Minimize Aging’s Metabolic Slump
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I know that metabolism slows with age, are there any waypoints or things to look out for? I don’t know whether I should be eating less, or doing less, or taking some other approach entirely. What’s recommended?❞
Age and sex count for a lot with this one! As metabolism is in large part directed by hormones:
- For men, declining testosterone (often from around 45 onwards) can result in a metabolic slump
- For women, declining estrogen with the menopause does have an effect, but progesterone is the bigger factor for metabolism in the sense you are talking about.
In both cases, simply taking more of those hormones can often help, but please of course speak with an endocrinologist if that seems like a possible option for you, as your circumstances (and physiology) may vary.
If you’d like to go to that conversation well-armed with information, here are some good starting points, by the way:
- The Testosterone Drop, & Topping Up Testosterone
- Menopausal HRT: Bioidentical vs Animal (It Makes A Difference!)
And if you’re wondering about the natural vs pharmaceutical approaches…
- What Does “Balance Your Hormones” Even Mean?
- What You Should Have Been Told About The Menopause Beforehand
About your metabolic base rate
We tend to think of “fast metabolism good, slow metabolism bad”, and that’s a reasonable general premise… but it’s not necessarily always so.
After all, if you could double your metabolism and keep it there all the time, without changing anything else, well… You’ve heard the phrase “burning the candle at both ends”? So, having at least some downtime is important too.
See for example: Sleep Deprivation & Diabetes Risk
What’s critical, when it comes to base metabolic rate, is that your body must be capable of adequately processing what you are putting into it. Because if your body can’t keep up with the input, it’ll just start storing the excess chemical energy in the quickest and easiest way possible.
…which is a fast track to metabolic disorder in general and type 2 diabetes in particular. For more on the science and mechanics of this, see:
How To Prevent And Reverse Type 2 Diabetes
As for portion sizes…
Your body knows what you need, so listen to it. There is no external source of knowledge that can tell you how much food you need better than your own body itself can tell you.
You may be wondering “how exactly do I listen to my body, though?”, in which case, check out:
The Kitchen Doctor: Interoception & Mindful Eating
As for exercise…
When you exercise, your metabolic rate temporarily increases. After most kinds of exercise, your metabolism slumps again afterwards to compensate.
There are two ways to avoid this:
- Exercise Less, Move More ← it’s about maximizing time spent not sitting still
- High Intensity Interval Training ← a special kind of exercise, the only one known to keep the metabolism running high for a couple of hours afterwards, with no counter-slump
…which makes it pretty effective indeed
Would you like this section to be bigger? If so, send us more questions!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Green Tea Can Benefit You (But Watch Out!)

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s not breaking news that green tea is healthy in moderation. But there’s a lot that many people don’t know, too.
A timeless classic, unless…
Of the various true teas, there are different possible metrics we may go by and different ways we could weight them, but the popular consensus is that green tea offers the strongest and most consistent health benefits, while traditionally brewed tea of any type is broadly safe and beneficial.
In terms of polyphenols, green tea retains high catechin levels due to minimal fermentation, while black tea contains theaflavins and thearubigins from oxidation; theanine and of course caffeine also contribute to physiological effects, and we’ve written about those in fair detail here:
- L-Theanine: What’s The Tea?
- Neuropsychologist Explains What She’s Got Out Of 6 Years Taking L-Theanine
- Caffeine: Cognitive Enhancer Or Brain-Wrecker?
As for the rest of the benefits, they are manifold, including:
- Cardiovascular protection: regular green tea intake—e.g. 2–3 cups per day—is linked to lower cardiovascular and all-cause mortality; polyphenols reduce LDL cholesterol, improve endothelial function, lower blood pressure, and reduce oxidative stress.
- Anticancer potential: findings in humans are mixed, but meta-analyses support reduced risks of oral, lung (in women), and colon cancers with regular green tea consumption.
- Weight and metabolic effects: green tea and catechin-rich preparations show modest, consistent reductions in body weight, fat mass, LDL cholesterol, and oxidative stress; cohort studies suggest lower diabetes risk, though other studies have not shown benefits, so in other words, the science is still a work-in-progress on this one.
- Neuroprotective effects: habitual tea drinking is associated with reduced cognitive decline, better cognitive performance, and lower Alzheimer’s-related biomarkers, with strongest benefits in adults aged 50 to 69. It’s also generally found to be beneficial for stress management.
- Muscle health benefits in aging: a surprising and much less well-known one, but catechin-rich green tea can help maintain or increase muscle mass and improve grip strength in older adults or those with sarcopenia in general.
- Inflammation and immunity: tea polyphenols lower inflammatory markers and oxidative stress, help reduce uric acid levels, and show antibacterial and antiviral activity (including against influenza, HPV, and SARS-CoV-2), though most antiviral data come from in vitro studies.
Rather than bombard you with sources for all of the above, we’ll drop a link to one excellent paper that covers them all:
Beneficial health effects and possible health concerns of tea consumption: a review
Wait, what’s that about “and possible health concerns”?
The problems highlighted by the above-linked studies are threefold, but the good news is that they can all be avoided, so long as you’re aware of them:
- Brew it yourself: bottled and bubble teas often contain sugars, artificial sweeteners, or preservatives that negate benefits, and to make things worse, processing and storage markedly reduce catechin content. So, just buy tea leaves and brew your own.
- Check safety/quality certifications: some teas contain pesticide residues, heavy metals, or microplastics; typical exposure is low risk, but long-term heavy consumption could run into problems if the supplier isn’t good.
- Timing matters for nutrient absorption: generous tea intake can inhibit non-heme iron and calcium absorption, so it’s best to avoid drinking your greens at the same time as eating your greens (leafy greens being good sources of non-heme iron and calcium).
Some people can also run into other problems that are more person-specific; we touched on that briefly here a few years ago: Green Tea Allergies and Capsules
Want to learn more?
As we mentioned up top, the other kinds of teas have their benefits too.
You can see which is best for what, here: Which Tea Is Best For The Health, By Science?
Enjoy!
Share This Post
-
Artichoke vs Carrots – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing artichoke to carrots, we picked the artichoke.
Why?
Both are great, but still, it wasn’t close:
In terms of macros, the artichoke has nearly 2x the fiber and more than 3x the protein, for the same carbs; a clear first-round win for artichoke.
In the category of vitamins, artichoke has more of vitamins B1, B2, B3, B5, B7, B9, C, and K, while carrots have more of vitamins A, B6, and E, giving artichoke an 8:3 win in this second round.
Looking at minerals, artichoke has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while carrots are not higher in any minerals; a complete win for artichoke here.
Adding up the sections makes for a clear overall win for artichoke, but by all means enjoy either or both, as diversity is best!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Share This Post
-
Yes, you still need to use sunscreen, despite what you’ve heard on TikTok
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Summer is nearly here. But rather than getting out the sunscreen, some TikTokers are urging followers to chuck it out and go sunscreen-free.
They claim it’s healthier to forgo sunscreen to get the full benefits of sunshine.
Here’s the science really says.

Karolina Grabowska/Pexels How does sunscreen work?
Because of Australia’s extreme UV environment, most people with pale to olive skin or other risk factors for skin cancer need to protect themselves. Applying sunscreen is a key method of protecting areas not easily covered by clothes.
Sunscreen works by absorbing or scattering UV rays before they can enter your skin and damage DNA or supportive structures such as collagen.
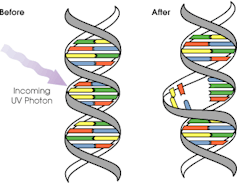
When UV particles hit DNA, the excess energy can damage our DNA. This damage can be repaired, but if the cell divides before the mistake is fixed, it causes a mutation that can lead to skin cancers.
The energy from a particle of UV (a photon) causes DNA strands to break apart and reconnect incorrectly. This causes a bump in the DNA strand that makes it difficult to copy accurately and can introduce mutations. NASA/David Herring The most common skin cancers are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). Melanoma is less common, but is the most likely to spread around the body; this process is called metastasis.
Two in three Australians will have at least one skin cancer in their lifetime, and they make up 80% of all cancers in Australia.
Around 99% of skin cancers in Australia are caused by excessive exposure to UV radiation.
Excessive exposure to UV radiation also affects the appearance of your skin. UVA rays are able to penetrate deep into the skin, where they break down supportive structures such as elastin and collagen.
This causes signs of premature ageing, such as deep wrinkling, brown or white blotches, and broken capillaries.
Sunscreen can help prevent skin cancers
Used consistently, sunscreen reduces your risk of skin cancer and slows skin ageing.
In a Queensland study, participants either used sunscreen daily for almost five years, or continued their usual use.
At the end of five years, the daily-use group had reduced their risk of squamous cell carcinoma by 40% compared to the other group.
Ten years later, the daily use group had reduced their risk of invasive melanoma by 73%
Does sunscreen block the health-promoting properties of sunlight?
The answer is a bit more complicated, and involves personalised risk versus benefit trade-offs.
First, the good news: there are many health benefits of spending time in the sun that don’t rely on exposure to UV radiation and aren’t affected by sunscreen use.
Sunscreen only filters UV rays, not all light. Ron Lach/Pexels Sunscreen only filters UV rays, not visible light or infrared light (which we feel as heat). And importantly, some of the benefits of sunlight are obtained via the eyes.
Visible light improves mood and regulates circadian rhythm (which influences your sleep-wake cycle), and probably reduces myopia (short-sightedness) in children.
Infrared light is being investigated as a treatment for several skin, neurological, psychiatric and autoimmune disorders.
So what is the benefit of exposing skin to UV radiation?
Exposing the skin to the sun produces vitamin D, which is critical for healthy bones and muscles.
Vitamin D deficiency is surprisingly common among Australians, peaking in Victoria at 49% in winter and being lowest in Queensland at 6% in summer.
Luckily, people who are careful about sun protection can avoid vitamin D deficiency by taking a supplement.
Exposing the skin to UV radiation might have benefits independent of vitamin D production, but these are not proven. It might reduce the risk of autoimmune diseases such as multiple sclerosis or cause release of a chemical that could reduce blood pressure. However, there is not enough detail about these benefits to know whether sunscreen would be a problem.
What does this mean for you?
There are some benefits of exposing the skin to UV radiation that might be blunted by sunscreen. Whether it’s worth foregoing those benefits to avoid skin cancer depends on how susceptible you are to skin cancer.
If you have pale skin or other factors that increase you risk of skin cancer, you should aim to apply sunscreen daily on all days when the UV index is forecast to reach 3.
If you have darker skin that rarely or never burns, you can go without daily sunscreen – although you will still need protection during extended times outdoors.
For now, the balance of evidence suggests it’s better for people who are susceptible to skin cancer to continue with sun protection practices, with vitamin D supplementation if needed.
Katie Lee, PhD Candidate, Dermatology Research Centre, The University of Queensland and Rachel Neale, Principal research fellow, QIMR Berghofer Medical Research Institute
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post




Related Posts
-

Moving Through Cancer – by Dr. Kathryn Schmitz
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We all know exercise is good for most things, but cancer is complicated, so… What should we do? Should we take it easy? Exercise more? Conserve energy? Can speeding up our metabolism (generally considered good) commensurately speed up the cancer (bad)?
Dr. Kathryn Schmitz is an expert in sports medicine for cancer patients, with decades of experience in that field.
Then, when her wife was diagnosed with an aggressive stage 3 cancer, Dr. Schmitz (of course) applied everything she knew, and doubled-down going through all available research with a fine-toothed comb. What was already her career, became her reason for living.
Prior to her wife getting cancer, Dr. Schmitz had already overturned the medical convention of yesteryear; it was her own research that changed mainstream policies on exercise recommendation for breast cancer patients specifically (previous advice was: avoid upper body exercise). That was about six years before her wife’s cancer diagnosis, which is at time of writing, 9 years ago now (happily, she is doing fine now, and is officially cancer-free* in the sense of “no evidence of disease”), and she’s only continued to increase her research since, to share it with us.
*this term is often avoided due to the technically non-zero chance of cancer returning, but the author uses it in this case, so we’ll use it here too.
This book covers many different kinds of cancer, with exercise protocols tailored for each, and also covers exercise in the context of surgery, chemotherapy and other infusion therapies, radiation therapies, hormonal therapies, and more.
On that note, she makes the distinction between “prehabilitation” (getting into the best possible condition before treatment) and post-treatment recovery protocols, and how to balance getting adequate exercise with getting adequate rest, during treatments of the ongoing kind (i.e. pretty much anything apart from surgery—since during surgery, one will certainly not be exercising).
All of this is very evidence-based, as one might expect from someone with her background in both academia and practice, and as such she refers to many studies throughout.
This is mostly a practical book, with direct instructions on what to do and how to do it and how to tailor it to your specific cancer/situation, with day-by-day, week-by-week plans, coupled with frequent reminders of such things as “but this adds to your stress, don’t do it; managing your stress is more important”, and “if you are unable to do the exercise on any given day, or must do a modified version, or cut your exercise short, just log that in your exercise journal and try again tomorrow”, and so forth.
That side of things is not limited to just disclaimers, either—she’s very aware, from her own experience with her wife, that fighting cancer is an emotional battle as much as a physical one, and she gives genuine attention to that too.
Bottom line: if you or a loved one has or has had cancer, this book can help survivorship and recovery, with highly specialised advice from someone who is not only a world-class expert in her field, but also very clearly cares very deeply.
Click here to check out Moving Through Cancer, and move through cancer!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Inverse Vaccines for Autoimmune Diseases
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Inverse Vaccines for Autoimmune Diseases

This is Dr. Jeffrey Hubbell. He’s a molecular engineer, with a focus on immunotherapy, immune response, autoimmune diseases, and growth factor variants.
He’s held 88 patents, and was the recipient of the Society for Biomaterials’ Founders Award for his “long-term, landmark contributions to the discipline of biomaterials”, amongst other awards and honours that would make our article too long if we included them all.
And, his latest research has been about developing…
Inverse Vaccines
You may be thinking: “you mean diseases; he’s engineering diseases?”
And no, it’s not that. Here’s how it works:
Normally in the case of vaccine, it’s something to tell the body “hey, if you see something that looks like this, you should kill it on sight” and the body goes “ok, preparing countermeasures according to these specifications; thanks for the heads-up”
In the case of an inverse vaccine, it’s the inverse. It’s something to tell the body “hey, this thing you seem to think is a threat, it’s actually not, and you should leave it alone”.
Why this matters for people with autoimmune diseases
Normally, autoimmune diseases are treated in one or more of the following ways:
- Dampen the entire immune system (bad for immunity against actual diseases, obviously, and is part of why many immunocompromised people have suffered and died disproportionately from COVID, for example)
- Give up and find a workaround (a good example of this is Type 1 Diabetes, and just giving up on the pancreas not being constantly at war with itself, and living on exogenous insulin instead)
Neither of those are great.
What inverse vaccines do is offer a way to flag the attacked-in-error items as acceptable things to have in the body. Those might be things that are in our body by default, as in the case of many autoimmune diseases, or they may even be external items that should be allowed but aren’t, as in the case of gluten, in the context of Celiac disease.
The latest research is not yet accessible for free, alas, but you can read the abstract here:
Or if you prefer a more accessible pop-science approach, here’s a great explanatory article:
“Inverse vaccine” shows potential to treat multiple sclerosis and other autoimmune diseases
Where can we get such inverse vaccines?
❝There are no clinically approved inverse vaccines yet, but we’re incredibly excited about moving this technology forward❞
~ Dr. Jeffrey Hubbell
But! Lest you be disappointed, you can get in line already, in the case of the Celiac disease inverse vaccine, if you’d like to be part of their clinical trial:
Click here to see if you are eligible to be part of their clinical trial
If you’re not up for that, or if your autoimmune disease is something else (most of the rest of their research is presently focusing on Multiple Sclerosis and Type 1 Diabetes), then:
- The phase 1 MS trial is currently active, estimated completion in summer 2024.
- They are in the process of submitting an investigational new drug (IND) application for Type 1 Diabetes
- This is the first step to starting clinical safety and efficacy trials
…so, watch this space!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

8 Signs Of Iodine Deficiency You Might Not Expect
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Health Coach Kait (BSc Nutrition & Exercise) is a certified health and nutrition coach, and today she’s here to talk about iodine—which is important for many of our body functions, from thyroid hormone production to metabolic regulation to heart rate management, as well as more superficial-but-important-too things like our skin and hair.
Kait’s hitlist
Here’s what she recommends we look out for:
- Swollen neck: even a slightly swollen neck might indicate low iodine levels (this is because that’s where the thyroid glands are)
- Hair loss: iodine is needed for healthy hair growth, so a deficiency can lead to hair loss / thinning hair
- Dry and flaky skin: with iodine’s role in our homeostatic system not being covered, our skin can dry out as a result
- Feeling cold all the time: because of iodine’s temperature-regulating activities
- Slow heart rate: A metabolic slump due to iodine deficiency can slow down the heart rate, leading to fatigue and weakness (and worse, if it persists)
- Brain fog: trouble focusing can be a symptom of the same metabolic slump
- Fatigue: this is again more or less the same thing, but she said eight signs, so we’re giving you the eight!
- Irregular period (if you normally have such, of course): because iodine affects reproductive hormones too, an imbalance can disrupt menstrual cycles.
For more on each of these, as well as how to get more iodine in your diet, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Further reading
You might also like to read:
- A Fresh Take On Hypothyroidism
- Foods For Managing Hypothyroidism (incl. Hashimoto’s)
- Eat To Beat Hyperthyroidism!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: