CBD Oil’s Many Benefits
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
CBD Oil: What Does The Science Say?
First, a quick legal (and practical) note:
CBD and THC are both derived from the hemp or cannabis plant, but only the latter has euphoriant psychoactive effects, i.e., will get you high. We’re writing here about CBD derived from hemp and not containing THC (thus, will not get you high).
Laws and regulations differ far too much from place to place for us to try to advise here, so please check your own local laws and regulations. And also, while you’re at it, with your doctor and/or pharmacist.
As ever, this newsletter is for purposes of education and enjoyment, and does not constitute any kind of legal (or medical) advice.
With that in mind, onwards to today’s research review…
CBD for Pain Relief
CBD has been popularly touted as a pain relief panacea, and there are a lot of pop-science articles out there “debunking” this, but…
The science seems to back it up. We couldn’t find studies refuting the claim (of CBD as a viable pain relief option). We did, however, find research showing it was good against:
Note that that latter (itself a research review, not a single study, hence covering a lot of bases) describes it matter-of-factly, with no caveats or weasel-words, as:
“CBD, a non-euphoriant, anti-inflammatory analgesic with CB1 receptor antagonist and endocannabinoid modulating effects”
As a quick note: all of the above is about the topical use of CBD oil, not any kind of ingestion
CBD for Anxiety/Depression
There’s a well-cited study with what honestly we think was a bit of a small sample size, but compelling results within that:
A study published in the Brazilian Journal of Psychiatry tested the anxiety levels of 57 men in a simulated public speaking test.
Compared to placebo…
- Those who received 300mg of CBD experienced significantly reduced anxiety during the test.
- Those who received either 150mg or 600mg of CBD experienced more anxiety during the test than the 300mg group
- This means there’s a sweet spot to the dosage
There was also a clinical study that found CBD to have anti-depressant effects.
The methodology was a lot more robust, but the subjects were mice. We can’t have everything in one study, apparently! There is probably a paucity of human volunteers to have their brain slices looked at after tests, though.
Anyway, what makes this study interesting is that it measured quite an assortment of biological markers in the brain, and found that the CBD had a similar physiological effect to the antidepressant imipramine.
CBD for Treating Opioid Addiction
There are a lot of studies for this, both animal and human, but we’d like to put the spotlight on a human study (with the participation of heroin users) that found:
❝Within one week, CBD significantly reduced cravings, anxiety, resting heart rate, and salivary cortisol levels. No serious adverse effects were found.❞
This is groundbreaking because the very thing about heroin is that it’s so addictive and the body rapidly needs more and more of it. You might think “duh”, but most people don’t realize this part:
Heroin is attractive because it offers (and delivers) an immediate guaranteed “downer”, instant relaxation… with none of the bad side effects of, for example, alcohol. No nausea, no hangover, nothing.
The problem is that the body gets tolerant to heroin very quickly, meaning your doses need to get bigger and more frequent to have the same effect.
Before you know it, what seemed like an affordable “self-medication for a stressful life” is very much out of control! Many doctors have personally found this out the hard way.
So, it’s ruinous:
- first to your financial health, as the costs rapidly spiral
- then to your physical health, as you either suffer from withdrawal or eventually overdose
Consequently, heroin is an incredibly easy drug to get hooked onto, and incredibly difficult to get back off.
So CBD offering relief is really a game-changer.
And more…
CBD has been well-studied and found to be effective for a lot of things, more than we could hope to cover in a single edition here.
Some further reading that may interest you includes:
- CBD against Diabetes in mice / in vitro / in humans
- CBD against neurological diseases (in general, in humans)
- CBD against arthritis in mice / in humans
- CBD specifically against the pain of rheumatoid arthritis / of osteoarthritis
Let us know if there’s any of these (or other) conditions you’d like us to look more into the CBD-related research for, because there’s a lot! You can always hit reply to any of our emails, or use the feedback widget at the bottom
Read (and shop, if you want and it’s permitted where you are):
10 Best CBD Oils of 2023, According to the Forbes Health Advisory Board
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What to Know About Stillbirths

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Series: Stillbirths:When Babies Die Before Taking Their First Breath
The U.S. has not prioritized stillbirth prevention, and American parents are losing babies even as other countries make larger strides to reduce deaths late in pregnancy.
Every year, more than 20,000 pregnancies in the U.S. end in a stillbirth, the death of an expected child at 20 weeks or more of pregnancy. Research shows as many as 1 in 4 stillbirths may be preventable. We interviewed dozens of parents of stillborn children who said their health care providers did not tell them about risk factors or explain what to watch for while pregnant. They said they felt blindsided by what followed. They did not have the information needed to make critical decisions about what happened with their baby’s body, about what additional testing could have been done to help determine what caused the stillbirth, or about how to navigate the process of requesting important stillbirth documents.
This guide is meant to help fill the void of information on stillbirths. It’s based on more than 150 conversations with parents, health care providers, researchers and other medical experts.
Whether you’re trying to better prepare for a pregnancy or grieving a loss, we hope this will help you and your family. This guide does not provide medical advice. We encourage you to seek out other reliable resources and consult with providers you trust.
We welcome your thoughts and questions at mailto:[email protected]. You can share your experience with stillbirth with us. If you are a health care provider interested in distributing this guide, let us know if we can help.
Table of contents:
- What Is Stillbirth?
- Are Stillbirths Preventable?
- What to Expect After a Stillbirth.
- Grieving After a Stillbirth.
- What You Might Say and Do After a Loved One Experiences a Stillbirth.
What Is Stillbirth?
Many people told us that the first time they heard the term stillbirth was after they delivered their stillborn baby. In many cases, the lack of information and awareness beforehand contributed to their heartache and guilt afterward.
Stillbirth is defined in the U.S. as the death of a baby in the womb at 20 weeks or more of pregnancy. Depending on when it happens, stillbirth is considered:
- Early: 20-27 weeks of pregnancy.
- Late: 28-36 weeks of pregnancy.
- Term: 37 or more weeks of pregnancy.
About half of all stillbirths in the U.S. occur at 28 weeks or later.
What is the difference between a stillbirth and a miscarriage?
Both terms describe pregnancy loss. The distinction is when the loss occurs. A miscarriage is typically defined as a loss before the 20th week of pregnancy, while stillbirth is after that point.
How common is stillbirth?
Each year, about 1 in 175 deliveries in the U.S. are stillbirths — that’s about 60 stillborn babies every day — making it one of the most common adverse pregnancy outcomes, but it is rarely discussed.
If you are surprised by that fact, you are not alone. Many people we spoke to did not know how common stillbirths are. Leandria Lee of Texas said she spent her 2021 pregnancy unaware that her daughter, Zuri Armoni, could die in the last phase of her pregnancy.
“If I was prepared to know that something could happen, I don’t think it would have been as bad. But to not know and then it happens, it affects you,” she said of her stillbirth at 35 weeks.
Some doctors have told us they don’t introduce the possibility of a stillbirth because they don’t want to create additional anxiety for patients.
Other doctors say withholding information leaves patients unprepared.
“We have this idea that we can’t scare the patient, which to me is very paternalistic,” said Dr. Heather Florescue, an OB-GYN near Rochester, New York, who works to inform doctors and patients about stillbirth prevention.
What causes stillbirths?
There is a lot we don’t know about stillbirths because there hasn’t been enough research. The cause of the stillbirth is unknown in about 1 in 3 cases.
What we do know is that a number of factors may cause or increase the risk of a stillbirth, including:
- The baby not growing as expected.
- Placental abnormalities or problems with the umbilical cord.
- Genetic or structural disorders that cause developmental issues.
- High blood pressure before pregnancy or preeclampsia, a potentially fatal complication that usually appears late in pregnancy and causes high blood pressure.
- Diabetes before or during pregnancy.
- An infection in the fetus, the placenta or the pregnant person.
- Smoking.
- Being 35 or older.
- Obesity.
- Being pregnant with more than one baby.
But not all doctors, hospitals or health departments perform tests to identify the potential cause of a stillbirth or determine if it could have been prevented. Even when a cause is identified, fetal death records are rarely updated. This means data is sometimes inaccurate. Researchers strongly encourage doctors to perform a stillbirth evaluation, which includes an examination of the placenta and umbilical cord, a fetal autopsy and genetic testing.
If your hospital or doctor does not proactively offer one or more of these exams, you can ask them to conduct the tests. Research shows that placental exams may help establish a cause of death or exclude a suspected one in about 65% of stillbirths, while autopsies were similarly useful in more than 40% of cases.
Are Stillbirths Preventable?
Not all stillbirths are preventable, but some are. For pregnancies that last 37 weeks or more, one study found that nearly half of stillbirths are potentially preventable.
Dr. Joanne Stone, who last year was president of the Society of Maternal-Fetal Medicine, leads the country’s first Rainbow Clinic at Mount Sinai Hospital in New York. The clinic is modeled on similar facilities in the United Kingdom that care for people who want to conceive again after a stillbirth. She said many doctors used to think there was nothing they could do to prevent stillbirth.
“People just looked at it like, ‘Oh, it was an accident, couldn’t have been prevented,’” said Stone, who also is the system chair of the obstetrics, gynecology and reproductive science department at the Icahn School of Medicine. “But we know now there are things that we can do to try to prevent that from happening.”
She said doctors can:
- More closely monitor patients with certain risk factors, like high blood pressure, diabetes or obesity.
- Ask about prior infant loss or other obstetrical trauma.
- Carefully assess whether a baby’s growth is normal.
- Work to diagnose genetic anomalies.
- Teach patients how to track their baby’s movements and encourage them to speak up if they notice activity has slowed or stopped.
- Deliver at or before 39 weeks if there are concerns.
What are the risks of stillbirth over the course of a pregnancy?
The risk of a stillbirth increases significantly toward the end of pregnancy, especially after 39 weeks. The risk is higher for people who get pregnant at 35 or older. The risk begins to climb even earlier, around 36 weeks, for people pregnant with twins.
What you and your doctor can do to reduce the risk of stillbirth.
While federal agencies in the U.S. have yet to come up with a checklist that may help reduce the risk of stillbirth, the Stillbirth Centre of Research Excellence in Australia has adopted a Safer Baby Bundle that lists five recommendations:
- Stop smoking.
- Regularly monitor growth to reduce the risk of fetal growth restriction, when the fetus is not growing as expected.
- Understand the importance of acting quickly if fetal movement decreases.
- Sleep on your side after 28 weeks.
- Talk to your doctor about when to deliver. Depending on your situation, it may be before your due date.
The American College of Obstetricians and Gynecologists has compiled a list of tests and techniques doctors can use to try to reduce the risk of a stillbirth. They include:
- A risk assessment to identify prenatal needs.
- A nonstresstest, which checks the fetus’s heart rate and how it changes as the fetus moves.
- A biophysical profile, which is done with an ultrasound to measure body movement, muscle tone and breathing, along with amniotic fluid volume.
The group stressed that there is no test that can guarantee a stillbirth won’t happen and that individual circumstances should determine what tests are run.
Are some people at higher risk for stillbirth?
Black women are more than twice as likely to have a stillbirth as white women. There are a number of possible explanations for that disparity, including institutional bias and structural racism, and a patient’s pre-pregnancy health, socioeconomic status and access to health care. In addition, research shows that Black women are more likely than white women to experience multiple stressful life events while pregnant and have their concerns ignored by their health care provider. Similar racial disparities drive the country’s high rate of maternal mortality.
How to find a provider you trust.
Finding a doctor to care for you during your pregnancy can be a daunting process. Medical experts and parents suggest interviewing prospective providers before you decide on the right one.
Here is a short list of questions you might want to ask a potential OB-GYN:
- What is the best way to contact you if I have questions or concerns?
- How do you manage inquiries after hours and on weekends? Do you see walk-ins?
- How do you manage prenatal risk assessments?
- What should I know about the risks of a miscarriage or stillbirth?
- How do you decide when a patient should be induced?
If a provider doesn’t answer your questions to your satisfaction, don’t be reluctant to move on. Dr. Ashanda Saint Jean, chair of the obstetrics and gynecology department at HealthAlliance Hospitals of the Hudson Valley in New York, said she encourages her patients to find the provider that meets their needs.
“Seek out someone that is like-minded,” said Saint Jean “It doesn’t have to be that they’re the same ethnicity or the same race, but like-minded in terms of the goals of what that patient desires for their own health and prosperity.”
What to know in the last trimester.
The last trimester can be an uncomfortable and challenging time as the fetus grows and you get increasingly tired. During this critical time, your provider should talk to you about the following topics:
- Whether you need a nonstress test to determine if the fetus is getting enough oxygen.
- The best way to track fetal movements.
- What to do if your baby stops moving.
- Whether you are at risk for preeclampsia or gestational diabetes.
Rachel Foran’s child, Eoin Francis, was stillborn at 41 weeks and two days. Foran, who lives in New York, said she believes that if her doctor had tracked her placenta, and if she had understood the importance of fetal movement, she and her husband might have decided to deliver sooner.
She remembers that her son was “very active” until the day before he was stillborn.
“I would have gone in earlier if someone had told me, ‘You’re doing this because the baby could die,’” she said of tracking fetal movement. “That would have been really helpful to know.”
Researchers are looking at the best way to measure the health, blood flow and size of the placenta, but studies are still in their early stages.
“If someone had been doing that with my son’s,” Foran said, “my son would be alive.”
A placental exam and an autopsy showed that a small placenta contributed to Foran’s stillbirth.
How often should you feel movement?
Every baby and each pregnancy are different, so it is important to get to know what levels of activity are normal for you. You might feel movement around 20 weeks. You’re more likely to feel movement when you’re sitting or lying down. Paying attention to movement during the third trimester is particularly important because research shows that changes, including decreased movement or bursts of excessive activity, are associated with an increased risk of stillbirth. Most of the time, it’s nothing. But sometimes it can be a sign that your baby is in distress. If you’re worried, don’t rely on a home fetal doppler to reassure you. Reach out to your doctor.
Saint Jean offers a tip to track movement: “I still tell patients each day to lay on their left side after dinner and record how many times their baby moves, because then that will give you an idea of what’s normal for your baby,” she said.
Other groups recommend using the Count the Kicks app as a way of tracking fetal movements and establishing what is normal for that pregnancy. Although there is no scientific consensus that counting kicks can prevent stillbirths, the American College of Obstetricians and Gynecologists and other groups recommend that patients be aware of fetal movement patterns.
Dr. Karen Gibbins is a maternal-fetal medicine specialist at Oregon Health & Science University who in 2018 had stillborn son named Sebastian. She said the idea that babies don’t move as much at the end of pregnancy is a dangerous myth.
“You might hear that babies slow down at the end,” she said. “They don’t slow down. They just have a little less space. So their movements are a little different, but they should be as strong and as frequent.”
What to Expect After a Stillbirth
What might happen at the hospital?
Parents are often asked to make several important decisions while they are still reeling from the shock and devastation of their loss. It’s completely understandable if you need to take some time to consider them.
Some other things you can ask for (if medical personnel don’t offer them) are:
- Blood work, a placental exam, an autopsy and genetic testing.
- A social worker or counselor, bereavement resources and religious or chaplain support.
- The option to be isolated from the labor rooms.
- Someone to take photos of you and your baby, typically either a nurse or an outside group.
- A small cooling cot that allows parents to spend more time with their babies after a stillbirth. If one is not available, you can ask for ice packs to put in the swaddle or the bassinet.
- A mold of your baby’s hands and feet.
- Information about burial or cremation services.
- Guidance on what to do if your milk comes in.
Getting an autopsy after a stillbirth.
Whether to have an autopsy is a personal decision. It may not reveal a cause of death, but it might provide important information about your stillbirth and contribute to broader stillbirth research. Autopsies can be useful if you are considering another pregnancy in the future. Families also told us that an autopsy can help parents feel they did everything they could to try to understand why their baby died.
But several families told us their health care providers didn’t provide them with the right information to help with that decision. Some aren’t trained in the advantages of conducting an autopsy after a stillbirth, or in when and how to sensitively communicate with parents about it. Some, for example, don’t explain that patients can still have an open-casket funeral or other service after an autopsy because the incisions can easily be covered by clothing. Others may not encourage an autopsy because they think they already know what caused the stillbirth or don’t believe anything could have been done to prevent it. In addition, not all hospitals have the capacity to do an autopsy, but there may be private autopsy providers that can perform one at an additional cost.
You can read more about autopsies in our reporting.
Paying for an autopsy after a stillbirth.
If you decide you want an autopsy, you may wonder whether you need to pay out-of-pocket for it. Several families told us their providers gave them incomplete or incorrect information. Many larger or academic hospitals offer autopsies at no cost to patients. Some insurance companies also cover the cost of an autopsy after a stillbirth.
When hospitals don’t provide an autopsy, they may give you names of private providers. That was the case for Rachel Foran. The hospital gave her and her husband a list of numbers to call if they wanted to pay for an autopsy themselves. The process, she said, shocked her.
“I had just delivered and we had to figure out what to do with his body,” Foran said. “It felt totally insane that that was what we had to do and that we had to figure it out on our own.”
An independent autopsy, records show, cost them $5,000.
What is a certificate of stillbirth and how do I get one?
A fetal death certificate is the official legal document that records the death. This is the document used to gather data on and track the number of stillbirths in the country. Many states also issue a certificate of stillbirth or a certificate of birth resulting in stillbirth, which acknowledge the baby’s birth. Families told us they appreciated having that document, since typical birth certificates are not issued for stillbirths. You can usually request a certificate from the vital records office.
Grieving After a Stillbirth
What are the effects of stillbirths on parents and families?
Over and over, families told us the effects of losing a baby can reverberate for a lifetime.
Bereavement support groups may help provide a space to share experiences and resources. Hospitals and birth centers may suggest a local grief group.
We talked with Anna Calix, a maternal health expert who became active in perinatal loss prevention after her son Liam was stillborn on his due date in 2016. Calix leads grief support groups for people of color in English and Spanish.
She suggested rededicating the time you would have spent taking care of a new baby to the grief process.
“You can do that by addressing your own thoughts and feelings and really experiencing those feelings,” Calix said. “We like to push those feelings away or try to do something to distract and avoid, but no matter what we do, the feelings are there.”
It’s important, she said, to give yourself permission to grow your connection with your child and work through thoughts of guilt or blame.
What You Might Say and Do After a Loved One Experiences a Stillbirth
Finding the right words can be difficult. The following are a few suggestions from parents who went through a stillbirth.
Helpful:
- Acknowledge the loss and offer condolences.
- Ask if the baby was named and use the name.
- Allow space for the family to talk about their baby.
Unhelpful:
- Avoid talking about the baby.
- Minimize the loss or compare experiences.
- Start statements with “at least.”
Suggested phrases to avoid:
- “You’re young. You can have more kids.”
- “At least you have other children.”
- “These things just happen.”
- “Your baby is in a better place now.”
Share This Post
-

Fix Your Upper Back With These Three Steps
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to back pain, the lower back gets a lot of attention, but what about when it’s nearer the neck and shoulders?
Reaching for better health
In this short video, Liv describes and shows three exercises:
Exercise 1: Thoracic Pullover (Dumbbell Pullover)
Purpose: Improves overhead reach and shoulder mobility.
Equipment: light weight, yoga block, or foam roller.
Steps:- Lie on the floor with the foam roller/block beneath the upper back.
- Hold the weight in both hands, arms extended upward.
- Inhale deeply and reach the weight toward the ceiling.
- Exhale and arc your spine over the block, moving the weight backward.
- Keep core tension to maintain a neutral lower back position.
- Perform 10 repetitions.
Exercise 2: Rotational Mobility Stretch
Purpose: enhances torso rotation, core strength, and hip mobility.
Equipment: none (or a mat)
Steps:- Lie on your side with knees stacked at 90° and arms extended in front.
- Hold a weight in the top hand.
- Inhale and lift the top arm toward the ceiling, extending the shoulder blade.
- Exhale and twist your torso, allowing the arm to move toward the floor.
- Modify by extending the bottom leg for a deeper twist if needed.
- Perform 6 reps per side, switching legs and repeating on the other side.
Exercise 3: Doorway/Pole Side Stretch
Purpose: targets multiple areas for a deep, satisfying stretch.
Equipment: door frame, pole, or wall.
Steps:- Stand at arm’s length from the wall or frame.
- Cross the outer leg (furthest from the wall) behind the inner leg.
- Place the closest hand on the wall and reach the other arm overhead.
- Grip the wall or frame with the top hand, pressing away with the bottom hand.
- Lean into a banana-shaped curve and rotate your chest upward for a deeper stretch.
- Hold for 20–30 seconds per side and repeat 2–3 times.
For more on all of these, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Share This Post
-

Egg Noodles vs Rice Noodles – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing egg noodles to rice noodles, we picked the egg noodles.
Why?
It was close—these are both quite mediocre foods. They’re neither amazing for the health nor appalling for the health (in moderation). They are both relatively low in nutrients, but they are also low in anti-nutrients, i.e. things that have a negative effect on the health.
Their mineral profiles are similar; both are a source of selenium, manganese, phosphorus, copper, and iron. Not as good as many sources, but not devoid of nutrients either.
Their vitamin profiles are both pitiful; rice noodles have trace amounts of various vitamins, and egg noodles have only slightly more. While eggs themselves are nutritious, the processing has robbed them of much of their value.
In terms of macros, egg noodles have a little more fat (but the fats are healthier) and rice noodles have a lot more carbs, so this is the main differentiator, and is the main reason we chose the egg noodles over the rice noodles. Both have a comparable (small) amount of protein.
In short:
- They’re comparable on minerals, and vitamins here are barely worth speaking about (though egg noodles do have marginally more)
- Egg noodles have a little more fat (but the fats are healthier)
- Rice noodles have a lot more carbs (with a moderately high glycemic index, which is relatively worse—if you eat them with vegetables and fats, then that’ll offset this, but we’re judging the two items on merit, not your meal)
Learn more
You might like this previous main feature of ours:
Should You Go Light Or Heavy On Carbs?
Take care!
Share This Post


Related Posts
-

How Science News Outlets Can Lie To You (Yes, Even If They Cite Studies!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Each Monday, we’re going to be bringing you cutting-edge research reviews to not only make your health and productivity crazy simple, but also, constantly up-to-date.
But today, in this special edition, we want to lay out plain and simple how to see through a lot of the tricks used not just by popular news outlets, but even sometimes the research publications themselves.
That way, when we give you health-related science news, you won’t have to take our word for it, because you’ll be able to see whether the studies we cite really support the claims we make.
Of course, we’ll always give you the best, most honest information we have… But the point is that you shouldn’t have to trust us! So, buckle in for today’s special edition, and never have to blindly believe sci-hub (or Snopes!) again.

The above now-famous Tumblr post that became a meme is a popular and obvious example of how statistics can be misleading, either by error or by deliberate spin.
But what sort of mistakes and misrepresentations are we most likely to find in real research?
Spin Bias
Perhaps most common in popular media reporting of science, the Spin Bias hinges on the fact that most people perceive numbers in a very “fuzzy logic” sort of way. Do you?
Try this:
- A million seconds is 11.5 days
- A billion seconds is not weeks, but 13.2 months!
…just kidding, it’s actually nearly thirty-two years.
Did the months figure seem reasonable to you, though? If so, this is the same kind of “human brains don’t do large numbers” problem that occurs when looking at statistics.
Let’s have a look at reporting on statistically unlikely side effects for vaccines, as an example:
- “966 people in the US died after receiving this vaccine!” (So many! So risky!)
- “Fewer than 3 people per million died after receiving this vaccine!” (Hmm, I wonder if it is worth it?)
- “Half of unvaccinated people with this disease die of it” (Oh)
How to check for this: ask yourself “is what’s being described as very common really very common?”. To keep with the spiders theme, there are many (usually outright made-up) stats thrown around on social media about how near the nearest spider is at any given time. Apply this kind of thinking to medical conditions.. If something affects only 1% of the population (So few! What a tiny number!), how far would you have to go to find someone with that condition? The end of your street, perhaps?
Selection/Sampling Bias
Diabetes disproportionately affects black people, but diabetes research disproportionately focuses on white people with diabetes. There are many possible reasons for this, the most obvious being systemic/institutional racism. For example, advertisements for clinical trial volunteer opportunities might appear more frequently amongst a convenient, nearby, mostly-white student body. The selection bias, therefore, made the study much less reliable.
Alternatively: a researcher is conducting a study on depression, and advertises for research subjects. He struggles to get a large enough sample size, because depressed people are less likely to respond, but eventually gets enough. Little does he know, even the most depressed of his subjects are relatively happy and healthy compared with the silent majority of depressed people who didn’t respond.

See This And Many More Educational Cartoons At Sketchplanations.com!
How to check for this: Does the “method” section of the scientific article describe how they took pains to make sure their sample was representative of the relevant population, and how did they decide what the relevant population was?
Publication Bias
Scientific publications will tend to prioritise statistical significance. Which seems great, right? We want statistically significant studies… don’t we?
We do, but: usually, in science, we consider something “statistically significant” when it hits the magical marker of p=0.05 (in other words, the probability of getting that result is 1/20, and the results are reliably coming back on the right side of that marker).
However, this can result in the clinic stopping testing once p=0.05 is reached, because they want to have their paper published. (“Yay, we’ve reached out magical marker and now our paper will be published”)
So, you can think of publication bias as the tendency for researchers to publish ‘positive’ results.
If it weren’t for publication bias, we would have a lot more studies that say “we tested this, and here are our results, which didn’t help answer our question at all”—which would be bad for the publication, but good for science, because data is data.
To put it in non-numerical terms: this is the same misrepresentation as the technically true phrase “when I misplace something, it’s always in the last place I look for it”—obviously it is, because that’s when you stop looking.
There’s not a good way to check for this, but be sure to check out sample sizes and see that they’re reassuringly large.
Reporting/Detection/Survivorship Bias
There’s a famous example of the rise in “popularity” of left-handedness. Whilst Americans born in ~1910 had a bit under a 3.5% chance of being left handed, those born in ~1950 had a bit under a 12% change.
Why did left-handedness become so much more prevalent all of a sudden, and then plateau at 12%?
Simple, that’s when schools stopped forcing left-handed children to use their right hands instead.
In a similar fashion, countries have generally found that homosexuality became a lot more common once decriminalized. Of course the real incidence almost certainly did not change—it just became more visible to research.
So, these biases are caused when the method of data collection and/or measurement leads to a systematic error in results.
How to check for this: you’ll need to think this through logically, on a case by case basis. Is there a reason that we might not be seeing or hearing from a certain demographic?
And perhaps most common of all…
Confounding Bias
This is the bias that relates to the well-known idea “correlation ≠ causation”.
Everyone has heard the funny examples, such as “ice cream sales cause shark attacks” (in reality, both are more likely to happen in similar places and times; when many people are at the beach, for instance).
How can any research paper possibly screw this one up?
Often they don’t and it’s a case of Spin Bias (see above), but examples that are not so obviously wrong “by common sense” often fly under the radar:
“Horse-riding found to be the sport that most extends longevity”
Should we all take up horse-riding to increase our lifespans? Probably not; the reality is that people who can afford horses can probably afford better than average healthcare, and lead easier, less stressful lives overall. The fact that people with horses typically have wealthier lifestyles than those without, is the confounding variable here.

See This And Many More Educational Cartoons on XKCD.com!
In short, when you look at the scientific research papers cited in the articles you read (you do look at the studies, yes?), watch out for these biases that found their way into the research, and you’ll be able to draw your own conclusions, with well-informed confidence, about what the study actually tells us.
Science shouldn’t be gatekept, and definitely shouldn’t be abused, so the more people who know about these things, the better!
So…would one of your friends benefit from this knowledge? Forward it to them!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why is cancer called cancer? We need to go back to Greco-Roman times for the answer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One of the earliest descriptions of someone with cancer comes from the fourth century BC. Satyrus, tyrant of the city of Heracleia on the Black Sea, developed a cancer between his groin and scrotum. As the cancer spread, Satyrus had ever greater pains. He was unable to sleep and had convulsions.
Advanced cancers in that part of the body were regarded as inoperable, and there were no drugs strong enough to alleviate the agony. So doctors could do nothing. Eventually, the cancer took Satyrus’ life at the age of 65.
Cancer was already well known in this period. A text written in the late fifth or early fourth century BC, called Diseases of Women, described how breast cancer develops:
hard growths form […] out of them hidden cancers develop […] pains shoot up from the patients’ breasts to their throats, and around their shoulder blades […] such patients become thin through their whole body […] breathing decreases, the sense of smell is lost […]
Other medical works of this period describe different sorts of cancers. A woman from the Greek city of Abdera died from a cancer of the chest; a man with throat cancer survived after his doctor burned away the tumour.
Where does the word ‘cancer’ come from?

Why does the word ‘cancer’ have its roots in the ancient Greek and Latin words for crab? The physician Galen offers one explanation. Pierre Roche Vigneron/Wikimedia The word cancer comes from the same era. In the late fifth and early fourth century BC, doctors were using the word karkinos – the ancient Greek word for crab – to describe malignant tumours. Later, when Latin-speaking doctors described the same disease, they used the Latin word for crab: cancer. So, the name stuck.
Even in ancient times, people wondered why doctors named the disease after an animal. One explanation was the crab is an aggressive animal, just as cancer can be an aggressive disease; another explanation was the crab can grip one part of a person’s body with its claws and be difficult to remove, just as cancer can be difficult to remove once it has developed. Others thought it was because of the appearance of the tumour.
The physician Galen (129-216 AD) described breast cancer in his work A Method of Medicine to Glaucon, and compared the form of the tumour to the form of a crab:
We have often seen in the breasts a tumour exactly like a crab. Just as that animal has feet on either side of its body, so too in this disease the veins of the unnatural swelling are stretched out on either side, creating a form similar to a crab.
Not everyone agreed what caused cancer
The physician Erasistratus didn’t think black bile was to blame. Didier Descouens/Musée Ingres-Bourdelle/Wikimedia, CC BY-SA In the Greco-Roman period, there were different opinions about the cause of cancer.
According to a widespread ancient medical theory, the body has four humours: blood, yellow bile, phlegm and black bile. These four humours need to be kept in a state of balance, otherwise a person becomes sick. If a person suffered from an excess of black bile, it was thought this would eventually lead to cancer.
The physician Erasistratus, who lived from around 315 to 240 BC, disagreed. However, so far as we know, he did not offer an alternative explanation.
How was cancer treated?
Cancer was treated in a range of different ways. It was thought that cancers in their early stages could be cured using medications.
These included drugs derived from plants (such as cucumber, narcissus bulb, castor bean, bitter vetch, cabbage); animals (such as the ash of a crab); and metals (such as arsenic).
Galen claimed that by using this sort of medication, and repeatedly purging his patients with emetics or enemas, he was sometimes successful at making emerging cancers disappear. He said the same treatment sometimes prevented more advanced cancers from continuing to grow. However, he also said surgery is necessary if these medications do not work.
Surgery was usually avoided as patients tended to die from blood loss. The most successful operations were on cancers of the tip of the breast. Leonidas, a physician who lived in the second and third century AD, described his method, which involved cauterising (burning):
I usually operate in cases where the tumours do not extend into the chest […] When the patient has been placed on her back, I incise the healthy area of the breast above the tumour and then cauterize the incision until scabs form and the bleeding is stanched. Then I incise again, marking out the area as I cut deeply into the breast, and again I cauterize. I do this [incising and cauterizing] quite often […] This way the bleeding is not dangerous. After the excision is complete I again cauterize the entire area until it is dessicated.
Cancer was generally regarded as an incurable disease, and so it was feared. Some people with cancer, such as the poet Silius Italicus (26-102 AD), died by suicide to end the torment.
Patients would also pray to the gods for hope of a cure. An example of this is Innocentia, an aristocratic lady who lived in Carthage (in modern-day Tunisia) in the fifth century AD. She told her doctor divine intervention had cured her breast cancer, though her doctor did not believe her.
Innocentia from Carthage, in modern-day Tunisia, believed divine intervention cured her breast cancer. Valery Bareta/Shutterstock From the past into the future
We began with Satyrus, a tyrant in the fourth century BC. In the 2,400 years or so since then, much has changed in our knowledge of what causes cancer, how to prevent it and how to treat it. We also know there are more than 200 different types of cancer. Some people’s cancers are so successfully managed, they go on to live long lives.
But there is still no general “cure for cancer”, a disease that about one in five people develop in their lifetime. In 2022 alone, there were about 20 million new cancer cases and 9.7 million cancer deaths globally. We clearly have a long way to go.
Konstantine Panegyres, McKenzie Postdoctoral Fellow, Historical and Philosophical Studies, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Cold Truth About Respiratory Infections
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Pathogens That Came In From The Cold

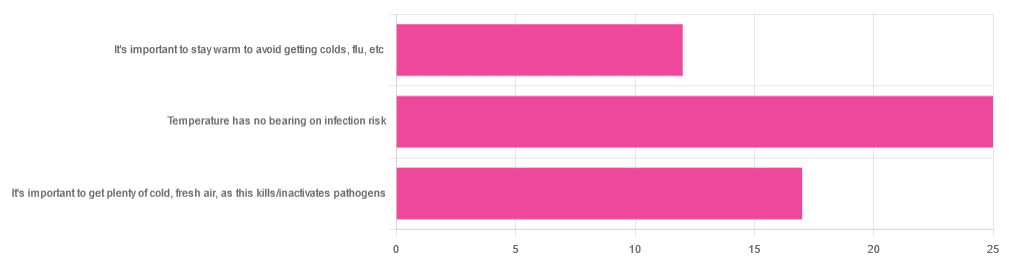
Yesterday, we asked you about your climate-themed policy for avoiding respiratory infections, and got the above-depicted, below-described, set of answers:
- About 46% of respondents said “Temperature has no bearing on infection risk”
- About 31% of respondents said “It’s important to get plenty of cold, fresh air, as this kills/inactivates pathogens”
- About 22% of respondents said “It’s important to stay warm to avoid getting colds, flu, etc”
Some gave rationales, including…
For “stay warm”:
❝Childhood lessons❞
For “get cold, fresh air”:
❝I just feel that it’s healthy to get fresh air daily. Whether it kills germs, I don’t know❞
For “temperature has no bearing”:
❝If climate issue affected respiratory infections, would people in the tropics suffer more than those in colder climates? Pollutants may affect respiratory infections, but I doubt just temperature would do so.❞
So, what does the science say?
It’s important to stay warm to avoid getting colds, flu, etc: True or False?
False, simply. Cold weather does increase the infection risk, but for reasons that a hat and scarf won’t protect you from. More on this later, but for now, let’s lay to rest the idea that bodily chilling will promote infection by cold, flu, etc.
In a small-ish but statistically significant study (n=180), it was found that…
❝There was no evidence that chilling caused any acute change in symptom scores❞
Read more: Acute cooling of the feet and the onset of common cold symptoms
Note: they do mention in their conclusion that chilling the feet “causes the onset of cold symptoms in about 10% of subjects who are chilled”, but the data does not support that conclusion, and the only clear indicator is that people who are more prone to colds generally, were more prone to getting a cold after a cold water footbath.
In other words, people who were more prone to colds remained more prone to colds, just the same.
It’s important to get plenty of cold, fresh air, as this kills/inactivates pathogens: True or False?
Broadly False, though most pathogens do have an optimal operating temperature that (for obvious reasons) is around normal human body temperature.
However, given that they don’t generally have to survive outside of a host body for long to get passed on, the fact that the pathogens may be a little sluggish in the great outdoors will not change the fact that they will be delighted by the climate in your respiratory tract as soon as you get back into the warm.
With regard to the cold air not being a reliable killer/inactivator of pathogens, we call to the witness stand…
Polar Bear Dies From Bird Flu As H5N1 Spreads Across Globe
(it was found near Utqiagvik, one of the northernmost communities in Alaska)
Because pathogens like human body temperature, raising the body temperature is a way to kill/inactivate them: True or False?
True! Unfortunately, it’s also a way to kill us. Because we, too, cannot survive for long above our normal body temperature.
So, for example, bundling up warmly and cranking up the heating won’t necessarily help, because:
- if the temperature is comfortable for you, it’s comfortable for the pathogen
- if the temperature is dangerous to the pathogen, it’s dangerous to you too
This is why the fever response evolved, and/but why many people with fevers die anyway. It’s the body’s way of playing chicken with the pathogen, challenging “guess which of us can survive this for longer!”
Temperature has no bearing on infection risk: True or False?
True and/or False, circumstantially. This one’s a little complex, but let’s break it down to the essentials.
- Temperature has no direct effect, for the reasons we outlined above
- Temperature is often related to humidity, which does have an effect
- Temperature does tend to influence human behavior (more time spent in open spaces with good ventilation vs more time spent in closed quarters with poor ventilation and/or recycled air), which has an obvious effect on transmission rates
The first one we covered, and the third one is self-evident, so let’s look at the second one:
Temperature is often related to humidity, which does have an effect
When the environmental temperature is warmer, water droplets in the air will tend to be bigger, and thus drop to the ground much more quickly.
When the environmental temperature is colder, water droplets in the air will tend to be smaller, and thus stay in the air for longer (along with any pathogens those water droplets may be carrying).
Some papers on the impact of this:
- Cold temperature and low humidity are associated with increased occurrence of respiratory tract infections
- A Decrease in Temperature and Humidity Precedes Human Rhinovirus Infections in a Cold Climate
So whatever temperature you like to keep your environment, humidity is a protective factor against respiratory infections, and dry air is a risk factor.
So, for example:
- If the weather doesn’t suit having good ventilation, a humidifier is a good option
- Being in an airplane is one of the worst places to be for this, outside of a hospital
Don’t have a humidifier? Here’s an example product on Amazon, but by all means shop around.
A crock pot with hot water in and the lid off is also a very workable workaround too
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: