The Big Book of Kombucha – by Hannah Crum & Alex LaGory
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you’ve been thinking “I should get into kombucha”, then this is the universe prompting you, because with in this book’s 400 pages is all the information you need and more.
Because, it’s understandable to be wary when starting out, from “what if my jar explodes” to “what if I poison my family”, but the authors (and photographer) take every care to ensure that everything goes perfectly, guiding us through everything from start to finish, including very many high-quality color photos of what things should (and shouldn’t) look like.
On which note, that does mean that to enjoy the color you should get a physical copy or Kindle Fire, not a Kindle e-ink version (as then it’d be black and white).
There’s also a comprehensive section on troubleshooting, as well as hundreds of recipes for all kinds of flavors and occasions.
Bottom line: in the category of books that could reasonably be called “The Bible of…”, this one’s the “The Bible of Kombucha”.
Click here to check out The Big Book Of Kombucha, and get brewing!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why do some autistic people walk differently?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Autism is a neurodevelopmental condition that affects how people’s brains develop and function, impacting behaviour, communication and socialising. It can also involve differences in the way you move and walk – known as your “gait”.
Having an “odd gait” is now listed in the Diagnostic and Statistical Manual of Mental Disorders as a supporting diagnostic feature of autism.
What does this look like?
The most noticeable gait differences among autistic people are:
- toe-walking, walking on the balls of the feet
- in-toeing, walking with one or both feet turned inwards
- out-toeing, walking with one or both feet turned out.
Research has also identified more subtle differences. A study summarising 30 years of research among autistic people reports that gait is characterised by:
- walking more slowly
- taking wider steps
- spending longer in the “stance” phase, when the foot leaves the ground
- taking more time to complete each step.
Autistic people show much more personal variability in the length and speed of their strides, as well as their walking speed.
Gait differences also tend to occur alongside other motor differences, such as issues with balance, coordination, postural stability and handwriting. Autistic people may need support for these other motor skills.
What causes gait differences?
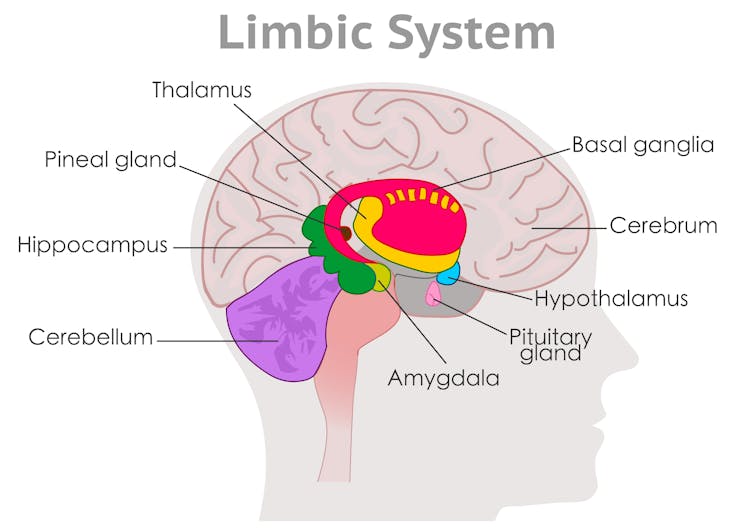
These are largely due to differences in brain development, specifically in areas known as the basal ganglia and cerebellum.
The basal ganglia are broadly responsible for sequencing movement including through shifting posture. It ensures your gait appears effortless, smooth and automatic.
The cerebellum then uses visual and proprioceptive information (to sense the body’s position and movement) to adjust and time movements to maintain postural stability. It ensures movement is controlled and coordinated.

Differences occur in the cerebellum and basal ganglia. grayjay/Shutterstock Developmental differences in these brain regions relate to the way the areas look (their structure), how they work (their function and activation) and how they “speak” to other areas of the brain (their connections).
While some researchers have suggested that autistic gait occurs due to delayed development, we now know gait differences persist across the lifespan. Some differences actually become clearer with age.
In addition to brain-based differences, the autistic gait is also associated with factors such as the person’s broader motor, language and cognitive capabilities.
People with more complex support needs might have more pronounced gait or motor differences, together with language and cognitive difficulties.
Motor dysregulation might indicate sensory or cognitive overload and be a useful marker that the person might benefit from extra support or a break.
How is it managed?
Not all differences need to be treated. Instead, clinicians take an individualised and goals-based approach.
Some autistic people might have subtle gait differences that are observable during testing. But if these differences don’t impact a person’s ability to participate in everyday life, they don’t require support.
An autistic person is likely to benefit from support for gait differences if they have a functional impact on their daily life. This might include:
- increased risk of, or frequent, falls
- difficulty participating in the physical activities they enjoy
- physical consequences such as tightness of the Achilles and calf muscles, or associated pain in other areas, such as the feet or back.
Some children may also benefit from support for motor skill development. However this doesn’t have to occur in a clinic.
Given children spend a large portion of their time at school, programs that integrate opportunities for movement throughout the school day allow autistic children to develop motor skills outside of the clinic and alongside peers. We developed the Joy of Moving Program in Australia, for example, which gets students moving in the classroom.
Our community-based intervention studies show autistic children’s movement abilities can improve after engaging in community-based interventions, such as sports or dance.
Community-based support models empower autistic children to have agency in how they move, rather than seeing different ways of moving as a problem to be fixed.
Where to from here?
While we have learnt a lot about autistic gait at a broad level, researchers and clinicians are still seeking a better understanding of why and when individual variability occurs.
We’re also still determining how to best support individual movement styles, including among children as they develop.
However there is growing evidence that physical activity enhances social skills and behavioural regulation in preschool children with autism.
So it’s encouraging that states and territories are moving towards more community-based foundational supports for autistic children and their peers, as governments develop supports outside the National Disability Insurance Scheme (NDIS).
The authors thank the late Emeritus Professor John Bradshaw for his early input into this piece.
Nicole Rinehart, Nicole Rinehart, Professor, Clinical Psychology, Director of the Neurodevelopment Program, School of Psychological Sciences, Faculty of Medicine, Nursing and Health Sciences, Monash University; Chloe Emonson, Research Fellow, School of Psychological Sciences, Monash University, and Ebony Renee Lindor, Senior Research Fellow and Senior Clinical Neuropsychologist, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Health & Happiness From Outside & In
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A friend in need…
In a recent large (n=3,486) poll across the US:
- 90% of people aged 50 and older say they have at least one close friend
- 75% say they have enough close friends
- 70% of those with a close friend say they can definitely count on them to provide health-related support
However, those numbers shrink by half when it comes to people whose physical and/or mental health is not so great, resulting in a negative feedback loop of fewer close friends whom one sees less often, and progressively worse physical and/or mental health. In other words, the healthier you are, the more likely you are to have a friend who’ll support you in your health:
Read in full: Friendships promote healthier living in older adults, says new survey
Related: How To Beat Loneliness & Isolation
Kindness makes a difference to healthcare outcomes
Defining kindness as action-oriented, positively focused, and purposeful in nature, this sets kindness apart from compassion and empathy, when it’s otherwise often been conflated with those, and thus overlooked. This also means that kindness can still be effected when clinicians are too burned-out to be compassionate, and/or when patients are not in a state of mind where empathy is useful.
Furthermore, unkindness (again, as defined by this review) was found in large studies to be the root cause of ¾ of patient harm events in hospital settings. This means that far from being a wishy-washy abstraction, kindness/unkindness can be a very serious factor when it comes to healthcare outcomes:
Read in full: Review suggests kindness could make for better health care
Related: The Human Touch vs AI, The Doctor That Never Tires
The gift of health?
🎵 Last Christmas, I gave you my heart
Which turned out to be a silly idea
This year, to save me from tears
I’ll just get you a Fitbit or something🎵Health & happiness go hand in hand, so does that make health stuff a good gift? It can do! But there are also plenty of opportunities for misfires.
For example, getting someone a gym membership when they don’t have time for that may not help them at all, and sports equipment that they’ll use once and then leave to gather dust might not be great either. In contrast, the American Heart Association recommends to first consider what they enjoy doing, and work with that, and ideally make it something versatile and/or portable. Wearable gadgets are a fine option for many, but a gift doesn’t have to be fancy to be good—with a blood pressure monitoring cuff being a suggestion from Dr. Sperling (a professor of preventative cardiology):
Read in full: Oh, there’s no gift like health for the holidays
Related: Here’s Where Activity Trackers Help (And Also Where They Don’t)
How you use social media matters more than how much
A study commissioned by the European Commission’s Joint Research Centre found that while the quantity of time one spends on social media is not associated (positively or negatively) with loneliness, they did find a correlation between passive (as opposed to engaged) use of social media, and loneliness. In other words, people who were chatting with friends less, were more lonely! Shocking news.
While the findings may seem obvious, it does present a call-to-action for anyone who is feeling lonely: to use social media not just to see what everyone else is up to, but also, to reach out to people.
Read in full: Unpacking the link between social media and loneliness
Related: Make Social Media Work For Your Mental Health Rather Than Against It
Gut-only antidepressants
Many antidepressants work by increasing serotonin levels in the brain; a new study suggests that targeting antidepressants to work only in the gut (which is where serotonin is made, not the brain) could not only be an effective treatment for mood disorders, but also cause fewer adverse side-effects:
Read in full: Antidepressants may act in gut to reduce depression and anxiety
Related: Antidepressants: Personalization Is Key!
Take care!
Share This Post
-
Is Sugar The New Smoking?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Could you do a this or that of which. Is worse, smoking cigarettes or having a sweet tooth? Also, perhaps have us evaluate one part of newsletter at a time, rather than overall. I especially appreciate your book reviews and often find them through my library system.❞
We’re glad you enjoy the book reviews! We certainly enjoy reading many books to write about them for you.
As for the idea having readers evaluate one part of the newsletter at a time, rather than overall, there is a technical limitation that embedded polls are very large, data-wise, so if we were to do a poll for each section, the email would then get clipped by gmail and other email providers. However, you are always more than welcome to do as you’ve done, and include comments about what section(s) you took the most value from.
Now, onto your main question/request: as it doesn’t quite fit the usual format for our This vs That section, we’ve opted to do it as a main feature here 🙂
So, let’s get into it…
Not a zero-sum game
First, let’s be clear that for most people there is no pressing reason that this should be an either/or decision. There is nothing inherent to quitting either one that makes the other loom larger.
However, that said, if you’re (speaking generally here, and not making any presumptions about the asker) currently smoking regularly and partaking of a lot of added sugar, then you may be wondering which you should prioritize quitting first—as it is indeed generally recommended to only try to quit one thing at a time.
Indeed, we wrote previously, as a guideline for “what to do in one what order”:
Not sure where to start? We suggest this order of priorities, unless you have a major health condition that makes something else a higher priority:
- If you smoke, stop
- If you drink, reduce, or ideally stop
- Improve your diet
About that diet…
Worry less about what to exclude, and instead focus on adding more variety of fruit/veg.
See also: Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
That said, if you’re looking for things to cut, sugar is a top candidate (and red meat is in clear second place albeit some way below)
That’s truncated from a larger list, but those were the top items.
You can read the rest in full, here: The Best Few Interventions For The Best Health: These Top 5 Things Make The Biggest Difference
The flipside of this “you can quit both” reality is that the inverse is also true: much like how having one disease makes it more likely we will get another, unhealthy habits tend to come in clusters too, as each will weaken our resolve with regard to the others. Thus, there is a sort of “comorbidity of habits” that occurs.
The good news is: the same can be said for healthy habits, so they (just like unhealthy habits) can support each other, stack, and compound. This means that while it may seem harder to quit two bad habits than one, in actual fact, the more bad habits you quit, the more it’ll become easy to quit the others. And similarly, the more good habits you adopt, the more it’ll become easy to adopt others.
See also: How To Really Pick Up (And Keep!) Those Habits
So, let’s keep that in mind, while we then look at the cases against smoking, and sugar:
The case against smoking
This is perhaps one of the easiest cases to make in the entirety of the health science world, and the only difficult part is knowing where to start, when there’s so much.
The World Health Organization leads with these key facts, on its tobacco fact sheet:
- Tobacco kills up to half of its users who don’t quit.
- Tobacco kills more than 8 million people each year, including an estimated 1.3 million non-smokers who are exposed to second-hand smoke.
- Around 80% of the world’s 1.3 billion tobacco users live in low- and middle-income countries.
- In 2020, 22.3% of the world’s population used tobacco: 36.7% of men and 7.8% of women.
- To address the tobacco epidemic, WHO Member States adopted the WHO Framework Convention on Tobacco Control (WHO FCTC) in 2003. Currently 182 countries are Parties to this treaty.
- The WHO MPOWER measures are in line with the WHO FCTC and have been shown to save lives and reduce costs from averted healthcare expenditure.
Source: World Health Organization | Tobacco
Now, some of those are just interesting sociological considerations (well, they are of practical use to the WHO whose job it is to offer global health policy guidelines, but for us at 10almonds, with the more modest goal of helping individual people lead their best healthy lives, there’s not so much that we can do with the Framework Convention on Tobacco Control, for example), but for the individual smoker, the first two are really very serious, so let’s take a closer look:
❝Tobacco kills up to half of its users who don’t quit.❞
A bold claim, backed up by at least three very large, very compelling studies:
- Mortality in relation to smoking: 50 years’ observations on male British doctors
- Tobacco smoking and all-cause mortality in a large Australian cohort study: findings from a mature epidemic with current low smoking prevalence
- Global burden of disease due to smokeless tobacco consumption in adults: an updated analysis of data from 127 countries
❝Tobacco kills more than 8 million people each year, including an estimated 1.3 million non-smokers who are exposed to second-hand smoke.❞
The WHO’s cited source for this was gatekept in a way we couldn’t access (and so probably most of our readers can’t either), but take a look at what the CDC has to say for the US alone (bearing in mind the US’s population of a little over 300,000,000, which is just 3.75% of the global population of a little over 8,000,000,000):
❝smoking causes more than 480,000 deaths [in the US] annually, with an estimated 41,000 deaths from secondhand smoke exposure, and it can reduce a person’s life expectancy by 10 years. Quitting smoking before the age of 40 reduces the risk of dying from smoking-related disease by about 90%❞
If we now remember that third bullet point, that said “Around 80% of the world’s 1.3 billion tobacco users live in low- and middle-income countries.”, then we can imagine the numbers are worse for many other countries, including large-population countries that have a lower median income than the US, such as India and Brazil.
Source for the CDC comment: Tobacco-Related Mortality
See also: AAMC | Smoking is still the leading cause of preventable death in the U.S.
We only have so much room here, but if that’s not enough…
More than 100 reasons to quit tobacco
The case against sugar
We reviewed an interesting book about this:
The Case Against Sugar – by Gary Taubes
But suffice it to say, added sugar is a big health problem; not in the same league as tobacco, but it’s big, because of how it messes with our metabolism (and when our metabolism goes wrong, everything else goes wrong):
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
The epidemiology of sugar consumption and related mortality is harder to give clear stats about than smoking, because there’s not a clear yes/no indicator, and cause and effect are harder to establish when the waters are so muddied by other factors. But for comparison, we’ll note that compared to the 480,000 deaths caused by tobacco in the US annually, the total death to diabetes (which is not necessarily “caused by sugar consumption”, but there’s at least an obvious link when it comes to type 2 diabetes and refined carbohydrates) was 101,209 deaths due to diabetes in 2022:
National Center for Health Statistics | Diabetes
Now, superficially, that looks like “ok, so smoking is just under 5x more deadly”, but it’s important to remember that almost everyone eats added sugar, whereas a minority of people smoke, and those are mortality per total US population figures, not mortality per user of the substance in question. So in fact, smoking is, proportionally to how many people smoke, many times more deadly than diabetes, which currently ranks 8th in the “top causes of death” list.
Note: we recognize that you did say “having a sweet tooth” rather than “consuming added sugar”, but it’s worth noting that artificial sweeteners are not a get-out-of-illness-free card either:
Let’s get back to sugar though, as while it’s a very different beast than tobacco, it is arguably addictive also, by multiple mechanisms of addiction:
The Not-So-Sweet Science Of Sugar Addiction
That said, those mechanisms of addiction are not necessarily as strong as some others, so in the category of what’s easy or hard to quit, this is on the easier end of things—not that that means it’s easy, just, quitting many drugs is harder. In any case, it can be done:
When It’s More Than “Just” Cravings: Beat Food Addictions!
In summary
Neither are good for the health, but tobacco is orders of magnitude worse, and should be the priority to quit, unless your doctor(s) tell you otherwise because of your personal situation, and even then, try to get multiple opinions to be sure.
Take care!
Share This Post


Related Posts
-

Wholesome Threesome Protein Soup
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This soup has two protein– and fiber-rich pseudo-grains, one real wholegrain, and nutrient-dense cashews for yet even more protein, and all of the above are full of many great vitamins and minerals. All in all, a well-balanced and highly-nutritious light meal!
You will need
- ⅓ cup quinoa
- ⅓ cup green lentils
- ⅓ cup wholegrain rice
- 5 cups low-sodium vegetable stock (ideally you made this yourself from offcuts of vegetables, but failing that, low-sodium stock cubes can be bought in most large supermarkets)
- ¼ cup cashews
- 1 tbsp dried thyme
- 1 tbsp black pepper, coarse ground
- ½ tsp MSG or 1 tsp low-sodium salt
Optional topping:
- ⅓ cup pine nuts
- ⅓ cup finely chopped fresh mint leaves
- 2 tbsp coconut oil
Method
(we suggest you read everything at least once before doing anything)
1) Rinse the quinoa, lentils, and rice.
2) Boil 4 cups of the stock and add the grains and seasonings (MSG/salt, pepper, thyme); simmer for about 25 minutes.
3) Blend the cashews with the other cup of vegetable stock, until smooth. Add the cashew mixture to the soup, stirring it in, and allow to simmer for another 5 minutes.
4) Heat the coconut oil in a skillet and add the pine nuts, stirring until they are golden brown.
5) Serve the soup into bowls, adding the mint and pine nuts to each.
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Give Us This Day Our Daily Dozen
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- Why You Should Diversify Your Nuts!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Women take more antidepressants after divorce than men but that doesn’t mean they’re more depressed
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Research out today from Finland suggests women may find it harder to adjust to later-life divorce and break-ups than men.
The study used population data from 229,000 Finns aged 50 to 70 who had undergone divorce, relationship break-up or bereavement and tracked their use of antidepressants before and after their relationship ended.
They found antidepressant use increased in the four years leading to the relationship dissolution in both genders, with women experiencing a more significant increase.
But it’s too simplistic to say women experience poorer mental health or tend to be less happy after divorce than men.
Remind me, how common is divorce?
Just under 50,000 divorces are granted each year in Australia. This has slowly declined since the 1990s.
More couple are choosing to co-habitate, instead of marry, and the majority of couples live together prior to marriage. Divorce statistics don’t include separations of cohabiting couples, even though they are more likely than married couples to separate.
Those who divorce are doing so later in life, often after their children grow up. The median age of divorce increased from 45.9 in 2021 to 46.7 in 2022 for men and from 43.0 to 43.7 for women.
The trend of late divorces also reflects people deciding to marry later in life. The median duration from marriage to divorce in 2022 was around 12.8 years and has remained fairly constant over the past decade.
Why do couples get divorced?
Changes in social attitudes towards marriage and relationships mean divorce is now more accepted. People are opting not to be in unhappy marriages, even if there are children involved.
Instead, they’re turning the focus on marriage quality. This is particularly true for women who have established a career and are financially autonomous.
Similarly, my research shows it’s particularly important for people to feel their relationship expectations can be fulfilled long term. In addition to relationship quality, participants reported needing trust, open communication, safety and acceptance from their partners.
“Grey divorce” (divorce at age 50 and older) is becoming increasingly common in Western countries, particularly among high-income populations. While factors such as an empty nest, retirement, or poor health are commonly cited predictors of later-in-life divorce, research shows older couples divorce for the same reasons as younger couples.
What did the new study find?
The study tracked antidepressant use in Finns aged 50 to 70 for four years before their relationship breakdown and four years after.
They found antidepressant use increased in the four years leading to the relationship break-up in both genders. The proportion of women taking antidepressants in the lead up to divorce increased by 7%, compared with 5% for men. For de facto separation antidepressant use increased by 6% for women and 3.2% for men.
Within a year of the break-up, antidepressant use fell back to the level it was 12 months before the break-up. It subsequently remained at that level among the men.
But it was a different story for women. Their use tailed off only slightly immediately after the relationship breakdown but increased again from the first year onwards.
Women’s antidepressant use increased again.
sk/UnsplashThe researchers also looked at antidepressant use after re-partnering. There was a decline in the use of antidepressants for men and women after starting a new relationship. But this decline was short-lived for women.
But there’s more to the story
Although this data alone suggest women may find it harder to adjust to later-life divorce and break-ups than men, it’s important to note some nuances in the interpretation of this data.
For instance, data suggesting women experience depression more often than men is generally based on the rate of diagnoses and antidepressant use, which does not account for undiagnosed and unmedicated people.
Women are generally more likely to access medical services and thus receive treatment. This is also the case in Australia, where in 2020–2022, 21.6% of women saw a health professional for their mental health, compared with only 12.9% of men.
Why women might struggle more after separating
Nevertheless, relationship dissolution can have a significant impact on people’s mental health. This is particularly the case for women with young children and older women.
So what factors might explain why women might experience greater difficulties after divorce later in life?
Research investigating the financial consequences of grey divorce in men and women showed women experienced a 45% decline in their standard of living (measured by an income-to-needs ratio), whereas men’s dropped by just 21%. These declines persisted over time for men, and only reversed for women following re-partnering.
Another qualitative study investigating the lived experiences of heterosexual couples post-grey divorce identified financial worries as a common theme between female participants.
A female research participant (age 68) said:
[I am most worried about] the money, [and] what I’m going to do when the little bit of money I have runs out […] I have just enough money to live. And, that’s it, [and if] anything happens I’m up a creek. And Medicare is incredibly expensive […] My biggest expense is medicine.
Another factor was loneliness. One male research participant (age 54) described he preferred living with his ex-wife, despite not getting along with her, than being by himself:
It was still [good] knowing that [the] person was there, and now that’s gone.
Other major complications of later-life divorce are possible issues with inheritance rights and next-of-kin relationships for medical decision-making.
Separation can be positive
For some people, divorce or separation can lead to increased happiness and feeling more independent.
And the mental health impact and emotional distress of a relationship dissolution is something that can be counterattacked with resilience. Resilience to dramatic events built from life experience means older adults often do respond better to emotional distress and might be able to adjust better to divorce than their younger counterparts.

Raquel Peel, Adjunct Senior Lecturer, University of Southern Queensland and Senior Lecturer, RMIT University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
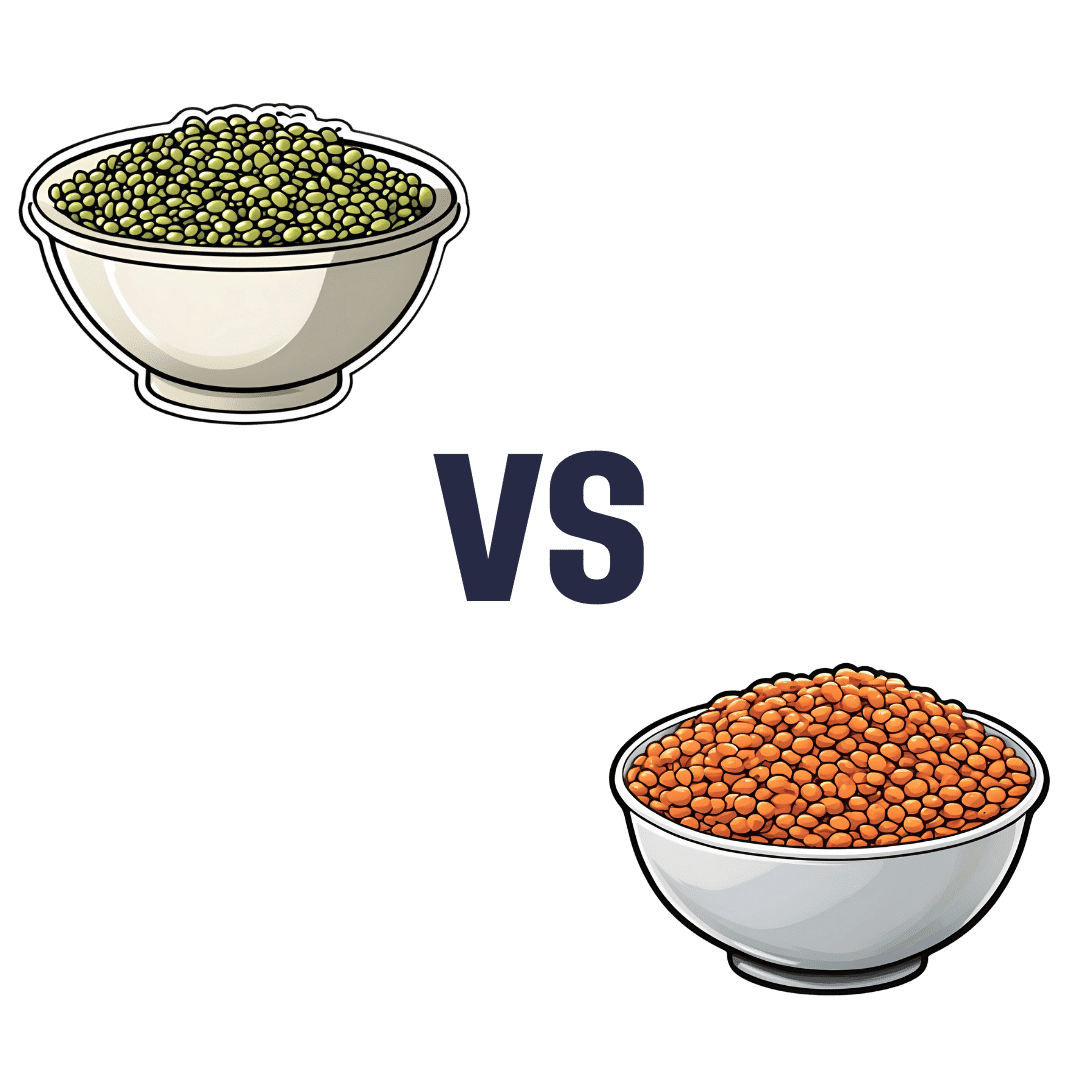
Mung Beans vs Red Lentils – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing mung beans to red lentils, we picked the lentils.
Why?
Both are great! But the lentils win on overall nutritional density.
In terms of macros, they have approximately the same carbs and fiber, and are both low glycemic index foods. The deciding factor is that the lentils have slightly more protein—but it’s not a huge difference; both are very good sources of protein.
In the category of vitamins, mung beans have more of vitamins A, E, and K, while red lentils have more of vitamins B1, B2, B3, B5, B6, B9, C, and choline. An easy win for lentils.
When it comes to minerals, again both are great, but mung beans have more calcium and magnesium (hence the green color) while red lentils have more copper, iron, manganese, phosphorus, potassium, selenium, and zinc. Another clear win for lentils.
Polyphenols are also a worthy category to note here; both have plenty, but red lentils have more, especially flavonols, anthocyanidins, proanthocyanidins, and anthocyanins (whence the red color).
In short: enjoy both, because diversity is almost always best. But if you’re picking one, red lentils are the most nutritious of the two.
Want to learn more?
You might like to read:
Sprout Your Seeds, Grains, Beans, Etc
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: