Endure – by Alex Hutchinson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Life is a marathon, not a sprint. For most of us, at least. But how do we pace ourselves to go the distance, without falling into complacency along the way?
According to our author Alex Hutchinson, there’s a lot more to it than goal-setting and strategy.
Hutchinson set out to write a running manual, and ended up writing a manual for life. To be clear, this is still mostly centered around the science of athletic endurance, but covers the psychological factors as much as the physical… and notes how the capacity to endure is the key trait that underlies great performance in every field.
The writing style is both personal and personable, and parts read like a memoir (Hutchinson himself being a runner and sports journalist), while others are scientific in nature.
As for the science, the kind of science examined runs the gamut from case studies to clinical studies. We examine not just the science of physical endurance, but the science of psychological endurance too. We learn about such things as:
- How perception of ease/difficulty plays its part
- What factors make a difference to pain tolerance
- How mental exhaustion affects physical performance
- What environmental factors increase or lessen our endurance
- …and many other elements that most people don’t consider
Bottom line: whether you want to run a marathon in under two hours, or just not quit after one minute forty seconds on the exercise bike, or to get through a full day’s activities while managing chronic pain, this book can help.
Click here to check out Endure, and find out what you are capable of when you move your limits!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Pine Bark’s Next-Level Antioxidant Properties

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pine Bark’s Next-Level Antioxidant Properties
Pine bark extract has been used by the indigenous peoples of N. America for a very long time, to treat a variety of ailments.
This one falls into the category of “things from traditional medicine that eventually got investigated and their scientific worth noticed by people from outside of those cultures”.
Not all pine trees!
If you happen to have pine trees near you, be aware that without sufficient botanical knowledge, you could find yourself bark-harvesting from the wrong tree—but many species of pine do have these qualities.
Useful (for this purpose) pine trees include, but are not limited to:
- Pinus banksiana
- Pinus massoniana
- Pinus pinaster
- Pinus radiata
- Pinus resinosa
- Pinus strobus
…which is already a fair list, but there are dozens more that have not been studied, and/or found lacking in medicinal qualities, and/or just didn’t make our list here today.
What does it do & How does it work?
We sneakily put those two questions together today because it’s easiest to explain in one:
The Pinus family in general has powerful antioxidant qualities, and not just like blueberries or coffee (wonderful as those are).
Rather, it has:
- Phenolic acids: these are the polyphenols found in many plant foods rich in antioxidants. These are great, but they aren’t the exciting part here.
- Catechins: these aren’t classified as antioxidants, but they are flavonoids that do the same job in a slightly different way
- Procyanidins: another class of flavonoids, and this is where pine bark really comes into its own
And yes, as ever, “those three things that always seem to come together”, it having these antioxidant properties means it is also anti-inflammatory and anti-cancer:
…and anti-aging:
Pleiotropic Effects of French Maritime Pine Bark Extract to Promote Healthy Aging
…which does of course mean that it almost certainly fights age-related cognitive decline, though studies for that have been animal studies so far, such as:
- Pine Bark Polyphenolic Extract Attenuates Amyloid-β and Tau Misfolding in a Model System of Alzheimer’s Disease Neuropathology
- Neuroprotective and Anti-Inflammatory Effects of Pinus densiflora Bark Extract in Gerbil Hippocampus Following Transient Forebrain Ischemia
- Neuroprotective Effects of Korean Red Pine ( Pinus densiflora) Bark Extract and Its Phenolics
- Pine bark treatment decelerates plaque development and improves spatial memory in Alzheimer’s disease mice
Where to get it?
As ever, we don’t sell it, but here’s an example product on Amazon for your convenience; we recommend shopping around though, as prices vary a lot!
Enjoy!
Share This Post
-

No-Frills, Evidence-Based Mindfulness
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s on your mind, really?
We hear a lot about “the evidence-based benefits of mindfulness”, but what actually are they? And what is the evidence? And, perhaps most importantly: how do we do it?
What are the benefits?
The benefits of mindfulness are many, and include:
- reducing stress
- reducing pain
- improving quality of life
- reducing fatigue
- providing relief from digestive disorders
- reducing symptoms of sleep disorders
- improving immune response
- providing support for caregivers
The evidence is also abundant, and includes:
- Effects of mindfulness exercises as stand-alone intervention on symptoms of anxiety and depression: Systematic review and meta-analysis
- Fusing character strengths and mindfulness interventions: Benefits for satisfaction and performance
- Evidence for the Role of Mindfulness in Cancer: Benefits and Techniques
- Effects of mindfulness-based stress reduction on anxiety symptoms: A systematic review and meta-analysis
- The benefits of meditation and mindfulness practices during times of crisis such as COVID-19
Sounds great… What actually is it, though?
Mindfulness is the state of being attentive to one’s mind. This is at its heart a meditative practice, but that doesn’t necessarily mean you have to be sitting in the lotus position with candles—mindfulness can be built into any daily activity, or even no activity at all.
An exercise you can try right now:
Take a moment to notice everything you can hear. For this writer, that includes:
- The noise of my keystrokes as I type
- The ticking of the clock on the wall
- The gentle humming of my computer’s processor
- The higher-pitched noise of my computer’s monitor
- Birdsong outside
- Traffic further away
- My own breathing
- The sound of my eyelids as I blink
Whatever it is for you, notice how much you can notice that you had previously taken for granted.
You can repeat this exercise with other senses, by the way! For example:
- Notice five things you can see in your immediate environment that you’ve never noticed before. If you’re at home reading this, you probably think you’re very familiar with everything around you, but now see that mark on the wall you’d never noticed before, or a quirk of some electrical wiring, or the stitching on some furnishing, for example.
- Notice the textures of your clothes, or your face, or perhaps an object you’ve never paid attention to touching before. Your fingertips, unless you have some special reason this doesn’t apply to you, are far more sensitive than you probably give them credit for, and can notice the tiniest differentiation in textures, so take a moment to do that now.
- Mindful eating can be an especially healthful practice because it requires that we pay every attention to what we’re putting in our mouth, tasting, chewing, swallowing. No more thoughtlessly downing a box of cookies; every bite is now an experience. On the one hand, you’ll probably eat less at a sitting. On the other hand, what a sensory experience! It really reminds one that life is for living, not just for zipping through at a speed-run pace!
What about mindfulness as a meditative practice?
Well, those are meditative practices! But yes, mindfulness goes for more formal meditation too. For example:
Sit comfortably, with good posture, whatever that means to you. No need to get too caught up in the physical mechanics here—it’d take a whole article. For now, if you’re sitting and comfortable, that’s enough.
Notice your breathing. No need to try to control it—that’s not what this is about today. Just notice it. The in, the out, whether you breathe to your chest or abdomen, through your nose or mouth, don’t worry about doing it “right”, just notice what you are doing. Observe without judgement.
Notice your thoughts—no need to try to stop them. Notice noticing your thoughts, and again, observe without judgement. Notice your feelings; are you angry, hopeful, stressed, serene? There are no wrong answers here, and there’s nothing you should try to “correct”. Just observe. No judgement, only observe. Watch your thoughts, and watch your thoughts go.
Did you forget about your breathing while watching your thoughts? Don’t worry about that either if so, just notice that it happened. If you have any feelings about that, notice them too, and carry on observing.
We go through so much of our lives in “autopilot”, that it can be an amazing experience to sometimes just “be”—and be aware of being.
Share This Post
-

Are berries safe to eat? How worried should I be about the pesticide dimethoate?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australia’s regulator has suspended use of a common pesticide used on blueberries, raspberries and blackberries known as dimethoate.
But this year-long suspension isn’t due to any new information about the pesticide itself. Rather, the Australian Pesticides and Veterinary Medicines Authority (APVMA) says it’s because we’re eating more berries so our potential exposure has increased.
In particular, it says children aged two to six years may be at increased risk of exceeding maximum limits.
Here’s what we know about dimethoate and whether berries are still safe to eat. https://www.youtube.com/embed/dds_-BiSng4?wmode=transparent&start=0

Alexander Sinn/Unsplash What is dimethoate?
Dimethoate is a pesticide that has been used in Australia since 1956. It belongs to a class of pesticides that inhibits the enzyme acetylcholinesterase. This prevents the breakdown of a key neurotransmitter (chemical messenger) and so paralyses an insect’s nervous system, killing it.
Mammals, including humans, also have the enzyme acetylcholinesterase, and can be poisoned by this class of pesticide.
So careful regulation of both application of dimethoate and levels of dimethoate residues on food are required so we are not exposed to harmful levels.
The amount of maximum permissible residues depends, in turn, on how much someone is exposed to from their food.
To do this, you need to have estimates of how much residue is on food and how much food we eat.
How much is too much?
The APVMA has a maximum limit for how much dimethoate we should be exposed to from our food. This is known as the acute reference dose (or ARfD), which is 0.02 milligrams per kilogram of body weight.
This maximum dose includes a safety factor of ten. In other words, the maximum dose allowed is ten times lower than the lowest dose that has no effect.
This dose was set in 2017. But it is consistent with current World Health Organization limits and Canadian regulations. Australia’s maximum dose is lower than limits from the United States Environmental Protection Agency.
So, what’s changed?
But our dietary habits have changed. Australian consumption of blueberries, blackberries and raspberries has increased substantially since the APVMA last assessed dimethoate. Consumption is up 285–962% compared to levels considered for its 2017 assessment.
Eating more berries is a good thing. But this means that current trace levels of dimethoate on berries (0.0033 micrograms per kilogram of body weight per day for a toddler) might potentially exceed the maximum limit for children aged two to six years.
The APVMA states:
The level of residues detected are unlikely to pose a serious risk to human health, but has proposed suspension of these specific dimethoate products as a precautionary measure.
What can you do?
Don’t give up on berries. Eating berries is an important part of a balanced diet. And the APVMA is at pains to emphasise the risk of harm is low.
The simplest approach is to wash your berries. You should be washing fruit and vegetables anyway. Washing helps get rid of soil, and potentially harmful microorganisms.
Washing berries will not remove all dimethoate, but can substantially reduce the levels so you can continue to enjoy them and their benefits.
Ian Musgrave, Senior Lecturer in Pharmacology, University of Adelaide
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-
Spit or swallow? What’s the best way to deal with phlegm?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A spitting pot I consider as an essential part of the bed-room apparatus.
That’s what French physician René Laennec wrote in 1821. Laennec, who invented the stethoscope, spent his days gazing at his patients’ phlegm. In the days before x-rays and blood tests, phlegm was considered a valuable diagnostic tool.
Today, most of us don’t carry around a spitting pot. But a persistent question remains, especially during winter, when noses are dripping and chests are rattling.
When you have a cough, should you spit out phlegm or is it better to swallow it?
It might feel like an odd or even slightly stomach-churning topic, but it’s a remarkably common question patients ask doctors.
Pop Paul-Catalin/Shutterstock What is phlegm?
Phlegm, also known as sputum, is the thick, sticky mucus your lungs and windpipe make. This acts as a defensive barrier to protect them.
Its main ingredients are mucins – large, sugar-coated proteins that trap viruses, bacteria, allergens and dust. These mucins also regulate inflammation and the body’s immune response to bacteria and viruses.
We most commonly see phlegm with viral illness during winter. But phlegm is also evident in other medical conditions including asthma and allergies, bacterial infections, such as sinusitis, or with smoking or exposure to air pollution.
In fact, we’re always making phlegm, even when we are healthy. Cells in the lungs secrete mucus to keep surfaces moist and trap irritants. When we encounter something potentially harmful, such as a virus or allergen, immune cells detect the threat and release signals that tell mucus-producing cells to step up their game.
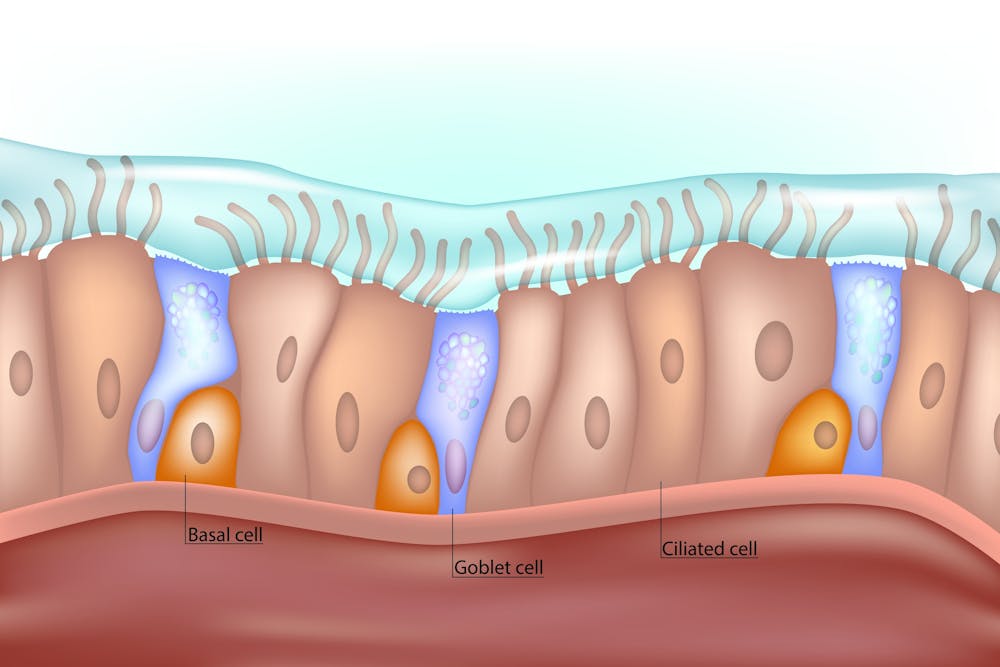
This extra mucus helps trap the invader and move it out of the lungs. Tiny hairs lining the airways (called cilia) then sweep the mucus up to the throat, where we cough it out or swallow it.
These tiny hairs, or cilia, sweep phlegm up to your throat. Sakurra/Shutterstock The case for spitting
Some people feel better if they spit out phlegm, especially if the phlegm is thick, sticky or irritates the throat.
Spitting also lets you see what’s coming up. If phlegm contains blood, for example, it is important to see a doctor to exclude a more serious underlying illness, such as tuberculosis or cancer.
If you do spit out, do so into a tissue and throw it in the bin. Wash your hands afterwards. This reduces the risk of spreading infection to others via respiratory droplets or contaminated surfaces.
However, spitting out phlegm isn’t always practical, or polite. And for most viral infections, it doesn’t help you get better any faster than swallowing. The aim is to remove phlegm from the lungs, which occurs with either method.
Spitting is also not feasible for young children, who haven’t yet developed the coordination to do so effectively. They’ll generally swallow their phlegm. https://www.youtube.com/embed/WW4skW6gucU?wmode=transparent&start=0 How mucus keeps us healthy all year round, even if we’re not sick.
The case for swallowing
It might not sound particularly appealing, but swallowing phlegm is a normal process, and harmless. In fact, we often swallow phlegm without realising it.
The lungs generate about 50 millilitres of phlegm daily. It goes unnoticed because it’s thin, blends with saliva and we continuously swallow it. We only become aware of it when it thickens, such as during a viral infection.
After you swallow phlegm, it travels to the stomach, where acid and enzymes break it down, along with any germs it carries.
Swallowing phlegm doesn’t “recycle” the germs, and it won’t result in the infection spreading elsewhere.
In fact, swallowing viruses can even help build immunity. Once inside the gut, immune cells begin to recognise pieces of the virus and start preparing the body to respond more effectively to it in the future. Some important immunisations, such as the oral polio vaccine, work through this very mechanism.
So, what’s the verdict?
Whether you spit or swallow phlegm, both are safe. Spitting can help some people feel better, especially if their cough is associated with thick phlegm that’s causing distress.
But for most healthy people, there’s no need to force a cough or spit out phlegm. Swallowing phlegm is completely safe. And in young children, it’s the only feasible option.
In the end, it won’t matter if you spit or swallow your phlegm this winter. So choose what feels right (and least icky) for you.
Niall Johnston, Conjoint Associate Lecturer, Faculty of Medicine, UNSW Sydney and Phoebe Williams, Paediatrician & Infectious Diseases Physician; Senior Lecturer & NHMRC Fellow, Faculty of Medicine, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Many Nonprofit (Wink, Wink) Hospitals Are Rolling in Money
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One owns a for-profit insurer, a venture capital company, and for-profit hospitals in Italy and Kazakhstan; it has just acquired its fourth for-profit hospital in Ireland. Another owns one of the largest for-profit hospitals in London, is partnering to build a massive training facility for a professional basketball team, and has launched and financed 80 for-profit start-ups. Another partners with a wellness spa where rooms cost $4,000 a night and co-invests with “leading private equity firms.”
Do these sound like charities?
These diversified businesses are, in fact, some of the country’s largest nonprofit hospital systems. And they have somehow managed to keep myriad for-profit enterprises under their nonprofit umbrella — a status that means they pay little or no taxes, float bonds at preferred rates, and gain numerous other financial advantages.
Through legal maneuvering, regulatory neglect, and a large dollop of lobbying, they have remained tax-exempt charities, classified as 501(c)(3)s.
“Hospitals are some of the biggest businesses in the U.S. — nonprofit in name only,” said Martin Gaynor, an economics and public policy professor at Carnegie Mellon University. “They realized they could own for-profit businesses and keep their not-for-profit status. So the parking lot is for-profit; the laundry service is for-profit; they open up for-profit entities in other countries that are expressly for making money. Great work if you can get it.”
Many universities’ most robust income streams come from their technically nonprofit hospitals. At Stanford University, 62% of operating revenue in fiscal 2023 was from health services; at the University of Chicago, patient services brought in 49% of operating revenue in fiscal 2022.
To be sure, many hospitals’ major source of income is still likely to be pricey patient care. Because they are nonprofit and therefore, by definition, can’t show that thing called “profit,” excess earnings are called “operating surpluses.” Meanwhile, some nonprofit hospitals, particularly in rural areas and inner cities, struggle to stay afloat because they depend heavily on lower payments from Medicaid and Medicare and have no alternative income streams.
But investments are making “a bigger and bigger difference” in the bottom line of many big systems, said Ge Bai, a professor of health care accounting at the Johns Hopkins University Bloomberg School of Public Health. Investment income helped Cleveland Clinic overcome the deficit incurred during the pandemic.
When many U.S. hospitals were founded over the past two centuries, mostly by religious groups, they were accorded nonprofit status for doling out free care during an era in which fewer people had insurance and bills were modest. The institutions operated on razor-thin margins. But as more Americans gained insurance and medical treatments became more effective — and more expensive — there was money to be made.
Not-for-profit hospitals merged with one another, pursuing economies of scale, like joint purchasing of linens and surgical supplies. Then, in this century, they also began acquiring parts of the health care systems that had long been for-profit, such as doctors’ groups, as well as imaging and surgery centers. That raised some legal eyebrows — how could a nonprofit simply acquire a for-profit? — but regulators and the IRS let it ride.
And in recent years, partnerships with, and ownership of, profit-making ventures have strayed further and further afield from the purported charitable health care mission in their community.
“When I first encountered it, I was dumbfounded — I said, ‘This not charitable,’” said Michael West, an attorney and senior vice president of the New York Council of Nonprofits. “I’ve long questioned why these institutions get away with it. I just don’t see how it’s compliant with the IRS tax code.” West also pointed out that they don’t act like charities: “I mean, everyone knows someone with an outstanding $15,000 bill they can’t pay.”
Hospitals get their tax breaks for providing “charity care and community benefit.” But how much charity care is enough and, more important, what sort of activities count as “community benefit” and how to value them? IRS guidance released this year remains fuzzy on the issue.
Academics who study the subject have consistently found the value of many hospitals’ good work pales in comparison with the value of their tax breaks. Studies have shown that generally nonprofit and for-profit hospitals spend about the same portion of their expenses on the charity care component.
Here are some things listed as “community benefit” on hospital systems’ 990 tax forms: creating jobs; building energy-efficient facilities; hiring minority- or women-owned contractors; upgrading parks with lighting and comfortable seating; creating healing gardens and spas for patients.
All good works, to be sure, but health care?
What’s more, to justify engaging in for-profit business while maintaining their not-for-profit status, hospitals must connect the business revenue to that mission. Otherwise, they pay an unrelated business income tax.
“Their CEOs — many from the corporate world — spout drivel and turn somersaults to make the case,” said Lawton Burns, a management professor at the University of Pennsylvania’s Wharton School. “They do a lot of profitable stuff — they’re very clever and entrepreneurial.”
The truth is that a number of not-for-profit hospitals have become wealthy diversified business organizations. The most visible manifestation of that is outsize executive compensation at many of the country’s big health systems. Seven of the 10 most highly paid nonprofit CEOs in the United States run hospitals and are paid millions, sometimes tens of millions, of dollars annually. The CEOs of the Gates and Ford foundations make far less, just a bit over $1 million.
When challenged about the generous pay packages — as they often are — hospitals respond that running a hospital is a complicated business, that pharmaceutical and insurance execs make much more. Also, board compensation committees determine the payout, considering salaries at comparable institutions as well as the hospital’s financial performance.
One obvious reason for the regulatory tolerance is that hospital systems are major employers — the largest in many states (including Massachusetts, Pennsylvania, Minnesota, Arizona, and Delaware). They are big-time lobbying forces and major donors in Washington and in state capitals.
But some patients have had enough: In a suit brought by a local school board, a judge last year declared that four Pennsylvania hospitals in the Tower Health system had to pay property taxes because its executive pay was “eye popping” and it demonstrated “profit motives through actions such as charging management fees from its hospitals.”
A 2020 Government Accountability Office report chided the IRS for its lack of vigilance in reviewing nonprofit hospitals’ community benefit and recommended ways to “improve IRS oversight.” A follow-up GAO report to Congress in 2023 said, “IRS officials told us that the agency had not revoked a hospital’s tax-exempt status for failing to provide sufficient community benefits in the previous 10 years” and recommended that Congress lay out more specific standards. The IRS declined to comment for this column.
Attorneys general, who regulate charity at the state level, could also get involved. But, in practice, “there is zero accountability,” West said. “Most nonprofits live in fear of the AG. Not hospitals.”
Today’s big hospital systems do miraculous, lifesaving stuff. But they are not channeling Mother Teresa. Maybe it’s time to end the community benefit charade for those that exploit it, and have these big businesses pay at least some tax. Communities could then use those dollars in ways that directly benefit residents’ health.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Okra vs Rhubarb – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing okra to rhubarb, we picked the okra.
Why?
It wasn’t close:
In terms of macros, okra has more fiber, carbs, and protein, making it the most nutritionally dense option in this category.
In the category of vitamins, okra has more of vitamins A, B1, B2, B3, B5, B6, B7. B9, C, E, and K, while rhubarb is not higher in any vitamins—a complete win for okra.
Looking at minerals, okra has more copper, iron, magnesium, manganese, phosphorus potassium, and zinc, while rhubarb has (slightly) more calcium and selenium. Another easy win for okra.
In other considerations, both are good sources of polyphenols, but okra has more, scoring it a fourth win in a row.
Adding up the sections makes for a clear overall win for okra, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: