve touched on this before by recommending the book, but today we’re going to give an overview of the absolute most core essentials of the “Getting Things Done” method. If you’re unfamiliar, this will be enough to get you going. If you’re already familiar, this may be a handy reminder!
First, you’ll need:
- A big table
- A block of small memo paper squares—post-it note sized, but no need to be sticky.
- A block of A4 printer paper
- A big trash bag
Gathering everything
Gather up not just all your to-dos, but: all sources of to-dos, too, and anything else that otherwise needs “sorting”.
Put them all in one physical place—a dining room table may have enough room. You’ll need a lot of room because you’re going to empty our drawers of papers, unopened (or opened and set aside) mail. Little notes you made for yourself, things stuck on the fridge or memo boards. Think across all areas of your life, and anything you’re “supposed” to do, write it down on a piece of paper. No matter what area of your life, no matter how big or small.
Whether it’s “learn Chinese” or “take the trash out”, write it down, one item per piece of paper (hence the block of little memo squares).
Sorting everything
Everything you’ve gathered needs one of three things to happen:
- You need to take some action (put it in a “to do” pile)
- You may need it later sometime (put it in a “to file” pile)
- You don’t need it (put it in the big trash bag for disposal)
What happens next will soothe you
- Dispose of the things you put for disposal
- File the things for filing in a single alphabetical filing system. If you don’t have one, you’ll need to get one, so write that down and add it to the “to do” pile.
- You will now process your “to dos”
Processing the “to dos”
The pile you have left is now your “inbox”. It’s probably huge; later it’ll be smaller, maybe just a letter-tray on your desk.
Many of your “to dos” are actually not single action items, they’re projects. If something requires more than one step, it’s a project.
Take each item one-by-one. Do this in any order; you’re going to do this as quickly as possible! Now, ask yourself: is this a single-action item that I could do next, without having to do something else first?
- If yes: put it in a pile marked “next action”
- If no: put it in a pile marked “projects”.
Take a sheet of A4 paper and fold it in half. Write “Next Action” on it, and put your pile of next actions inside it.
Take a sheet of A4 paper per project and write the name of the project on it, for example “Learn Chinese”, or “Do taxes”. Put any actions relating to that project inside it.
Likely you don’t know yet what the first action will be, or else it’d be in your “Next Action” pile, so add an item to each project that says “Brainstorm project”.
Processing the “Next Action” pile
Again you want to do this as quickly as possible, in any order.
For each item, ask yourself “Do I care about this?” If the answer is no, ditch that item, and throw it out. That’s ok. Things change and maybe we no longer want or need to do something. No point in hanging onto it.
For each remaining item, ask yourself “can this be done in under 2 minutes?”.
- If yes, do it, now. Throw away the piece of paper for it when you’re done.
- If no, ask yourself:”could I usefully delegate this to someone else?” If the answer is yes, do so.
If you can’t delegate it, ask yourself: “When will be a good time to do this?” and schedule time for it. A specific, written-down, clock time on a specific calendar date. Input that into whatever you use for scheduling things. If you don’t already use something, just use the calendar app on whatever device you use most.
The mnemonic for the above process is “Do/Defer/Delegate/Ditch”
Processing projects:
If you don’t know where to start with a project, then figuring out where to start is your “Next Action” for that project. Brainstorm it, write down everything you’ll need to do, and anything that needs doing first.
The end result of this is:
- You will always, at any given time, have a complete (and accessible) view of everything you are “supposed” to do.
- You will always, at any given time, know what action you need to take next for a given project.
- You will always, when you designate “work time”, be able to get straight into a very efficient process of getting through your to-dos.
Keeping on top of things
- Whenever stuff “to do something with/about” comes to you, put it in your physical “inbox” place—as mentioned, a letter-tray on a desk should suffice.
- At the start of each working day, quickly process things as described above. This should be a small daily task.
- Once a week, do a weekly review to make sure you didn’t lose sight of something.
- Monthly, quarterly, and annual reviews can be a good practice too.
How to do those reviews? Topic for another day, perhaps.
Or:
Check out the website / Check out GTD apps / Check out the book
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:





