

Is It Dementia?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Spot The Signs (Because None Of Us Are Immune)
Dementia affects increasingly many people, and unlike a lot of diseases, it disproportionately affects people in wealthy industrialized nations.
There are two main reasons for this:
- Longevity (in poorer countries, more people die of other things sooner; can’t get age-related cognitive decline if you don’t age)
- Lifestyle (in the age of convenience, it has never been easier to live an unhealthy lifestyle)
The former is obviously no bad thing for those of us lucky enough to be in wealthier countries (though even in such places, good healthcare access is of course sadly not a given for all).
The latter, however, is less systemic and more epidemic. But it does cut both ways:
- An unhealthy lifestyle is much easier here, yes
- A healthier lifestyle is much easier here, too!
This then comes down to two factors in turn:
- Information: knowing about dementia, what things lead to it, what to look out for, what to do
- Motivation: priorities, and how much attention we choose to give this matter
So, let’s get some information, and then give it our attention!
More than just memory
It’s easy to focus on memory loss, but the four key disabilities directly caused by dementia (each person may not get all four), can be remembered by the mnemonic: “AAAA!”
No, somebody didn’t just murder your writer. It’s:
- Amnesia: memory loss, in one or more of its many forms
- e.g. short term memory loss, and/or inability to make new memories
- Aphasia: loss of ability to express oneself, and/or understand what is expressed
- e.g. “More people have been to Berlin than I have”
- Or even less communication-friendly, Broca’s (Expressive) Aphasia and Wernicke’s (Receptive) Aphasia
- Apraxia: loss of ability to do things, through no obvious physical disability
- e.g. staring at the bathroom mirror wondering how to brush one’s teeth
- Agnosia: loss of ability to recognize things
- e.g. prosopagnosia, also called face-blindness.
If any of those seem worryingly familiar, be aware that while yes, it could be a red flag, what’s most important is patterns of these things.
Another difference between having a momentary brainlapse and having dementia might be, for example, the difference between forgetting your keys, and forgetting what keys do or how to use one.
That said, some are neurological deficits that may show up quite unrelated to dementia, including most of those given as examples above. So if you have just one, then that’s probably worthy of note, but probably not dementia.
Writer’s anecdote: I have had prosopagnosia all my life. To give an example of what that is like and how it’s rather more than just “bad with faces”…
Recently I saw my neighbor, and I could tell something was wrong with her face, but I couldn’t put my finger on what it was. Then some moments later, I realized I had mistaken her hat for her face. It was a large beanie with a panda design on it, and that was facelike enough for me to find myself looking at the wrong face.
Subjective memory matters as much as objective
Objective memory tests are great indicators of potential cognitive decline (or improvement!), but even a subjective idea of having memory problems, that one’s memory is “not as good as it used to be”, can be an important indicator too:
Subjective memory may be marker for cognitive decline
And more recently:
If your memory feels like it’s not what it once was, it could point to a future dementia risk
If you’d like an objective test of memory and other cognitive impairments, here’s the industry’s gold standard test (it’s free):
SAGE: A Test to Detect Signs of Alzheimer’s and Dementia
(The Self-Administered Gerocognitive Exam (SAGE) is designed to detect early signs of cognitive, memory or thinking impairments)
There are things that can look like dementia that aren’t
A person with dementia may be unable to recognize their partner, but hey, this writer knows that feeling very well too. So what sets things apart?
More than we have room for today, but here’s a good overview:
What are the early signs of dementia, and how does it differ from normal aging?
Want to read more?
You might like our previous article more specifically about reducing Alzheimer’s risk:
Reducing Alzheimer’s Risk Early!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What happens in my brain when I get a migraine? And what medications can I use to treat it?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine is many things, but one thing it’s not is “just a headache”.
“Migraine” comes from the Greek word “hemicrania”, referring to the common experience of migraine being predominantly one-sided.
Some people experience an “aura” preceding the headache phase – usually a visual or sensory experience that evolves over five to 60 minutes. Auras can also involve other domains such as language, smell and limb function.
Migraine is a disease with a huge personal and societal impact. Most people cannot function at their usual level during a migraine, and anticipation of the next attack can affect productivity, relationships and a person’s mental health.

Francisco Gonzelez/Unsplash What’s happening in my brain?
The biological basis of migraine is complex, and varies according to the phase of the migraine. Put simply:
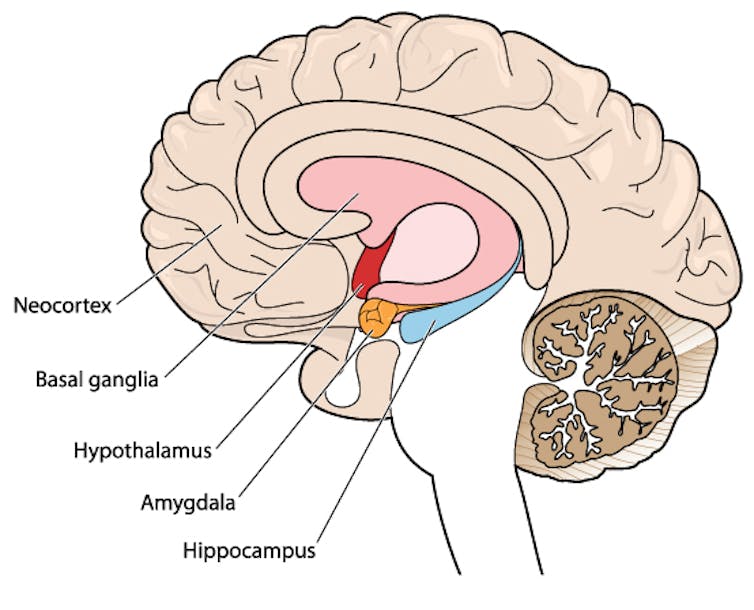
The earliest phase is called the prodrome. This is associated with activation of a part of the brain called the hypothalamus which is thought to contribute to many symptoms such as nausea, changes in appetite and blurred vision.
The hypothalamus is shown here in red. Blamb/Shutterstock Next is the aura phase, when a wave of neurochemical changes occur across the surface of the brain (the cortex) at a rate of 3–4 millimetres per minute. This explains how usually a person’s aura progresses over time. People often experience sensory disturbances such as flashes of light or tingling in their face or hands.
In the headache phase, the trigeminal nerve system is activated. This gives sensation to one side of the face, head and upper neck, leading to release of proteins such as CGRP (calcitonin gene-related peptide). This causes inflammation and dilation of blood vessels, which is the basis for the severe throbbing pain associated with the headache.
Finally, the postdromal phase occurs after the headache resolves and commonly involves changes in mood and energy.
What can you do about the acute attack?
A useful way to conceive of migraine treatment is to compare putting out campfires with bushfires. Medications are much more successful when applied at the earliest opportunity (the campfire). When the attack is fully evolved (into a bushfire), medications have a much more modest effect.
Aspirin
For people with mild migraine, non-specific anti-inflammatory medications such as high-dose aspirin, or standard dose non-steroidal medications (NSAIDS) can be very helpful. Their effectiveness is often enhanced with the use of an anti-nausea medication.
Triptans
For moderate to severe attacks, the mainstay of treatment is a class of medications called “triptans”. These act by reducing blood vessel dilation and reducing the release of inflammatory chemicals.
Triptans vary by their route of administration (tablets, wafers, injections, nasal sprays) and by their time to onset and duration of action.
The choice of a triptan depends on many factors including whether nausea and vomiting is prominent (consider a dissolving wafer or an injection) or patient tolerability (consider choosing one with a slower onset and offset of action).
As triptans constrict blood vessels, they should be used with caution (or not used) in patients with known heart disease or previous stroke.
Triptans should be used cautiously in patients with heart disease. CDC/Unsplash Gepants
Some medications that block or modulate the release of CGRP, which are used for migraine prevention (which we’ll discuss in more detail below), also have evidence of benefit in treating the acute attack. This class of medication is known as the “gepants”.
Gepants come in the form of injectable proteins (monoclonal antibodies, used for migraine prevention) or as oral medication (for example, rimegepant) for the acute attack when a person has not responded adequately to previous trials of several triptans or is intolerant of them.
They do not cause blood vessel constriction and can be used in patients with heart disease or previous stroke.
Ditans
Another class of medication, the “ditans” (for example, lasmiditan) have been approved overseas for the acute treatment of migraine. Ditans work through changing a form of serotonin receptor involved in the brain chemical changes associated with the acute attack.
However, neither the gepants nor the ditans are available through the Pharmaceutical Benefits Scheme (PBS) for the acute attack, so users must pay out-of-pocket, at a cost of approximately A$300 for eight wafers.
What about preventing migraines?
The first step is to see if lifestyle changes can reduce migraine frequency. This can include improving sleep habits, routine meal schedules, regular exercise, limiting caffeine intake and avoiding triggers such as stress or alcohol.
Despite these efforts, many people continue to have frequent migraines that can’t be managed by acute therapies alone. The choice of when to start preventive treatment varies for each person and how inclined they are to taking regular medication. Those who suffer disabling symptoms or experience more than a few migraines a month benefit the most from starting preventives.
Some people will take medicines to prevent migraines. Tbel Abuseridze/Unsplash Almost all migraine preventives have existing roles in treating other medical conditions, and the physician would commonly recommend drugs that can also help manage any pre-existing conditions. First-line preventives include:
- tablets that lower blood pressure (candesartan, metoprolol, propranolol)
- antidepressants (amitriptyline, venlafaxine)
- anticonvulsants (sodium valproate, topiramate).
Some people have none of these other conditions and can safely start medications for migraine prophylaxis alone.
For all migraine preventives, a key principle is starting at a low dose and increasing gradually. This approach makes them more tolerable and it’s often several weeks or months until an effective dose (usually 2- to 3-times the starting dose) is reached.
It is rare for noticeable benefits to be seen immediately, but with time these drugs typically reduce migraine frequency by 50% or more.
‘Nothing works for me!’
In people who didn’t see any effect of (or couldn’t tolerate) first-line preventives, new medications have been available on the PBS since 2020. These medications block the action of CGRP.
The most common PBS-listed anti-CGRP medications are injectable proteins called monoclonal antibodies (for example, galcanezumab and fremanezumab), and are self-administered by monthly injections.
These drugs have quickly become a game-changer for those with intractable migraines. The convenience of these injectables contrast with botulinum toxin injections (also effective and PBS-listed for chronic migraine) which must be administered by a trained specialist.
Up to half of adolescents and one-third of young adults are needle-phobic. If this includes you, tablet-form CGRP antagonists for migraine prevention are hopefully not far away.
Data over the past five years suggest anti-CGRP medications are safe, effective and at least as well tolerated as traditional preventives.
Nonetheless, these are used only after a number of cheaper and more readily available first-line treatments (all which have decades of safety data) have failed, and this also a criterion for their use under the PBS.
Mark Slee, Associate Professor, Clinical Academic Neurologist, Flinders University and Anthony Khoo, Lecturer, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Seven Steps to Managing Your Memory – by Dr. Andrew Budson & Dr. Maureen O’Connor
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, what this is not: a “how to improve your memory” book of the kind marketed to students and/or people who want to do memory-themed party tricks.
What this book actually is: exactly what the title and subtitle claim it to be: seven steps to managing your memory: what’s normal, what’s not, and what to do about it.
Drs. Budson & O’Connor cover:
- which memory errors can (and usually do) happen at any age
- how memory changes with normal aging, and
- what kinds of memory problems are not normal.
One thing that sets this book aside from a lot of its genre is that it also covers which kinds of memory loss are reversible—and, where appropriate, what can be undertaken to effect such a reversal.
The authors talk about what things have (and what things haven’t!) been shown to strengthen memory and reduce cognitive decline, and in the worst case scenario, what medications can help against Alzheimer’s disease and other dementias.
The style is halfway between pop-science and a science textbook. The structure of the book, with its headings, subheadings, bullet points, summaries, etc, helps the reader to process and remember the information.
Bottom line: if you’d like to get on top of managing your memory before you forget, then this book is for you.
Share This Post
-

5 Movements You’ll Wish You’d Known Sooner
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Alisa Zuravskaja, mobility coach, shows us why:
Best for mobility, best against pain
These movements are what’s needed for good mobility (range of motion, flexibility, strength, stability) while also being a top-tier way of combatting pain, due to what they do for the body’s natural functions.
Specifically, the exercises are intended to build on one another, beginning with neck stability, then restoring upper-back rotation, activating your glutes, improving hip control, and finally reducing hamstring and posterior-chain tightness:
- Chin tucks: stand tall, bring your chin slightly forwards, then push it straight back to create a double chin while keeping your head level, and follow with slow shoulder shrugs by lifting your shoulders towards your ears and lowering them under control.
- Quadruped thoracic rotations: start on all fours with one hand on the floor and the other extended to the side, rotate through your upper back to lift the arm towards the ceiling while following it with your eyes, then return to the start position.
- Glute bridges: lie on your back with your knees bent and feet flat, squeeze your glutes before lifting your hips, hold briefly at the top, then lower slowly while keeping the effort in your glutes rather than your lower back.
- Hip CARs (controlled articular rotations): stand or kneel, lift one knee and slowly move your hip through its fullest circular range while keeping your spine and upper body still, then repeat in both directions on each side.
- Sciatic nerve flossing: lie on your back with one knee bent and your foot flat on the floor, raise the other leg towards the ceiling, then gently flex and point your foot or make slow ankle circles, to glide the sciatic nerve through its range of motion.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Best Mobility Drills For Posture & Pain Relief
Take care!
Share This Post






-
What is wabi-sabi? Will this Japanese philosophy make me happy?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The ceramic bowl with an uneven glaze. The teacup mended with gold lacquer.
The images are calming and attractive.
They are said to reflect wabi-sabi – a Japanese aesthetic often summarised in the West as valuing imperfection, impermanence and incompleteness.
And wabi-sabi is having a moment on social media. It’s linked to everything from interior design to makeup trends and happiness.
So can wabi-sabi improve your wellbeing? Here’s what the psychological evidence says.
Marco Montalti/Getty What is wabi-sabi?
At its core, wabi-sabi, as it is commonly understood in the West, rests on three simple ideas: things are flawed, things change, and things are never fully finished.
There isn’t much scientific research on wabi-sabi itself. You won’t find clinical trials testing the effects of “becoming wabi-sabi”.
But the ideas behind wabi-sabi reflect several well-established principles in psychology – responding kindly to imperfection, accepting change, and loosening rigid perfectionism.
Imperfection and self-compassion
Wabi-sabi begins with imperfection. Instead of disguising cracks, it incorporates them. The flaw becomes part of the object’s character, not proof it is worthless.
In psychological terms, this resembles self-compassion – responding to your own mistakes or shortcomings with warmth and care, rather than harsh self-criticism.
Self-compassion does not pretend errors do not exist. It changes how we relate to them.
Research consistently shows people who are more self-compassionate report lower anxiety and depression and greater wellbeing.
When interventions help people develop this skill, their mental health often improves.
Like the repaired bowl, the person is not defined by the crack. The crack is acknowledged and becomes part of their story.
Impermanence and acceptance
Wabi-sabi also reminds us nothing lasts. Everything changes.
Some of our distress comes not only from change itself, but from insisting things should not change. We want relationships to stay the same. We want our bodies not to age. We want plans to unfold exactly as expected.
When reality shifts and we resist it, the struggle intensifies.
In psychology, acceptance means allowing thoughts, emotions and changes to occur without constantly trying to push them away or control them.
Modern therapies, such as “acceptance and commitment therapy”, teach this skill because resisting unavoidable experiences often intensifies distress.
Mindfulness – paying attention to what is happening right now without immediately judging or trying to fix it – is one way people practise acceptance.
Seen this way, wabi-sabi’s focus on impermanence is not passive resignation. It reflects a practical insight. When change is unavoidable, reducing the fight against it can reduce suffering.
Incompleteness and perfectionism
The third idea in wabi-sabi is incompleteness. Nothing is ever fully finished.
This runs counter to a form of perfectionism psychologists call clinical perfectionism. This is not simply wanting to do well. It occurs when people base their self-worth on meeting extremely high standards and respond to falling short with harsh self-criticism.
Research links this form of perfectionism with anxiety and depression.
Self-compassion may offer a similar shift in perspective. When people respond to setbacks with understanding rather than harsh self-criticism, the psychological cost of imperfection is reduced.
Wabi-sabi does not reject effort or aspiration. It questions the belief that you must be flawless before you are acceptable.
Imperfection and meaning
I recently wrote that meaning does not emerge from perfectly executed life plans. It grows from repeated, worthwhile action, often messy, unfinished and imperfect. Wabi-sabi echoes this.
If we wait for flawless conditions before acting, we may wait indefinitely. The project will never feel polished enough. The timing will never seem quite right.
But wellbeing is strongly shaped by what we do repeatedly, especially when those actions align with our values. From this perspective, imperfection is not an obstacle to meaning. It is often the setting in which meaning develops.
The repaired bowl is still used.
The musician keeps playing after a broken string.
The parent apologises and tries again.
Imperfection and connection
There is also a social dimension.
Research shows vulnerability can strengthen relationships. In other words, when people acknowledge mistakes or limitations, they are often seen as more relatable and trustworthy.
Presenting as flawless can create distance. Allowing cracks to be visible can create connection.
Wabi-sabi offers a simple image for this. The crack is not hidden. It becomes part of the story.
Wabi-sabi has its limits
It is important not to overstate what wabi-sabi offers.
There is no evidence adopting it as a named philosophy guarantees happiness. It is not a treatment for depression. And acceptance does not mean tolerating injustice or giving up on improvement.
But at its heart, wabi-sabi questions whether our expectations have become too polished.
It asks whether some of our expectations – of our bodies, our productivity, our relationships – have become so polished they leave no room for being human.
How can I use it?
Wabi-sabi may not offer something entirely new. But it captures, in a single image, several psychological skills research suggests can help people live well.
It invites us to:
- respond to our flaws with kindness
- accept that change is normal
- loosen rigid standards
- act in line with our values despite imperfection
- connect with others by showing our humanity.
Wabi-sabi is not a shortcut to happiness. But as both an image and a practice, it reflects a grounded psychological idea.
Wellbeing is less about erasing the cracks, and more about continuing to live, act and connect with them visible.
Trevor Mazzucchelli, Associate Professor of Clinical Psychology, Curtin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Beetroot vs Parsnips – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing beetroot to parsnips, we picked the parsnips.
Why?
Beetroot definitely has its fine merits, but…
In terms of macros, beetroot has very slightly more protein, while parsnips have nearly 2x the fiber and a little under 2x the carbs, which, weighting things for importance and statistical significance, we’d say the fiber comes out as the most relevant figure, which tips this round to parsnips. An argument could be made for beetroot or a tie, though.
In the category of vitamins, beetroot has more vitamin B9, while parsnips have more of vitamins B1, B2, B3, B5, B6, B7, C, E, and K, winning this round by a country mile.
Looking at minerals, beetroot has a tiny bit more iron, while parsnips have notably more calcium, copper, magnesium, manganese, phosphorus, potassium, selenium, and zinc, for another overwhelming win in this round.
In other considerations, beetroot has a generous betalain content and especially betanin, winning this round.
Adding up the sections makes for a compelling overall win for parsnips, but by all means enjoy either or both, as diversity is great!
Want to learn more?
You might like:
Beetroot For More Than Just Your Blood Pressure
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

4 Critical Things Female Runners Should Know
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When it comes to keeping up performance in the face of menopause, Shona Hendricks has advice:
Don’t let menopause run you down
- Prioritize recovery! Overtraining without adequate recovery just leads to decreased performance in the long term, and remember, you may not recover as quickly as you used to. If you’re still achey from your previous run, give it another day, or at least make it a lighter run.
- Slow down in easy and long runs! This isn’t “taking the easy way out”; it will improve your overall performance, reducing muscle damage, allowing for quicker recovery and ultimately better fitness gains.
- Focus on nutrition! And that means carbs too. A lot of people fighting menopausal weight gain reduce their intake of food, but without sufficient energy availability, you will not be able to run well. In particular, carbohydrates are vital for energy. Consume them sensibly and with fiber and proteins and fats rather than alone, but do consume them.
- Incorporate strength training! Your run is not “leg day” by itself. Furthermore, do whole-body strength training, to prevent injuries and improve overall performance. A strong core is particularly important.
For more on each of these (and some bonus comments about mobility training for runners), enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:



