Why do some autistic people walk differently?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Autism is a neurodevelopmental condition that affects how people’s brains develop and function, impacting behaviour, communication and socialising. It can also involve differences in the way you move and walk – known as your “gait”.
Having an “odd gait” is now listed in the Diagnostic and Statistical Manual of Mental Disorders as a supporting diagnostic feature of autism.
What does this look like?
The most noticeable gait differences among autistic people are:
- toe-walking, walking on the balls of the feet
- in-toeing, walking with one or both feet turned inwards
- out-toeing, walking with one or both feet turned out.
Research has also identified more subtle differences. A study summarising 30 years of research among autistic people reports that gait is characterised by:
- walking more slowly
- taking wider steps
- spending longer in the “stance” phase, when the foot leaves the ground
- taking more time to complete each step.
Autistic people show much more personal variability in the length and speed of their strides, as well as their walking speed.
Gait differences also tend to occur alongside other motor differences, such as issues with balance, coordination, postural stability and handwriting. Autistic people may need support for these other motor skills.
What causes gait differences?
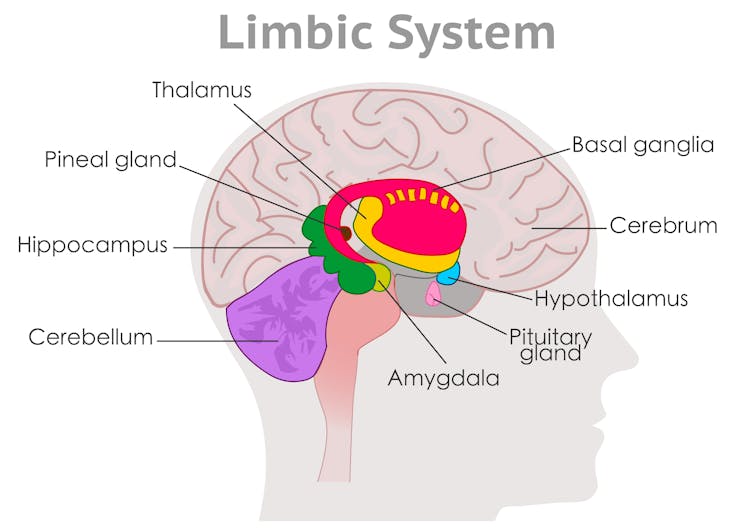
These are largely due to differences in brain development, specifically in areas known as the basal ganglia and cerebellum.
The basal ganglia are broadly responsible for sequencing movement including through shifting posture. It ensures your gait appears effortless, smooth and automatic.
The cerebellum then uses visual and proprioceptive information (to sense the body’s position and movement) to adjust and time movements to maintain postural stability. It ensures movement is controlled and coordinated.
Developmental differences in these brain regions relate to the way the areas look (their structure), how they work (their function and activation) and how they “speak” to other areas of the brain (their connections).
While some researchers have suggested that autistic gait occurs due to delayed development, we now know gait differences persist across the lifespan. Some differences actually become clearer with age.
In addition to brain-based differences, the autistic gait is also associated with factors such as the person’s broader motor, language and cognitive capabilities.
People with more complex support needs might have more pronounced gait or motor differences, together with language and cognitive difficulties.
Motor dysregulation might indicate sensory or cognitive overload and be a useful marker that the person might benefit from extra support or a break.
How is it managed?
Not all differences need to be treated. Instead, clinicians take an individualised and goals-based approach.
Some autistic people might have subtle gait differences that are observable during testing. But if these differences don’t impact a person’s ability to participate in everyday life, they don’t require support.
An autistic person is likely to benefit from support for gait differences if they have a functional impact on their daily life. This might include:
- increased risk of, or frequent, falls
- difficulty participating in the physical activities they enjoy
- physical consequences such as tightness of the Achilles and calf muscles, or associated pain in other areas, such as the feet or back.
Some children may also benefit from support for motor skill development. However this doesn’t have to occur in a clinic.
Given children spend a large portion of their time at school, programs that integrate opportunities for movement throughout the school day allow autistic children to develop motor skills outside of the clinic and alongside peers. We developed the Joy of Moving Program in Australia, for example, which gets students moving in the classroom.
Our community-based intervention studies show autistic children’s movement abilities can improve after engaging in community-based interventions, such as sports or dance.
Community-based support models empower autistic children to have agency in how they move, rather than seeing different ways of moving as a problem to be fixed.
Where to from here?
While we have learnt a lot about autistic gait at a broad level, researchers and clinicians are still seeking a better understanding of why and when individual variability occurs.
We’re also still determining how to best support individual movement styles, including among children as they develop.
However there is growing evidence that physical activity enhances social skills and behavioural regulation in preschool children with autism.
So it’s encouraging that states and territories are moving towards more community-based foundational supports for autistic children and their peers, as governments develop supports outside the National Disability Insurance Scheme (NDIS).
The authors thank the late Emeritus Professor John Bradshaw for his early input into this piece.
Nicole Rinehart, Nicole Rinehart, Professor, Clinical Psychology, Director of the Neurodevelopment Program, School of Psychological Sciences, Faculty of Medicine, Nursing and Health Sciences, Monash University; Chloe Emonson, Research Fellow, School of Psychological Sciences, Monash University, and Ebony Renee Lindor, Senior Research Fellow and Senior Clinical Neuropsychologist, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Can You Pass This 10-Second Walking Test?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This 10-second walking test should actually only take about 4 seconds, but it’s very important:
Stepping into good health
Set up a 12ft walkway (it doesn’t have to be anything special, just a flat floor on which you can walk in a straight line for about 12ft). Walk at a normal pace while timing yourself, and if it takes longer than about 4 seconds to walk that distance, then your walking speed is in a risk zone for future loss of independence.
Why walking speed matters: slower walking, especially after age 60, strongly predicts falls, fatigue, and declining independence, often before people realize there’s a problem.
So, what causes slow walking speed? Weak calves, stiff hips, and weak glutes are the three most common and most fixable reasons walking speed drops with age. Of those,
- Weak glutes: the gluteus maximus provides push-off power and upright stability, and when it isn’t firing, walking feels flat, slow, and draining.
- Weak calves: calves act as your walking engine, and when they weaken, pushing forwards feels harder, balance worsens, and walking becomes slower and more tiring.
- Stiff hips: tight hip flexors shorten your stride, making walking slower and more effortful, with prolonged sitting being the biggest contributor.
So, what to do about it?
- Prone glute training: lie on your front, gently squeeze your glutes, lift one leg slightly while keeping your lower back relaxed, then lower with control to target your glutes rather than your spine.
- Single-leg donkey calf raise: lean forwards with your hands on a chair or counter, lift one foot, and repeatedly push up onto your tiptoes and lower with control, using both legs if balance feels unsafe.
- Skateboard swings: no skateboard necessary; just stand holding a support, keep your back upright, place your weight on one leg, and swing the free leg forwards and backwards in a controlled motion to restore hip extension.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
90% Of People Over 50 Fail This Balance Test. Will You?
Take care!
Share This Post
-
Rapid Rise in Syphilis Hits Native Americans Hardest
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
From her base in Gallup, New Mexico, Melissa Wyaco supervises about two dozen public health nurses who crisscross the sprawling Navajo Nation searching for patients who have tested positive for or been exposed to a disease once nearly eradicated in the U.S.: syphilis.
Infection rates in this region of the Southwest — the 27,000-square-mile reservation encompasses parts of Arizona, New Mexico, and Utah — are among the nation’s highest. And they’re far worse than anything Wyaco, who is from Zuni Pueblo (about 40 miles south of Gallup) and is the nurse consultant for the Navajo Area Indian Health Service, has seen in her 30-year nursing career.
Syphilis infections nationwide have climbed rapidly in recent years, reaching a 70-year high in 2022, according to the most recent data from the Centers for Disease Control and Prevention. That rise comes amid a shortage of penicillin, the most effective treatment. Simultaneously, congenital syphilis — syphilis passed from a pregnant person to a baby — has similarly spun out of control. Untreated, congenital syphilis can cause bone deformities, severe anemia, jaundice, meningitis, and even death. In 2022, the CDC recorded 231 stillbirths and 51 infant deaths caused by syphilis, out of 3,761 congenital syphilis cases reported that year.
And while infections have risen across the U.S., no demographic has been hit harder than Native Americans. The CDC data released in January shows that the rate of congenital syphilis among American Indians and Alaska Natives was triple the rate for African Americans and nearly 12 times the rate for white babies in 2022.
“This is a disease we thought we were going to eradicate not that long ago, because we have a treatment that works really well,” said Meghan Curry O’Connell, a member of the Cherokee Nation and chief public health officer at the Great Plains Tribal Leaders’ Health Board, who is based in South Dakota.
Instead, the rate of congenital syphilis infections among Native Americans (644.7 cases per 100,000 people in 2022) is now comparable to the rate for the entire U.S. population in 1941 (651.1) — before doctors began using penicillin to cure syphilis. (The rate fell to 6.6 nationally in 1983.)
O’Connell said that’s why the Great Plains Tribal Leaders’ Health Board and tribal leaders from North Dakota, South Dakota, Nebraska, and Iowa have asked federal Health and Human Services Secretary Xavier Becerra to declare a public health emergency in their states. A declaration would expand staffing, funding, and access to contact tracing data across their region.
“Syphilis is deadly to babies. It’s highly infectious, and it causes very severe outcomes,” O’Connell said. “We need to have people doing boots-on-the-ground work” right now.
In 2022, New Mexico reported the highest rate of congenital syphilis among states. Primary and secondary syphilis infections, which are not passed to infants, were highest in South Dakota, which had the second-highest rate of congenital syphilis in 2022. In 2021, the most recent year for which demographic data is available, South Dakota had the second-worst rate nationwide (after the District of Columbia) — and numbers were highest among the state’s large Native population.
In an October news release, the New Mexico Department of Health noted that the state had “reported a 660% increase in cases of congenital syphilis over the past five years.” A year earlier, in 2017, New Mexico reported only one case — but by 2020, that number had risen to 43, then to 76 in 2022.
Starting in 2020, the covid-19 pandemic made things worse. “Public health across the country got almost 95% diverted to doing covid care,” said Jonathan Iralu, the Indian Health Service chief clinical consultant for infectious diseases, who is based at the Gallup Indian Medical Center. “This was a really hard-hit area.”
At one point early in the pandemic, the Navajo Nation reported the highest covid rate in the U.S. Iralu suspects patients with syphilis symptoms may have avoided seeing a doctor for fear of catching covid. That said, he doesn’t think it’s fair to blame the pandemic for the high rates of syphilis, or the high rates of women passing infections to their babies during pregnancy, that continue four years later.
Native Americans are more likely to live in rural areas, far from hospital obstetric units, than any other racial or ethnic group. As a result, many do not receive prenatal care until later in pregnancy, if at all. That often means providers cannot test and treat patients for syphilis before delivery.
In New Mexico, 23% of patients did not receive prenatal care until the fifth month of pregnancy or later, or received fewer than half the appropriate number of visits for the infant’s gestational age in 2023 (the national average is less than 16%).
Inadequate prenatal care is especially risky for Native Americans, who have a greater chance than other ethnic groups of passing on a syphilis infection if they become pregnant. That’s because, among Native communities, syphilis infections are just as common in women as in men. In every other ethnic group, men are at least twice as likely to contract syphilis, largely because men who have sex with men are more susceptible to infection. O’Connell said it’s not clear why women in Native communities are disproportionately affected by syphilis.
“The Navajo Nation is a maternal health desert,” said Amanda Singer, a Diné (Navajo) doula and lactation counselor in Arizona who is also executive director of the Navajo Breastfeeding Coalition/Diné Doula Collective. On some parts of the reservation, patients have to drive more than 100 miles to reach obstetric services. “There’s a really high number of pregnant women who don’t get prenatal care throughout the whole pregnancy.”
She said that’s due not only to a lack of services but also to a mistrust of health care providers who don’t understand Native culture. Some also worry that providers might report patients who use illicit substances during their pregnancies to the police or child welfare. But it’s also because of a shrinking network of facilities: Two of the Navajo area’s labor and delivery wards have closed in the past decade. According to a recent report, more than half of U.S. rural hospitals no longer offer labor and delivery services.
Singer and the other doulas in her network believe New Mexico and Arizona could combat the syphilis epidemic by expanding access to prenatal care in rural Indigenous communities. Singer imagines a system in which midwives, doulas, and lactation counselors are able to travel to families and offer prenatal care “in their own home.”
O’Connell added that data-sharing arrangements between tribes and state, federal, and IHS offices vary widely across the country, but have posed an additional challenge to tackling the epidemic in some Native communities, including her own. Her Tribal Epidemiology Center is fighting to access South Dakota’s state data.
In the Navajo Nation and surrounding area, Iralu said, IHS infectious disease doctors meet with tribal officials every month, and he recommends that all IHS service areas have regular meetings of state, tribal, and IHS providers and public health nurses to ensure every pregnant person in those areas has been tested and treated.
IHS now recommends all patients be tested for syphilis yearly, and tests pregnant patients three times. It also expanded rapid and express testing and started offering DoxyPEP, an antibiotic that transgender women and men who have sex with men can take up to 72 hours after sex and that has been shown to reduce syphilis transmission by 87%. But perhaps the most significant change IHS has made is offering testing and treatment in the field.
Today, the public health nurses Wyaco supervises can test and treat patients for syphilis at home — something she couldn’t do when she was one of them just three years ago.
“Why not bring the penicillin to the patient instead of trying to drag the patient in to the penicillin?” said Iralu.
It’s not a tactic IHS uses for every patient, but it’s been effective in treating those who might pass an infection on to a partner or baby.
Iralu expects to see an expansion in street medicine in urban areas and van outreach in rural areas, in coming years, bringing more testing to communities — as well as an effort to put tests in patients’ hands through vending machines and the mail.
“This is a radical departure from our past,” he said. “But I think that’s the wave of the future.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

Monosodium Glutamate: Sinless Flavor-Enhancer Or Terrible Health Risk?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s The Deal With MSG?
There are a lot of popular beliefs about MSG. Is there a grain of truth, or should we take them with a grain of salt? We’ll leap straight into myth-busting:
MSG is high in salt
True (technically) False (practically)
- MSG is a salt (a monosodium salt of L-glutamic acid), but to call it “full of salt” in practical terms is like calling coffee “full of fruit”. (Coffee beans are botanically fruit)
- It does contain sodium, though which is what the S stands for!
- We talked previously about how MSG’s sodium content is much lower than that of (table) salt. Specifically, it’s about one third of that of sodium chloride (e.g. table salt).
MSG triggers gluten sensitivity
False!
Or at least, because this kind of absolute negative is hard to prove in science, what we can say categorically is: it does not contain gluten. We understand that the similar name can cause that confusion. However:
- Gluten is a protein, found in wheat (and thus wheat-based foods).
- Glutamate is an amino acid, found in protein-rich foods.
- If you’re thinking “but proteins are made from amino acids”, yes, they are, but the foundational amino acid of gluten is glutamine, not glutamate. Different bricks → different house!
The body can’t process MSG correctly
False!
The body has glutamate receptors throughout the gut and nervous system.
The body metabolizes glutamate from MSG just the same as from any other food that contains it naturally.
Read: Update on food safety of monosodium l-glutamate (MSG) ← evidence-based safety review
MSG causes “Chinese Restaurant Syndrome”
False!
Racism causes that. It finds its origins in what was originally intended as a satirical joke, that the papers picked up and ran with, giving it that name in the 1960s. As to why it grew and persisted, that has more to do with US politics (the US has been often at odds with China for a long time) and xenophobia (people distrust immigrants, such as those who opened restaurants), including nationalistic rhetoric associating immigrants with diseases.
Read: Xenophobia in America in the Age of Coronavirus and Beyond ← academic paper that gives quite a compact yet comprehensive overview
Research science, meanwhile, has not found any such correlation, in more than 40 years of looking.
PS: we realize this item in the list is very US-centric. Apologies to our non-US subscribers. We know that this belief isn’t so much of a thing outside the US—though it certainly can crop up elsewhere sometimes, too.
Are there any health risks associated with MSG, then?
Well, as noted, it does contain sodium, albeit much less than table salt. So… do go easy on it, all the same.
Aside from that, the LD50 (a way of measuring toxicity) of MSG is 15.8g/kg, so if for example you weigh 150lb (68 kg), don’t eat 2.2lb (a kilogram) of MSG.
There have been some studies on rats (or in one case, fruit flies) that found high doses of MSG could cause heart problems and/or promote obesity. However:
- this has not been observed to be the case in humans
- those doses were really high, ranging from 1g/kg to 8g/kg. So that’d be the equivalent of our 150lb person eating it by the cupful
- it was injected (as a solution) into the rats, not ingested by them
- so don’t let someone inject you with a cup of MSG!
Read: A review of the alleged health hazards of monosodium glutamate
Bottom line on MSG and health:
Enjoy in moderation, but enjoy if you wish! MSG is just the salt form of the amino acid glutamate, which is found naturally in many foods, including shrimp, seaweed, and tomatoes.
Scientists have spent more than 40 years trying to find health risks for MSG, and will probably keep trying (which is as science should be), but for now… Everything has either come up negative, or has been the result of injecting laboratory animals with megadoses.
If you’d like to try it in your cooking as a low-sodium way to bring out the flavor of your dishes, you can order it online. Cheapest in bulk, but try it and see if you like it first!
(I’ll be real with you… I have 5 kg in the pantry myself and use about half a teaspoon a day, cooking for two)
Share This Post


-

Cranberry juice really can help with UTIs – and reduce reliance on antibiotics
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cranberry juice has been used medicinally for centuries. Our new research indicates it should be a normal aspect of urinary tract infection (UTI) management today.
While some benefits of cranberry compounds for the prevention of UTIs have been suspected for some time, it hasn’t been clear whether the benefits from cranberry juice were simply from drinking more fluid, or something in the fruit itself.
For our study, published this week, we combined and collectively assessed 3,091 participants across more than 20 clinical trials.
Our analysis indicates that increasing liquids reduces the rate of UTIs compared with no treatment, but cranberry in liquid form is even better at reducing UTIs and antibiotic use.

Julie Falk/Flickr, CC BY-NC-ND Are UTIs really that bad?
Urinary tract infections affect more than 50% of women and 20% of men in their lifetime.
Most commonly, UTIs are caused from the bug called Escherichia coli (E.coli). This bug lives harmlessly in our intestines, but can cause infection in the urinary tract. This is why, particularly for women, it is recommended people wipe from front to back after using the toilet.
An untreated UTI can move up to the kidneys and cause even more serious illness.
Even when not managing infection, many people are anxious about contracting a UTI. Sexually active women, pregnant women and older women may all be at increased risk.
Why cranberries?
To cause a UTI, the bacteria need to attach to the wall of the urinary bladder. Increasing fluids helps to flush out bacteria before it attaches (or makes its way up into the bladder).
Some beneficial compounds in cranberry, such as proanthocyanidins (also called condensed tannins), prevent the bacteria from attaching to the wall itself.
While there are treatments, over 90% of the bugs that cause UTIs exhibit some form of microbial resistance. This suggests that they are rapidly changing and some cases of UTI might be left untreatable.
The juice of cranberries has long been thought to have infection-fighting properties. duckeesue/Shutterstock What we found
Our analysis showed a 54% lower rate of UTIs from cranberry juice consumption compared to no treatment. This means that significantly fewer participants who regularly consumed cranberry juice (most commonly around 200 millilitres each day) reported having a UTI during the periods assessed in the studies we analysed.
Cranberry juice was also linked to a 49% lower rate of antibiotic use than placebo liquid and a 59% lower rate than no treatment, based on analysis of indirect and direct effects across six studies. The use of cranberry compounds, whether in drinks or tablet form, also reduced the prevalence of symptoms associated with UTIs.
While some studies we included presented conflicts of interest (such as receiving funding from cranberry companies), we took this “high risk of bias” into account when analysing the data.
The study found extra hydration helped but not to the same extent as cranberry juice. Pixelshot/Shutterstock So, when can cranberry juice help?
We found three main benefits of cranberry juice for UTIs.
1. Reduced rates of infections
Increasing fluids (for example, drinking more water) reduced the prevalence of UTIs, and taking cranberry compounds (such as tablets) was also beneficial. But the most benefits were identified from increasing fluids and taking cranberry compounds at the same time, such as with cranberry juice.
2. Reduced use of antibiotics
The data shows cranberry juice lowers the need to use antibiotics by 59%. This was identified as fewer participants in randomised cranberry juice groups required antibiotics.
Increasing fluid intake also helped reduce antibiotic use (by 25%). But this was not as useful as increasing fluids at the same time as using cranberry compounds.
Cranberry compounds alone (such as tablets without associated increases in fluid intake) did not affect antibiotic use.
3. Reducing symptoms
Taking cranberry compounds (in any form, liquid or tablet) reduced the symptoms of UTIs, as measured in the overall data, by more than five times.
Take home advice
While cranberry juice cannot treat a UTI, it can certainly be part of UTI management.
If you suspect that you have a UTI, see your GP as soon as possible.
Christian Moro, Associate Professor of Science & Medicine, Bond University and Charlotte Phelps, Senior Teaching Fellow, Medical Program, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Samosa Spiced Surprise
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You know what’s best about samosas? It’s not actually the fried pastry; that’s just what holds it together. If you were to try eating sheets of pastry alone, it would not be much fun. But, the spiced vegetable filling? Now we’re talking! So, this recipe takes what’s best about samosas, and makes them into healthy snack-sized patties.
You will need
- Extra virgin olive oil, or coconut oil (per your preference) for cooking
- 4 medium potatoes, boiled, peeled, and mashed
- 1 medium onion, diced
- 1 cup peas
- 1 carrot, finely chopped
- ½ cup garbanzo bean flour (chickpea flour, gram flour, whatever your supermarket calls it)
- ¼ cup fresh cilantro, chopped (substitute parsley if you have the soap gene)
- ¼ bulb garlic, minced
- 1 jalapeño pepper, chopped
- 1 tbsp ground cumin
- 2 tsp garam masala
- 1 tsp ground coriander
- 1 tsp ground turmeric
- 1 tsp ground black pepper
Method
(we suggest you read everything at least once before doing anything)
1) Fry the onion until it is becoming soft and translucent (3–5 minutes).
2) Add the spices (the garlic, both kinds of pepper, cumin, coriander, turmeric, and the garam masala), stirring in well
3) Add the carrot and peas, stirring and cooking until just becoming soft (probably another 3–5 minutes, depending on the heat, how small you chopped the carrot, and whether the peas were frozen or fresh). Take it off the heat.
4) Mix the potato, chickpea flour, and cilantro in a bowl, and carefully add everything from the pan, mixing that in thoroughly too.
5) Shape into patties, and fry them on each side until browned and crispy.
6) Serve as part of a buffet, or perhaps as an appetizer—raita is a fine accompaniment option.
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cognitive Enhancement Without Drugs
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cognitive Enhancement Without Drugs

This is Elizabeth Ricker. She’s a Harvard-and-MIT-trained neuroscientist and researcher, who now runs the “Citizen Science” DIY-neurohacking organization, NeuroEducate.
Sounds fun! What’s it about?
The philosophy that spurs on her research and practice can be summed up as follows:
❝I’m not going to leave my brain up to my doctor or [anyone else]… My brain is my own responsibility, and I’m going to do the best that I can to optimize it❞
Her goal is not just to optimize her own brain though; she wants to make the science accessible to everyone.
What’s this about Citizen Science?
“Citizen Science” is the idea that while there’s definitely an important role in society for career academics, science itself should be accessible to all. And, not just the conclusions, but the process too.
This can take the form of huge experiments, often facilitated these days by apps where we opt-in to allow our health metrics (for example) to be collated with many thousands of others, for science. It can also involve such things as we talked about recently, getting our own raw genetic data and “running the numbers” at home to get far more comprehensive and direct information than the genetic testing company would ever provide us.
For Ricker, her focus is on the neuroscience side of biohacking, thus, neurohacking.
I’m ready to hack my brain! Do I need a drill?
Happily not! Although… Bone drills for the skull are very convenient instruments that make it quite hard to go wrong even with minimal training. The drill bit has a little step/ledge partway down, which means you can only drill through the thickness of the skull itself, before the bone meeting the wider part of the bit stops you from accidentally drilling into the brain. Still, please don’t do this at home.
What you can do at home is a different kind of self-experimentation…
If you want to consider which things are genuinely resulting in cognitive enhancement and which things are not, you need to approach the matter like a scientist. That means going about it in an organized fashion, and recording results.
There are several ways cognitive enhancement can be measured, including:
- Learning and memory
- Executive function
- Emotional regulation
- Creative intelligence
Let’s look at each of them, and what can be done. We don’t have a lot of room here; we’re a newsletter not a book, but we’ll cover one of Ricker’s approaches for each:
Learning and memory
This one’s easy. We’re going to leverage neuroplasticity (neurons that fire together, wire together!) by simple practice, and introduce an extra element to go alongside your recall. Perhaps a scent, or a certain item of clothing. Tell yourself that clinical studies have shown that this will boost your recall. It’s true, but that’s not what’s important; what’s important is that you believe it, and bring the placebo effect to bear on your endeavors.
You can test your memory with word lists, generated randomly by AI, such as this one:
You’ll soon find your memory improving—but don’t take our word for it!
Executive function
Executive function is the aspect of your brain that tells the other parts how to work, when to work, and when to stop working. If you’ve ever spent 30 minutes thinking “I need to get up” but you were stuck in scrolling social media, that was executive dysfunction.
This can be trained using the Stroop Color and Word Test, which shows you words, specifically the names of colors, which will themselves be colored, but not necessarily in the color the word pertains to. So for example, you might be shown the word “red”, colored green. Your task is to declare either the color of the word only, ignoring the word itself, or the meaning of the word only, ignoring its appearance. It can be quite challenging, but you’ll get better quite quickly:
The Stroop Test: Online Version
Emotional Regulation
This is the ability to not blow up angrily at the person with whom you need to be diplomatic, or to refrain from laughing when you thought of something funny in a sombre situation.
It’s an important part of cognitive function, and success or failure can have quite far-reaching consequences in life. And, it can be trained too.
There’s no online widget for this one, but: when and if you’re in a position to safely* do so, think about something that normally triggers a strong unwanted emotional reaction. It doesn’t have to be something life-shattering, but just something that you feel in some way bad about. Hold this in your mind, sit with it, and practice mindfulness. The idea is to be able to hold the unpleasant idea in your mind, without becoming reactive to it, or escaping to more pleasant distractions. Build this up.
*if you perchance have PTSD, C-PTSD, or an emotional regulation disorder, you might want to talk this one through with a qualified professional first.
Creative Intelligence
Another important cognitive skill, and again, one that can be cultivated and grown.
The trick here is volume. A good, repeatable test is to think of a common object (e.g. a rock, a towel, a banana) and, within a time constraint (such as 15 minutes) list how many uses you can think of for that item.
Writer’s storytime: once upon a time, I was sorting through an inventory of medical equipment with a colleague, and suggested throwing out our old arterial clamps, as we had newer, better ones—in abundance. My colleague didn’t want to part with them, so I challenged him “Give me one use for these, something we could in some possible world use them for that the new clamps don’t do better, and we’ll keep them”. He said “Thumbscrews”, and I threw my hands up in defeat, saying “Fine!”, as he had technically fulfilled my condition.
What’s the hack to improve this one? Just more volume. Creativity, as it turns out, isn’t something we can expend—like a muscle, it grows the more we use it. And because the above test is repeatable (with different objects), you can track your progress.
And if you feel like using your grown creative muscle to write/paint/compose/etc your magnum opus, great! Or if you just want to apply it to the problem-solving of everyday life, also great!
In summary…
Our brain is a wonderful organ with many functions. Society expects us to lose these as we get older, but the simple, scientific truth is that we can not only maintain our cognitive function, but also enhance and grow it as we go.
Want to know more from today’s featured expert?
You might enjoy her book, “Smarter Tomorrow”, which we reviewed back in March
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: