Antidepressants: Personalization Is Key!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Antidepressants: Personalization Is Key!
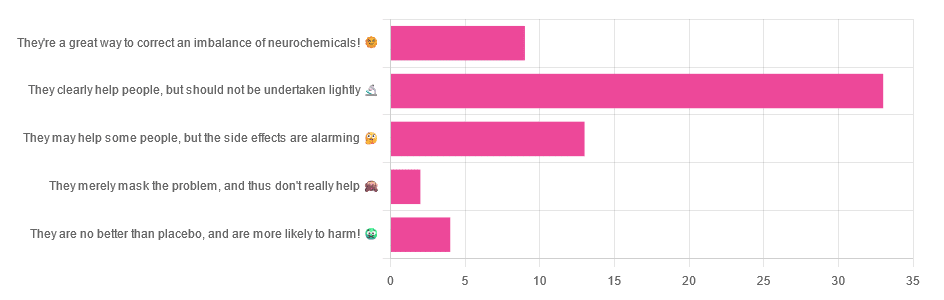
Yesterday, we asked you for your opinions on antidepressants, and got the above-depicted, below-described, set of responses:
- Just over half of respondents said “They clearly help people, but should not be undertaken lightly”
- Just over a fifth of respondents said “They may help some people, but the side effects are alarming”
- Just under a sixth of respondents said “They’re a great way to correct an imbalance of neurochemicals”
- Four respondents said “They are no better than placebo, and are more likely to harm”
- Two respondents said “They merely mask the problem, and thus don’t really help”
So what does the science say?
❝They are no better than placebo, and are more likely to harm? True or False?❞
True or False depending on who you are and what you’re taking. Different antidepressants can work on many different systems with different mechanisms of action. This means if and only if you’re not taking the “right” antidepressant for you, then yes, you will get only placebo benefits:
- Placebo Effect in the Treatment of Depression and Anxiety ← randomly assigned antidepressants are, shockingly, luck of the draw in usefulness
- Antidepressants versus placebo in major depression: an overview ← “wow this science is messy”
- Comparative efficacy and acceptability of 21 antidepressant drugs: a systematic review and network meta-analysis ← “oh look, it makes a difference which antidepressant we give to people”
Rather than dismissing antidepressants as worthless, therefore, it is a good idea to find out (by examination or trial and error) what kind of antidepressant you need, if you indeed do need such.
Otherwise it is like getting a flu shot and being surprised when you still catch a cold!
❝They merely mask the problem, and thus don’t really help: True or False?❞
False, categorically.
The problem in depressed people is the depressed mood. This may be influenced by other factors, and antidepressants indeed won’t help directly with those, but they can enable the person to better tackle them (more on this later).
❝They may help some people, but the side-effects are alarming: True or False?❞
True or False depending on more factors than we can cover here.
Side-effects vary from drug to drug and person to person, of course. As does tolerability and acceptability, since to some extent these things are subjective.
One person’s dealbreaker may be another person’s shrugworthy minor inconvenience at most.
❝They’re a great way to correct an imbalance of neurochemicals: True or False?❞
True! Contingently.
That is to say: they’re a great way to correct an imbalance of neurochemicals if and only if your problem is (at least partly) an imbalance of neurochemicals. If it’s not, then your brain can have all the neurotransmitters it needs, and you will still be depressed, because (for example) the other factors* influencing your depression have not changed.
*common examples include low self-esteem, poor physical health, socioeconomic adversity, and ostensibly bleak prospects for the future.
For those for whom the problem is/was partly a neurochemical imbalance and partly other factors, the greatest help the antidepressants give is getting the brain into sufficient working order to be able to tackle those other factors.
Want to know more about the different kinds?
Here’s a helpful side-by-side comparison of common antidepressants, what type they are, and other considerations:
Mind | Comparing Antidepressants
Want a drug-free approach?
You might like our previous main feature:
The Mental Health First-Aid That You’ll Hopefully Never Need
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A Urologist Explains Edging: What, Why, & Is It Safe?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Edging” is the practice of intentionally delaying orgasm, which can be enjoyed by anyone, with a partner or alone.
On the edge
Question: why?
Answer: the more tension is built up, the stronger the orgasm can be at the end of it. And, even before then, pleasure along the way is pleasure along the way, which is generally considered a good thing—especially for any (usually but not always women, for hormonal and social reasons) who find it difficult to orgasm. It’s also a great way to experiment and learn more about one’s own body and/or that of one’s partner(s), personal responses, and so forth. Also, for any (usually but not always men, for hormonal reasons) who find they usually orgasm sooner than they’d like, it’s a great way to change that, if changing that is what’s wanted.
Bonus answer: for some (usually but not always men, for hormonal reasons) who find they have an uncomfortable slump in mood after orgasm, that can simply be skipped entirely, postponed for another time, etc, with pleasure being derived from the sexual activity rather than orgasm. That way, there’s a lasting dopamine high, with no prolactin crash afterwards ← this is very much tied to male hormones, by the way. If you have female hormones, there’s usually no prolactin crash either way, and instead, the post-orgasm spike in oxytocin is stronger, and a wave of serotonin makes the later decline of dopamine much more gentle.
Question: can it cause any problems?
Answer: yep! Or rather, subjectively, it may be considered so—this is obviously a personal matter and your mileage may vary. The main problem it may cause is that if practised habitually, it may result in greater difficulty achieving orgasm, simply because the body has got used to “ok, when we do this (sex/masturbation), we are in no particular rush to do that (orgasm)”. So whether not this would be a worry for you is down to any given individual. Lastly, if your intent was a long edging session with an orgasm at the end and then something happened to interrupt that, then your orgasm may be unintentionally postponed to another time, which again, may be more or less of an issue depending on your feelings about that.
For more on these things including advice on how to try it, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Mythbusting The Big O ← 10almonds main feature on orgasms, health, and associated myths
- Come Together: The Science (and Art) of Creating Lasting Sexual Connections – by Dr. Emily Nagoski
- Better Sex Through Mindfulness: How Women Can Cultivate Desire – by Dr. Lori Brotto
Take care!
Share This Post
-

Continuous Glucose Monitors Without Diabetes: Pros & Cons
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The “Glucose Goddess”, biochemist Jessie Inchauspé, gives us the low-down:
Knowledge is power (but watch out)
A continuous glucose monitor (CGM) is a device that continually monitors glucose levels, without the need to stab one’s finger every few hours to test blood.
It was designed for diabetics, especially for those with Type 1 Diabetes, where around-the-clock monitoring is necessary for appropriate insulin dosing.
For non-diabetics, they can be a good way of learning what our body’s response to various foods and activities is like, the better to be able to tweak our habits to avoid undue glucose spikes (which are harmful for our pancreas, liver, heart, brain, kidneys, and more).
How it works: there’s a sensor that sits on the arm (or elsewhere, but the arm is a popular placement) with a little probe that goes under the skin. It’s applied using a device that inserts it automatically using a needle (you only need to press a button, you don’t need to guide the needle yourself); the needle then retracts, leaving the soft, flexible probe in place. Having been attached, that sensor can now stay in place for 2 weeks (usually; depends on brand, but for example FreeStyle Libre, the most popular brand, the sensors last 2 weeks), and yes, it’s fine to bathe/shower/etc with it. When you want an update from your CGM, you scan it with your phone (or you can buy a dedicated reader, but that is more expensive and unnecessary), and it uploads the data since your last scan.
Pros: it’s convenient and gives a lot of data, so even if you only use it for a short period of time (for example, a month) you can get a very good idea of what affects your blood sugar levels and how. Also, because of the constant nature of the monitoring, it helps avoid accidental sample bias of the kind that can occur with manual testing, by testing a little too soon or too late, and missing a spike/dip.
Cons: it can be expensive, depending on where you live and what options are available for you locally, so you might not want to do it long-term (since that would require buying two sensors per month). It’s also, for all its wealth of data, slightly less accurate than fingerprick testing—that’s because it takes an interstitial reading instead of directly from the blood. For this reason, if you test both ways, you may find a discrepancy of about 3mg/dL. Given that the healthy range is about 70–140mg/dL, a discrepancy of 3mg/dL is probably not going to be important, but it is a thing to mention can (and probably will) happen.
Patterns to bear in mind (with any kind of blood sugar monitoring):
- Dawn phenomenon: a natural glucose rise upon waking.
- Exercise-induced spikes (normal due to energy demands).
- Fat in meals slowing glucose absorption.
- Different foods can sometimes cause a double-wave after dinner (because glucose from different foods is absorbed differently, and/or different foods affect insulin response independent of glucose)
- Steep, rapid spikes that are more harmful than gradual, sustained increases.
- Vitamin C spikes: temporary chemical interference with the sensor, not actual glucose rises.
- Nighttime glucose dips (often false readings caused by sleeping position).
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
10 Ways To Balance Blood Sugars
Take care!
Share This Post
-
Red-dy For Anything Polyphenol Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
So, you’ve enjoyed your Supergreen Superfood Salad Slaw, and now you’re ready for another slice of the rainbow. Pigments in food aren’t just for decoration—they each contain unique benefits! Today’s focus is on some red foods that, combined, make a deliciously refreshing salad that’s great for the gut, heart, and brain.
You will need
- 1 cup crème fraîche or sour cream (if vegan, use our Plant-Based Healthy Cream Cheese recipe, and add the juice of 1 lime)
- ½ small red cabbage, thinly sliced
- 1 red apple, cored and finely chopped
- 1 red onion, thinly sliced
- 10 oz red seedless grapes, halved
- 10 oz red pomegranate seeds
- 1 tsp red chili flakes
Method
(we suggest you read everything at least once before doing anything)
1) Combine all the red ingredients in a big bowl.
2) Add the crème fraîche and mix gently but thoroughly.
3) If you have time, let it sit in the fridge for 48 hours before enjoying, as its colors will intensify and its polyphenols will become more bioavailable. But if you want/need, you can serve immediately; that’s fine too.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Resveratrol & Healthy Aging
- Tasty Polyphenols For Your Heart And Brain
- Pomegranate vs Cherries – Which is Healthier?
- Capsaicin For Weight Loss And Against Inflammation
Take care!
Share This Post


Related Posts
-

Healthy Mind In A Healthy Body
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The 8-minute piece of music “Weightless” by Marconi was created scientifically to lower the heart rate and relax the listener. How did they do it? You can read the British Academy of Sound Therapy’s explanation of the methodology here, but important results of the study were:
- “Weightless” was able to induce greater relaxation levels than a massage (increase of 6%).
- “Weightless” also induced an 11% increase in relaxation over all other relaxing music tracks in the study.
- “Weightless” was also subjectively rated as more relaxing than any other music by all the participants.
Try it for yourself!
Click Here If The Embedded Video Doesn’t Load Automatically!
Isn’t that better? Whenever you’re ready, read on…
Today we’re going to share a technique for dealing with difficult emotions. The technique is used in Cognitive Behavioral Therapy (CBT), and Dialectical Behavior Therapy (DBT), and it’s called RAIN:
- Recognizing: ask yourself “what is it that I’m feeling?”, and put a name to it. It could be anger, despair, fear, frustration, anxiety, overwhelm etc.
- Accepting: “OK, so, I’m feeling ________”. There’s no point in denying it, or being defensive about it, these things won’t help you. For now, just accept it.
- Investigating: “Why am I feeling ________?” Maybe there is an obvious reason, maybe you need to dig for a reason—or dig deeper for the real reason. Most bad feelings are driven by some sort of fear or insecurity, so that can be a good avenue for examination. Important: your feelings may be rational or irrational. That’s fine. This is a time for investigating, not judging.
- Non-Identification: not making whatever it is you’re feeling into a part of you. Once you get too attached to “I am jealous”, “I am angry”, “I am sad” etc, it can be difficult to manage something that has become a part of your personality; you’ll defend your jealousy, anger, sadness etc rather than tackle it.
As a CBT tool, this is something you can do for yourself at any time. It won’t magically solve your problems, but it can stop you from spiralling into a state of crisis, and get you back on a more useful track.
As a DBT tool, to give this its full strength, ideally now you will communicate what you’re feeling, to somebody you trust, perhaps a partner or friend, for instance.
Humans are fundamentally social creatures, and we achieve our greatest strengths when we support each other—and that also means sometimes seeking and accepting support!
Do you have a good technique you’d like to share? Reply to this email and let us know!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Vital Aspects of Holistic Wellness
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
This newsletter has been growing a lot lately, and so have the questions/requests, and we love that! In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
Q: I am interested in the following: Aging, Exercise, Diet, Relationships, Purpose, Lowering Stress
You’re going to love our Psychology Sunday editions of 10almonds! You might like some of these…
- Relationships: Seriously Useful Communication Skills!
- Purpose: Are You Flourishing? (There’s a Scale)
- Managing stress: Lower Your Cortisol! (Here’s Why & How)
- Also about managing stress: Sunday Stress-Buster
- Also applicable to stress: How To Set Your Anxiety Aside
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
For Many Rural Women, Finding Maternity Care Outweighs Concerns About Abortion Access
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
BAKER CITY, Ore. — In what has become a routine event in rural America, a hospital maternity ward closed in 2023 in this small Oregon town about an hour from the Idaho border.
For Shyanne McCoy, 23, that meant the closest hospital with an obstetrician on staff when she was pregnant was a 45-mile drive away over a mountain pass.
When McCoy developed symptoms of preeclampsia last January, she felt she had the best chance of getting the care she needed at a larger hospital in Boise, Idaho, two hours away. She spent the final week of her pregnancy there, too far from home to risk leaving, before giving birth to her daughter.
Six months later, she said it seems clear to her that the health care needs of rural young women like her are largely ignored.
For McCoy and others, figuring out how to obtain adequate care to safely have a baby in Baker City has quickly eclipsed concerns about another medical service lacking in the area: abortion. But in Oregon and elsewhere in the country, progressive lawmakers’ attempts to expand abortion access sometimes clash with rural constituencies.
Oregon is considered one of the most protective states in the country when it comes to abortion. There are no legal limits on when someone can receive an abortion in the state, and the service is covered by its Medicaid system. Still, efforts to expand access in the rural, largely conservative areas that cover most of the state have encountered resistance and incredulity.
It’s a divide that has played out in elections in such states as Nevada, where voters passed a ballot measure in November that seeks to codify abortion protections in the state constitution. Residents in several rural counties opposed the measure.
In Oregon, during the months just before the Baker City closure was announced, Democratic state lawmakers were focused on a proposed pilot program that would launch two mobile reproductive health care clinics in rural areas. The bill specified that the van-based clinics would include abortion services.
State Rep. Christine Goodwin, a Republican from a southwestern Oregon district, called the proposal the “latest example” of urban legislators telling rural leaders what their communities need.
The mobile health clinic pilot was eventually removed from the bill that was under discussion. That means no new abortion options in Oregon’s Baker County — and no new state-funded maternity care either.
“I think if you expanded rural access in this community to abortions before you extended access to maternal health care, you would have an uprising on your hands,” said Paige Witham, 27, a member of the Baker County health care steering committee and the mother of two children, including an infant born in October.
A study published in JAMA in early December that examined nearly 5,000 acute care hospitals found that by 2022, 52% of rural hospitals lacked obstetrics care after more than a decade of unit closures. The health implications of those closures for young women, the population most likely to need pregnancy care, and their babies can be significant. Research has shown that added distance between a patient and obstetric care increases the likelihood the baby will be admitted to a neonatal intensive care unit, or NICU.
Witham said that while she does not support abortion, she believes the government should not “legislate it away completely.” She said that unless the government provides far more support for young families, like free child care and better mental health care, abortion should remain legal.
Conversations with a liberal school board member, a moderate owner of a timber company, members of Baker City’s Republican Party chapter, a local doula, several pregnant women, and the director of the Baker County Health Department — many of whom were not rigidly opposed to abortion — all turned up the same answer: No mobile clinics offering abortions here, please.
Kelle Osborn, a nurse supervisor for the Baker County Health Department, loved the idea of a mobile clinic that would provide education and birth control services to people in outlying areas. She was less thrilled about including abortion services in a clinic on wheels.
“It’s not something that should just be handed out from a mobile van,” she said of abortion services. She said people in her conservative rural county would probably avoid using the clinics for anything if they were understood to provide abortion services.
Both Osborn and Meghan Chancey, the health department’s director, said they would rank many health care priorities higher, including the need for a general surgeon, an ICU, and a dialysis clinic.
Nationally, reproductive health care services of all types tend to be limited for people in rural areas, even within states that protect abortion access. More than two-thirds of people in “maternity care deserts” — all of which are in rural counties — must drive more than a half-hour to get obstetric care, according to a 2024 March of Dimes report. For people in the Southern states where lawmakers installed abortion bans, abortion care can be up to 700 miles away, according to a data analysis by Axios.
Nathan Defrees grew up in Baker City and has practiced medicine here since 2017. He works for a family medicine clinic. If a patient asks about abortion, he provides information about where and how one can be obtained, but he doesn’t offer abortions himself.
“There’s not a lot of anonymity in small towns for physicians who provide that care,” he said. “Many of us aren’t willing to sacrifice the rest of our career for that.”
He also pointed to the small number of patients requesting the service locally. Just six people living in Baker County had an abortion in 2023, according to data from the Oregon Department of Public Health. Meanwhile, 125 residents had a baby that year.
A doctor with obstetric training living in another rural part of the state has chosen to quietly provide early-stage abortions when asked. The doctor, concerned for their family’s safety in the small, conservative town where they live, asked not to be identified.
The idea that better access to abortion is not needed in rural areas seems naive, the doctor said. People most in need of abortion often don’t have access to any medical service not already available in town, the doctor pointed out. The first patient the doctor provided an abortion for at the clinic was a meth user with no resources to travel or to manage an at-home medication abortion.
“It seemed entirely inappropriate for me to turn her away for care I had the training and the tools to do,” the doctor said.
Defrees said it has been easier for Baker County residents to get an abortion since the U.S. Supreme Court overturned Roe v. Wade.
A new Planned Parenthood clinic in Ontario, Oregon, 70 miles away in neighboring Malheur County, was built primarily to provide services to people from the Boise metro area, but it also created an option for many living in rural eastern Oregon.
Idaho is one of the 16 states with near-total bans on abortion. Like many states with bans, Idaho has struggled to maintain its already small fleet of fetal medicine doctors. The loss of regional expertise touches Baker City, too, Defrees said.
For example, he said, the treatment plan for women who have a desired pregnancy but need a termination for medical reasons is now far less clear. “It used to be those folks could go to Boise,” he said. “Now they can’t. That does put us in a bind.”
Portland is the next closest option for that type of care, and that means a 300-mile drive along a set of highways that can be treacherous in winter.
“It’s a lot scarier to be pregnant now in Baker City than it ever has been,” Defrees said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: