What’s Your Plant Diversity Score?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We speak often about the importance of dietary diversity, and of that, especially diversity of plants in one’s diet, but we’ve never really focused on it as a main feature, so that’s what we’re going to do today.
Specifically, you may have heard the advice to “eat 30 different kinds of plants per week”. But where does that come from, and is it just a number out of a hat?
The magic number?
It is not, in fact, a number out of a hat. It’s from a big (n=11,336) study into what things affect the gut microbiome for better or for worse. It was an observational population study, championing “citizen science” in which volunteers tracked various things and collected and sent in various samples for analysis.
The most significant finding of this study was that those who consumed more than 30 different kinds of plants per week, had a much better gut microbiome than those who consumed fewer than 10 different kinds of plants per week (there is a bell curve at play, and it gets steep around 10 and 30):
American Gut: an Open Platform for Citizen Science Microbiome Research
Why do I care about having a good gut microbiome?
Gut health affects almost every other kind of health; it’s been called “the second brain” for the various neurotransmitters and other hormones it directly makes or indirectly regulates (which in turn affect every part of your body), and of course there is the vagus nerve connecting it directly to the brain, impacting everything from food cravings to mood swings to sleep habits.
See also:
Any other benefits?
Yes there are! Let’s not forget: as we see often in our “This or That” section, different foods can be strong or weak in different areas of nutrition, so unless we want to whip out a calculator and database every time we make food choices, a good way to cover everything is to simply eat a diverse diet.
And that goes not just for vitamins and minerals (which would be true of animal products also), but in the case of plants, a wide range of health-giving phytochemicals too:
Measuring Dietary Botanical Diversity as a Proxy for Phytochemical Exposure
Ok, I’m sold, but 30 is a lot!
It is, but you don’t have to do all 30 in your first week of focusing on this, if you’re not already accustomed to such diversity. You can add in one or two new ones each time you go shopping, and build it up.
As for “what counts”: we’re counting unprocessed or minimally-processed plants. So for example, an apple is an apple, as are dried apple slices, as is apple sauce. Any or all of those would count as 1 plant type.
Note also that we’re counting types, not totals. If you’re having apple slices with apple sauce, for some reason? That still only counts as 1.
However, while apple sauce still counts as apples (minimally processed), you cannot eat a cake and say “that’s 2 because there was wheat and sugar cane somewhere in its dim and distant history”.
Nor is your morning espresso a fruit (by virtue of coffee beans being the fruit of the plant, botanically speaking). However, it would count as 1 plant type if you eat actual coffee beans—this writer has been known to snack on such; they’re only healthy in very small portions though, because their saturated fat content is a little high.
You, however, count grains in general, as well as nuts and seeds, not just fruits and vegetables. As for herbs and spices, they count for ¼ each, except for salt, which might get lumped in with spices but is of course not a plant.
How to do it
There’s a reason we’re doing this in our Saturday Life Hacks edition. Here are some tips for getting in far more plants than you might think, a lot more easily than you might think:
- Buy things ready-mixed. This means buying the frozen mixed veg, the frozen mixed chopped fruit, the mixed nuts, the mixed salad greens etc. This way, when you’re reaching for one pack of something, you’re getting 3–5 different plants instead of one.
- Buy things individually, and mix them for storage. This is a more customized version of the above, but in the case of things that keep for at least a while, it can make lazy options a lot more plentiful. Suddenly, instead of rice with your salad you’re having sorghum, millet, buckwheat, and quinoa. This trick also works great for dried berries that can just be tipped into one’s morning oatmeal. Or, you know, millet, oats, rye, and barley. Suddenly, instead of 1 or 2 plants for breakfast you have maybe 7 or 8.
- Keep a well-stocked pantry of shelf-stable items. This is good practice anyway, in case of another supply-lines shutdown like at the start of the COVID-19 pandemic. But for plant diversity, it means that if you’re making enchiladas, then instead using kidney beans because that’s what’s in the cupboard, you can raid your pantry for kidney beans, black beans, pinto beans, fava beans, etc etc. Yes, all of them; that’s a list, not a menu.
- Shop in the discount section of the supermarket. You don’t have shop exclusively there, but swing by that area, see what plants are available for next to nothing, and buy at least one of each. Figure out what to do with it later, but the point here is that it’s a good way to get suggestions of plants that you weren’t actively looking for—and novelty is invariably a step into diversity.
- Shop in a different store. You won’t be able to beeline the products you want on autopilot, so you’ll see other things on the way. Also, they may have things your usual store doesn’t.
- Shop in person, not online—at least as often as is practical. This is because when shopping for groceries online, the store will tend to prioritize showing you items you’ve bought before, or similar items to those (i.e. actually the same item, just a different brand). Not good for trying new things!
- Consider a meal kit delivery service. Because unlike online grocery shopping, this kind of delivery service will (usually) provide you with things you wouldn’t normally buy. Our sometimes-sponsor Purple Carrot is a fine option for this, but there are plenty of others too.
- Try new recipes, especially if they have plants you don’t normally use. Make a note of the recipe, and go out of your way to get the ingredients; if it seems like a chore, reframe it as a little adventure instead. Honestly, it’s things like this that keep us young in more ways than just what polyphenols can do!
- Hide the plants. Whether or not you like them; hide them just because it works in culinary terms. By this we mean; blend beans into that meaty sauce; thicken the soup with red lentils, blend cauliflower into the gravy. And so on.
One more “magic 30”, while we’re at it…
30g fiber per day makes a big (positive) difference to many aspects of health. Obviously, plants are where that comes from, so there’s a big degree of overlap here, but most of the tips we gave are different, so for double the effectiveness, check out:
Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Scrolling on the toilet increases your risk of haemorrhoids, new study shows

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many of us are guilty of scrolling our smartphones on the toilet. But a new study from the United States, published today, has found this habit may increase your risk of developing haemorrhoids by up to 46%.
So, what’s the link? How can time on your phone lead to these painful lumps in and around your anus? Here’s what we know.

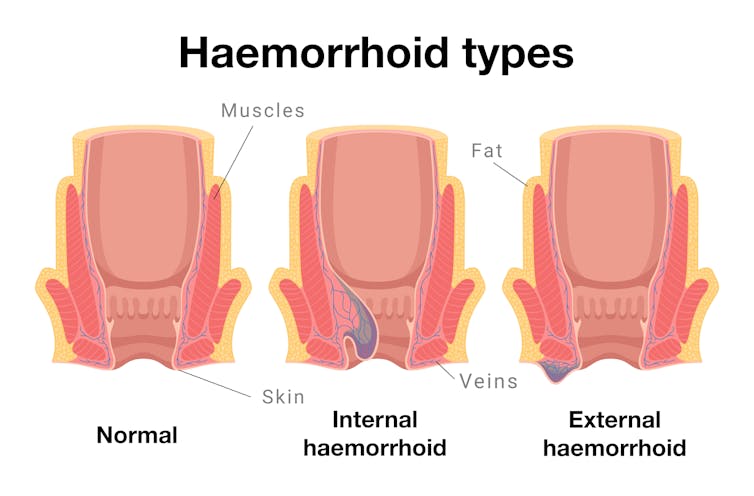
Arisara_Tongdonnoi/Getty What are haemorrhoids?
Every healthy person has haemorrhoids, sometimes called piles. They are columns of cushioned tissue and blood vessels found close to the opening of the anus.
We don’t notice haemorrhoids until they’re symptomatic. Aleksandr Kharitonov/Getty Haemorrhoids have a really important role in maintaining bowel continence or, to put it simply, keeping your poo in.
When all is well, we don’t notice them. But haemorrhoids can get swollen and this can lead to symptoms such as pain, bleeding or feeling a lump just inside your anus (internal haemorrhoids) or protruding outside (external haemorrhoids).
So when someone “has haemorrhoids”, it means they have become inflamed or symptomatic.
This is extremely common: more than one in two of us will experience symptomatic haemorrhoids at some point in our lives.
You are more likely to get haemorrhoids if you:
- are older (over 45)
- are pregnant
- are overweight
- have persistent constipation or diarrhoea
- regularly lift heavy objects
- spend a lot of time on the toilet.
The link between toilet time and haemorrhoids
Prolonged sitting in general has not been linked to developing haemorrhoids.
However, a standard toilet seat – unlike a chair or couch – has a large internal opening that provides no support for the pelvic floor (the group of muscles and ligaments that support the bladder, bowel and uterus).
Prolonged sitting on a toilet seat is believed to increase pressure inside the pelvic floor and lead to blood pooling in the vascular cushions of the anus. This makes haemorrhoids more likely to develop.
What the new study looked at
The new US study recruited 125 adults, aged 45 and older, who were undergoing a colonoscopy at Beth Israel Deaconess Medical centre.
Researchers surveyed them about their smartphone habits while using the toilet, including how often they checked their phone and for how long. Participants also reported on other behaviours such as straining, their fibre intake, and how much physical activity they did.
The researchers recorded whether they had haemorrhoids. Since the participants were all having a colonoscopy, the presence of internal haemorrhoids could be directly confirmed visually.
What did the study show?
Two-thirds (66%) of all participants used smartphones while on the toilet. The most common activity was reading news (54.3%), followed by social media (44.4%).
Those who used their smartphones spent longer on the toilet than those who didn’t. More than one in three (37.3%) toilet smartphone users spent over five minutes on the toilet, compared to just over one in 20 (7%) of those who didn’t use their smartphones.
The smartphone users had a 46% higher risk of haemorrhoids, compared to those who didn’t use their smartphone. To calculate this, researchers took into account other known risk factors for haemorrhoids such as gender, age, body mass index, exercise activity, straining and fibre intake.
However, unlike some other research, this study did not find a link between straining and haemorrhoids.
As a result, the researchers concluded that time spent on the toilet poses a more significant risk for haemorrhoids than straining. However, we can’t rule out straining as a risk factor, based on one study.
Some other limitations to consider
The study relied on participants remembering whether or not they strained, and how long they spent on the toilet.
This kind of recall is subjective, and may also be influenced by taking part in the study. For example, if the participants thought they had haemorrhoids, they may be more likely to report straining.
The study’s small sample size and the participants’ age (all over 45) also mean it is unlikely to be representative of the broader population.
Toilet sitting time
The new study is not the first to study the link between time spent on the toilet and developing haemorrhoids. In 2020, a Turkish study found spending more than five minutes on the toilet was associated with haemorrhoids.
Another 2020 study from Italy of 52 people with diagnosed internal or external haemorrhoids noted the longer they spent on the toilet, the more severe their haemorrhoids.
So, what are we doing on the toilet?
Defaecation itself usually doesn’t take long. One study found it took healthy adults an average two minutes when sitting, but only 51 seconds when squatting.
The majority of “toilet sitting time” usually means just that – sitting on the toilet, doing other activities aside from pooing (or weeing).
One 2008 study from Israel surveyed 500 adults and found more than half (52.7%) read books or newspapers while on the toilet. It also found toilet readers spent significantly more time on the toilet.
How to avoid haemorrhoids
The usual advice is to increase the amount of fibre in your diet (eating more fruit, vegetables and wholegrains) and ensure you drink enough water. This makes it easier to pass a stool and reduces straining – which you should also try to avoid.
However, the new research confirms previous evidence that cutting down toilet sitting time may also help. So, avoiding distractions by leaving your smartphone outside the bathroom is a good idea (and as a bonus, will expose your device to fewer germs).
If you have any concerning symptoms, such as blood in your stool, a new lump in the anal region, or pain when passing a bowel motion then you should see your local doctor for further investigations and treatment.
Vincent Ho, Associate Professor and Clinical Academic Gastroenterologist, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Can You Step Backwards Without Your Foot Or Torso Turning Out?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Walking backwards is often overlooked, but research shows it can enhance forward walking, especially in stroke patients; it has other benefits for everyone else, too. The physiotherapists at Fitness4Life Physical Therapy explain:
…and one step back
How it works: walking backwards heightens proprioception and stimulates muscles, improving balance and posture. Additionally, our daily lives tend to involve forward-leaning postures, causing upper back bending, and walking backwards helps counterbalance this.
Extra benefits: training to walk backwards can reduce the risk of falls, as stepping back is a common movement that is often untrained.
Exercise: try doing backwards lunges, to assess your skill and balance while moving backward. If foot rotation or torso rotation occurs during the exercise, then there’s room for improvement. Correcting these movements is then simply a matter of practicing backward lunges without turning.
10almonds tip: any exercise is only as good as your will to actually do it. For this reason, dancing is a great exercise in this case, as almost all forms of dance involve stepping backwards (in order to have steps without travelling somewhere, forwards steps are usually balanced with backwards ones)
For more on all this, plus a visual demonstration of the exercise, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Fall Special ← About how to avoid falling, and how to avoid (and failing that, at least minimize) injury if you do fall. If you think this only happens to other/older people, remember, there’s a first time for everything, so it is better to be prepared in advance!
Take care!
Share This Post
-
Basic Baked Tofu
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One of the main criticisms of tofu is that it is tasteless. Well, so is flour, but you’re not supposed to eat it plain, and the same goes for tofu. It’s a blank canvas that you get to decide what to do with—not to mention, it’s a canvas that’s very high in protein, and is a complete protein too, containing all essential amino acids. Anyway, here’s a starter recipe that elevates tofu from “nutrition” to “nutritious tasty snack”!
We were going to do a fancier recipe today, but considered that it might be judicious to cover this basic element first, that can be incorporated into a larger recipe later, a bit like we have done with recipes such as our Tasty Versatile Rice, and Plant-Based Healthy Cream Cheese (amongst others).
You will need
- 1 block of extra-firm tofu; these are quite standardized in size; it should be about 12oz; don’t worry if it’s a little more or less.
- 2 tbsp arrowroot powder (or potato starch if you don’t have arrowroot)
- 1½ tbsp extra virgin olive oil
- 1 tbsp nutritional yeast
- 1 tsp black pepper
- ½ tsp MSG or 1 tsp low-sodium salt
- Optional: ½ tsp garlic powder
- Optional: ½ tsp ground turmeric
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 425ºF / 220ºC.
2) Press the tofu for about 15 minutes (to remove excess moisture), using a tofu press if you have one. If you don’t, then here is an example product on Amazon, or alternatively, you can go with the time-honored tradition of cutting the tofu lengthways into slabs, and wrapping it in a lint-free kitchen towel or muslin cloth, and pressing it with heavy books. We don’t recommend pressing for more than about 15 minutes, as you are going to bake the tofu so you don’t want it too dry going in.
3) Cut the tofu into cubes. Size is up to you, but half-inch cubes are very respectable.
4) Combine the tofu cubes in a big bowl with the oil and seasonings, including the nutritional yeast but not the arrowroot powder or potato starch yet. You will need to toss them gently (very gently; they are fragile!) to combine.
5) Add the arrowroot powder or potato starch, and again toss gently to combine. We do this last, because it would stop the other things from sticking properly if we did it earlier.
6) Arrange the tofu on a baking tray lined with baking paper, in a single layer so that the cubes don’t touch. Bake for 15 minutes, turn them over, and bake for a further 15 minutes on the other side. They should now be golden and crisp, but if they’re not, just give them a little more time.
7) Serve as a snack, or set aside for whatever else you’re going to do with them in a larger more complex recipe.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Tofu vs Seitan – Which is Healthier?
- Plant vs Animal Protein: Head to Head
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Share This Post




Related Posts
-

Tempeh vs Tofu – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing tempeh to tofu, we picked the tempeh.
Why?
Per 100g, tempeh has about 1.5x as many calories, about 2x as much protein, about 3x as much fiber, and about 4x the carbohydrates.
Which latter sounds like a lot, but really, the amounts here are small—tempeh is under 12% carbohydrates, and most of that is treated by the body as fiber (e.g. it’s a resistant starch).
Both have no sugar, and both have more or less the same (tiny) amount of fat.
Micronutrients, you ask? As they’re both made from soybeans, the micronutrient profiles are similar, but exact amounts will depend on the method used, so by all means check labels if comparing products in store. By and large, there’s usually not much difference, though.
You can see sample stats here:
In summary
Both are great, and/but tempeh is the more nutrient-dense of the two.
Therefore, tempeh is the healthier option, unless you are on a very strictly calorie-controlled diet, in which case, tofu will give you more quantity per calorie.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
New cases of meningococcal disease have been detected. What are the symptoms? And who can get vaccinated?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Two Tasmanian women have been hospitalised with invasive meningococcal disease, bringing the number of cases nationally so far this year to 48. Health authorities are urging people to watch for symptoms and to check if they’re eligible for vaccination.
Invasive meningococcal disease is a rare but life-threatening illness caused by the bacteria Neisseria meningitidis. Invasive means the infection spreads rapidly through the blood and into your organs.
Early emergency medical care is important for survival and to reduce the chance of long-term complications. Even in those who survive, up to 30% suffer permanent cognitive, physical or psychological disabilities.
Thankfully, vaccines are available to protect against it.
How do you catch it?
Around one in ten people carry the meningococcal bacteria in their nose or throats.
The bacteria does not easily pass from person to person by breathing the same air or sharing drinks or food – and the bacteria do not survive well outside the human body.
It is spread through close and prolonged contact of oral and respiratory secretions, such as saliva, from others who live in your household or through deep, intimate kissing.
There is no way to know if you carry the bacteria, as carriers don’t have symptoms.
Who is most at risk?
Meningococcal disease can affect anyone.
But infants under one, adolescents and young adults aged 15–25 years, and people without a spleen or who are immunosuppressed are at a higher risk of developing invasive disease.
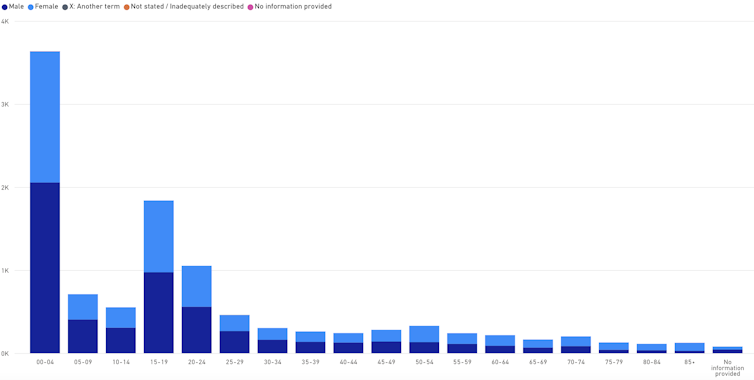
Meningococcal disease notifications by age and sex
Babies and teens are more likely to contract the disease than other age groups. National Notifiable Disease Surveillance System Although sensitive to common antibiotics such as penicillin, the meningococcal bacteria can cause severe infection and death in a matter of hours. The difficulty in picking up meningococcal disease early is that, early on, it can mimic common viral illnesses that people would recover from without any treatment.
Most people experience a sudden onset of fever, difficulty looking at light and/or a rash. The rash is non-blanching, meaning it doesn’t fade when you apply pressure to it. But early in the illness, it can start out as a blanching rash that fades with pressure.
Young infants may also become irritable, have difficulty waking up, or refuse to feed.
The bacteria usually causes a meningitis – inflammation of the lining around the brain and spinal cord – or a bloodstream infection, called septicemia or sepsis. But sometimes it can cause an infection of the bone, lungs (pneumonia) or eyes (conjunctivitis).
Protection against different strains
There are 13 types of meningococcal bacteria that cause invasive disease, but types A, B, C, W and Y cause the most illness.
The rapid disease progression occurs because the bacteria has a sugar capsule which allows it to evade the immune system.
But each of the 13 types has its own unique capsule. So immunity to one strain does not offer immunity to other strains.
Currently, two types of vaccines are available: a vaccine that protects against meningococcal A, C, W and Y (MenACWY); and another vaccine that protects against meningococcal B.
The vaccines are manufactured differently and therefore have different mechanisms of protection.
The MenACWY vaccine uses parts of the sugar capsule within each of the bacteria and joins them to a protein. This is called a “conjugate vaccine” and allows for a better immune response, especially in young infants.
The MenB vaccine does not contain the sugar capsule but includes four other proteins from the surface of the meningococcal B bacteria.
Both vaccines are registered for all people aged six months and older, and are safe for immunocompromised people.
MenACWY vaccine
The MenACWY vaccine is funded under the National Immunisation Program, and given for free, to all infants aged 12 months. There is also a free catch-up program for teens in Year 10.
The MenACWY vaccine protects against disease and also decreases the bacteria load in the throat, reducing the likelihood of transmission to others.
MenB vaccine
The MenB vaccine recommended for all infants aged six weeks or more. But it’s only available for free to infants in South Australia and Queensland, through state-based programs, and to Aboriginal and Torres Strait Islander infants nationally, via the National Immunisation Program.
Parents of non-Indigenous infants in other states will pay around A$220–270 for two doses of the MenB vaccine.
The MenB vaccine is highly protective against invasive disease for the person who receives the vaccine. But it does not eradicate the bacteria from the throat, nor does it decrease spread of the bacteria to others.
Reducing meningococcal disease
Other people who are at high risk of meningococcal exposure are also recommended for vaccination: people without a functional spleen, those with certain immunocompromising conditions, certain travellers and some lab workers.
Since the rollout of the conjugate MenC vaccine in 2001 and the MenACWY in 2018, rates of invasive meningococcal disease have dropped dramatically, from 684 cases in 2002, to 136 cases in 2024. The most common strain to cause disease is now meningococcal B.
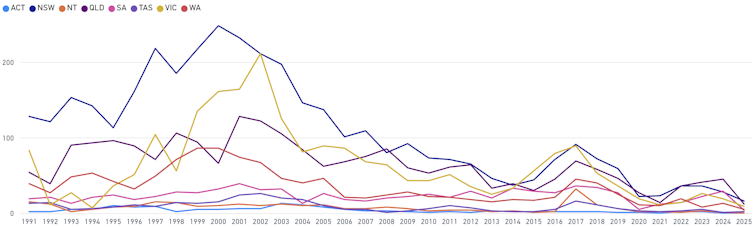
Meningococcal notifications by jurisdiction
Vaccination has reduced case numbers. National Notifiable Disease Surveillance System Another reason for adults to get vaccinated
The MenB vaccine has also been shown to lower rates of another bacterial infection, gonorrhoea, by 33–47%. This is because the gonococcal bacteria is closely related and shares similar surface protein structures to meningococcal bacteria.
In Australia, rates of gonorrhea have doubled over the past ten years , with higher rates among young Aboriginal and Torres Islander people.
The Northern Territory began offering the vaccine to people aged 14 to 19 last year as part of a research trial.
Further research is underway in Australia to better understand the meningococcal bacteria, its capability to evade the immune system and the cross protection against gonorrhoea.
Archana Koirala, Paediatrician and Infectious Diseases Specialist; Clinical Researcher, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Apricots vs Oranges – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apricots to oranges, we picked the apricots.
Why?
Both are great, and it was close!
In terms of macros, apricots have more protein while oranges have more carbs and fiber, the ratio of of which means that apricots have the slightly lower glycemic index, though really, nobody is getting metabolic disease from eating whole fruit. All in all, we’ll call this category a tie.
In the category of vitamins, apricots have more of vitamins A, B3, E, and K, while oranges have more of vitamins B1, B9, C, and choline, meaning another tie in this category.
When it comes to minerals, apricots have more copper, iron, magnesium, manganese, phosphorus, potassium, and zinc, while oranges have more calcium and selenium. A win for apricots, then!
In terms of beneficial phytochemicals, apricots have more, and you can read about some of them in the link below.
Adding up the sections makes for an overall win for apricots, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Top 8 Fruits That Prevent & Kill Cancer
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: