Foods for Stronger Bones
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
This newsletter has been growing a lot lately, and so have the questions/requests, and we love that! In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
Q: Foods that help build stronger bones and cut inflammation? Thank you!
We’ve got you…
For stronger bones / To cut inflammation
That “stronger bones” article is about the benefits of collagen supplementation for bones, but there’s definitely more to say on the topic of stronger bones, so we’ll do a main feature on it sometime soon!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cheeky diet soft drink getting you through the work day? Here’s what that may mean for your health

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many people are drinking less sugary soft drink than in the past. This is a great win for public health, given the recognised risks of diets high in sugar-sweetened drinks.
But over time, intake of diet soft drinks has grown. In fact, it’s so high that these products are now regularly detected in wastewater.
So what does the research say about how your health is affected in the long term if you drink them often?

Breakingpic/Pexels What makes diet soft drinks sweet?
The World Health Organization (WHO) advises people “reduce their daily intake of free sugars to less than 10% of their total energy intake. A further reduction to below 5% or roughly 25 grams (six teaspoons) per day would provide additional health benefits.”
But most regular soft drinks contain a lot of sugar. A regular 335 millilitre can of original Coca-Cola contains at least seven teaspoons of added sugar.
Diet soft drinks are designed to taste similar to regular soft drinks but without the sugar. Instead of sugar, diet soft drinks contain artificial or natural sweeteners. The artificial sweeteners include aspartame, saccharin and sucralose. The natural sweeteners include stevia and monk fruit extract, which come from plant sources.
Many artificial sweeteners are much sweeter than sugar so less is needed to provide the same burst of sweetness.
Diet soft drinks are marketed as healthier alternatives to regular soft drinks, particularly for people who want to reduce their sugar intake or manage their weight.
But while surveys of Australian adults and adolescents show most people understand the benefits of reducing their sugar intake, they often aren’t as aware about how diet drinks may affect health more broadly.
Diet soft drinks contain artificial or natural sweeteners. Vintage Tone/Shutterstock What does the research say about aspartame?
The artificial sweeteners in soft drinks are considered safe for consumption by food authorities, including in the US and Australia. However, some researchers have raised concern about the long-term risks of consumption.
People who drink diet soft drinks regularly and often are more likely to develop certain metabolic conditions (such as diabetes and heart disease) than those who don’t drink diet soft drinks.
The link was found even after accounting for other dietary and lifestyle factors (such as physical activity).
In 2023, the WHO announced reports had found aspartame – the main sweetener used in diet soft drinks – was “possibly carcinogenic to humans” (carcinogenic means cancer-causing).
Importantly though, the report noted there is not enough current scientific evidence to be truly confident aspartame may increase the risk of cancer and emphasised it’s safe to consume occasionally.
Will diet soft drinks help manage weight?
Despite the word “diet” in the name, diet soft drinks are not strongly linked with weight management.
In 2022, the WHO conducted a systematic review (where researchers look at all available evidence on a topic) on whether the use of artificial sweeteners is beneficial for weight management.
Overall, the randomised controlled trials they looked at suggested slightly more weight loss in people who used artificial sweeteners.
But the observational studies (where no intervention occurs and participants are monitored over time) found people who consume high amounts of artificial sweeteners tended to have an increased risk of higher body mass index and a 76% increased likelihood of having obesity.
In other words, artificial sweeteners may not directly help manage weight over the long term. This resulted in the WHO advising artificial sweeteners should not be used to manage weight.
Studies in animals have suggested consuming high levels of artificial sweeteners can signal to the brain it is being starved of fuel, which can lead to more eating. However, the evidence for this happening in humans is still unproven.
You can’t go wrong with water. hurricanehank/Shutterstock What about inflammation and dental issues?
There is some early evidence artificial sweeteners may irritate the lining of the digestive system, causing inflammation and increasing the likelihood of diarrhoea, constipation, bloating and other symptoms often associated with irritable bowel syndrome. However, this study noted more research is needed.
High amounts of diet soft drinks have also been linked with liver disease, which is based on inflammation.
The consumption of diet soft drinks is also associated with dental erosion.
Many soft drinks contain phosphoric and citric acid, which can damage your tooth enamel and contribute to dental erosion.
Moderation is key
As with many aspects of nutrition, moderation is key with diet soft drinks.
Drinking diet soft drinks occasionally is unlikely to harm your health, but frequent or excessive intake may increase health risks in the longer term.
Plain water, infused water, sparkling water, herbal teas or milks remain the best options for hydration.
Lauren Ball, Professor of Community Health and Wellbeing, The University of Queensland and Emily Burch, Accredited Practising Dietitian and Lecturer, Southern Cross University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

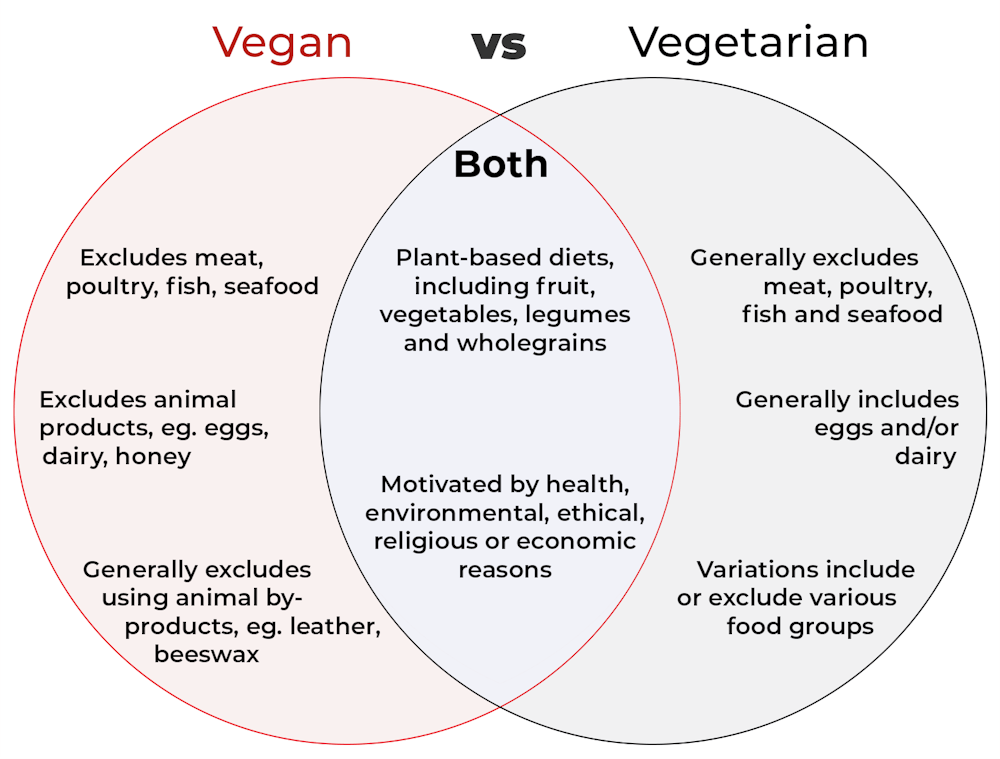
What’s the difference between vegan and vegetarian?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?
Creative Cat Studio/Shutterstock What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.
More than a diet: veganism can form part of someone’s identity. Shutterstock So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

The Seven-Day Sleep Prescription – by Dr. Aric Prather
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You probably already know about sleep hygiene. So, what does this book have to offer?
Dr. Aric Prather offers seven days’ worth of adjustments, practices to take up, from when you get up in the morning to when you lay your head down at night.
Some you’ll surely be familiar with, like avoiding blue light and social media at night.
Others, you might not be familiar with, like scheduling 15 minutes for worrying in the daytime. The rationale for this one is that when you find yourself inclined to worry at a time that will keep you awake, you’ll know that you can put off such thoughts to your scheduled “worrying time”. That they’ll be addressed then, and that you can thus sleep soundly meanwhile.
Where the book really comes into its own is in such things as discussing how to not just manage sleep debt, but how to actually use it in your favour.
Nor does Dr. Prather shy away from the truths of our world… That the world these days is not built for us to sleep well. That there are so many other priorities; to get our work done, to succeed and achieve, to pay bills, to support our kids and partners. That so many of these things make plenty of sense in the moment, but catch up with us eventually.
Bottom line: what this book aims to give is a genuinely sustainable approach to sleeping—controlling what we can, and working with what we can’t. If you’d like to have a better relationship with sleep, this book is an excellent choice.
Click here to check out the Seven-Day Sleep Prescription, and improve yours!
Share This Post






Related Posts
-

How Eating Grapes Protects Your Skin From UV Damage
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Oftentimes, when we write about the benefits of grapes, it’s about the water volume. Much like in our recent article about watermelon, the water volume is actually useful, in two main ways, so let’s quickly recap:
- One way is because enjoying food that contains water is generally more hydrating than just drinking water: Things Many People Forget When It Comes To Hydration
- Another way is that its volume (which is only possible because of its water content) increases satiety too: Some Surprising Truths About Hunger And Satiety
Of course, grapes are also well-known for their polyphenol content, or more specifically, for their resveratrol content, which has most popularly been talked about in the matter of the proposed health benefits of red wine.
We’ve written about that here: Can We Drink To Good Health? ← while there are polyphenols such as resveratrol that makes it through the process of turning into red wine that per se would boost heart health, there’s so little per glass that you may need 100–1000 glasses per day to get the dosage that provides benefits in mouse studies*.
*If you’re not a mouse, you might even need more than that!
To this end, many people prefer resveratrol supplementation ← link is to an example product on Amazon, but there are plenty more so feel free to shop around 😎
Now, it’s not the only reason for popular misunderstandings about alcohol and health, but for how that myth got started, see French biochemist Jessie Inchauspé’s explanation: Are You Making This Alcohol Mistake?
But what’s this about protecting one’s skin?
Save your skin
Researchers (Dr. John Pezzuto et al.) found that enjoying the equivalent of 3 portions of grapes per day for 2 weeks resulted in improved resistance to UV radiation in 30–50% of people.
How it works: it has to do with gene expression, and while the results were varied in terms of how each participant’s gene expression changed, gene expression was altered in all participants. Specifically these changes increased keratinization and cornification, which might sound bad, but in fact they are both processes that, in healthy moderation, help form the skin’s protective outer barrier (the “horny layer“, as it is also known, to the mirth of first-year students throughout the English-speaking world) against environmental damage.
As Dr. Pezzuto himself put it:
❝We are now certain that grapes act as a superfood and mediate a nutrigenomic response in humans.
We observed this with the largest organ of the body, the skin. The changes in gene expression indicated improvements in skin health. But beyond skin, it is nearly certain that grape consumption affects gene expression in other somatic tissues of the body, such as liver, muscle, kidney and even brain.
This helps us to understand how consumption of a whole food, in this case grapes, affects our overall health. It’s very exciting to be working in the post-genomics era where we can finally start to employ functional genomics and actually visualize complex matrices indicative of nutrigenomic responses.❞
You can read this paper in full, here: Inter- and Intraindividual Variation of Gene Expression in Human Skin Following Grape Consumption and/or Exposure to Ultraviolet Irradiation
And how this builds on from Dr. Pezzuto’s earlier work, here: Short-Term Grape Consumption Diminishes UV-Induced Skin Erythema
This is very similar to part of the mechanism by which almonds have similar skin benefits, including improving the skin’s resistance to UV radiation: Eat This Daily For No Wrinkles (& How It Works)
Want to learn more?
For more about protecting your skin from UV radiation, check out:
Beyond Sunscreen: The Ultimate Guide To Photoprotection For Your Skin
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Blood-Sugar Balancing Beetroot Cutlets
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
These beetroot cutlets are meaty and proteinous and fibrous and even have a healthy collection of fats, making these much better for your heart and blood than an animal-based equivalent.
You will need
- 1 can kidney beans, drained and rinsed (or 1 cup same, cooked, drained, and rinsed)
- ½ cup chopped roasted or steamed beetroot, blotted dry
- ½ cup chopped walnuts (if allergic, substitute with ¼ cup pumpkin seeds)
- ½ cup cooked (ideally: mixed) grains of your choice (if you need gluten-free, there are plenty of gluten-free grains and pseudocereals)
- ¼ cup finely chopped onion
- ¼ bulb garlic, minced or crushed
- 2 tbsp nutritional yeast
- 2 tbsp ground flaxseeds
- 2 tbsp ground chia seeds
- 2 tsp tomato purée
- 1 tsp black pepper
- ½ tsp white miso paste
- ½ tsp smoked paprika
- ½ tsp cayenne pepper
- ¼ tsp MSG or ½ tsp low-sodium salt
Method
(we suggest you read everything at least once before doing anything)
1) Combine the beetroot, beans, walnuts, grains, and onion in a food processor, and process until a coarse even mixture.
2) Add the remaining ingredients and process to mix thoroughly.
3) Transfer the mixture to a clean work surface and divide into six balls. If the structural integrity is not good (i.e. too soft), add a little more of any or all of these ingredients: chopped walnuts, ground flax, ground chia, nutritional yeast.
4) Press the balls firmly into cutlets, and refrigerate for at least 1 hour, but longer is even better if you have the time. Alternatively, if you’d like to freeze them for later use, then this is the point at which to do that.
5) Preheat the oven to 375℉ / 190℃.
6) Roast the cutlets on a baking tray lined with baking paper, for about 30 minutes, turning over carefully with a spatula halfway through. They should be firm when done; if they’re not, give them a little longer.
7) Serve hot, for example on a bed of greens and with a drizzle of aged balsamic vinegar.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Beetroot’s Many Benefits
- Our Top 5 Spices: How Much Is Enough For Benefits?
- What Omega-3 Fatty Acids Really Do For Us
- Three Daily Servings of Beans?
- If You’re Not Taking Chia, You’re Missing Out
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Bird Flu Is Bad for Poultry and Dairy Cows. It’s Not a Dire Threat for Most of Us — Yet.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Headlines are flying after the Department of Agriculture confirmed that the H5N1 bird flu virus has infected dairy cows around the country. Tests have detected the virus among cattle in nine states, mainly in Texas and New Mexico, and most recently in Colorado, said Nirav Shah, principal deputy director at the Centers for Disease Control and Prevention, at a May 1 event held by the Council on Foreign Relations.
A menagerie of other animals have been infected by H5N1, and at least one person in Texas. But what scientists fear most is if the virus were to spread efficiently from person to person. That hasn’t happened and might not. Shah said the CDC considers the H5N1 outbreak “a low risk to the general public at this time.”
Viruses evolve and outbreaks can shift quickly. “As with any major outbreak, this is moving at the speed of a bullet train,” Shah said. “What we’ll be talking about is a snapshot of that fast-moving train.” What he means is that what’s known about the H5N1 bird flu today will undoubtedly change.
With that in mind, KFF Health News explains what you need to know now.
Q: Who gets the bird flu?
Mainly birds. Over the past few years, however, the H5N1 bird flu virus has increasingly jumped from birds into mammals around the world. The growing list of more than 50 species includes seals, goats, skunks, cats, and wild bush dogs at a zoo in the United Kingdom. At least 24,000 sea lions died in outbreaks of H5N1 bird flu in South America last year.
What makes the current outbreak in cattle unusual is that it’s spreading rapidly from cow to cow, whereas the other cases — except for the sea lion infections — appear limited. Researchers know this because genetic sequences of the H5N1 viruses drawn from cattle this year were nearly identical to one another.
The cattle outbreak is also concerning because the country has been caught off guard. Researchers examining the virus’s genomes suggest it originally spilled over from birds into cows late last year in Texas, and has since spread among many more cows than have been tested. “Our analyses show this has been circulating in cows for four months or so, under our noses,” said Michael Worobey, an evolutionary biologist at the University of Arizona in Tucson.
Q: Is this the start of the next pandemic?
Not yet. But it’s a thought worth considering because a bird flu pandemic would be a nightmare. More than half of people infected by older strains of H5N1 bird flu viruses from 2003 to 2016 died. Even if death rates turn out to be less severe for the H5N1 strain currently circulating in cattle, repercussions could involve loads of sick people and hospitals too overwhelmed to handle other medical emergencies.
Although at least one person has been infected with H5N1 this year, the virus can’t lead to a pandemic in its current state. To achieve that horrible status, a pathogen needs to sicken many people on multiple continents. And to do that, the H5N1 virus would need to infect a ton of people. That won’t happen through occasional spillovers of the virus from farm animals into people. Rather, the virus must acquire mutations for it to spread from person to person, like the seasonal flu, as a respiratory infection transmitted largely through the air as people cough, sneeze, and breathe. As we learned in the depths of covid-19, airborne viruses are hard to stop.
That hasn’t happened yet. However, H5N1 viruses now have plenty of chances to evolve as they replicate within thousands of cows. Like all viruses, they mutate as they replicate, and mutations that improve the virus’s survival are passed to the next generation. And because cows are mammals, the viruses could be getting better at thriving within cells that are closer to ours than birds’.
The evolution of a pandemic-ready bird flu virus could be aided by a sort of superpower possessed by many viruses. Namely, they sometimes swap their genes with other strains in a process called reassortment. In a study published in 2009, Worobey and other researchers traced the origin of the H1N1 “swine flu” pandemic to events in which different viruses causing the swine flu, bird flu, and human flu mixed and matched their genes within pigs that they were simultaneously infecting. Pigs need not be involved this time around, Worobey warned.
Q: Will a pandemic start if a person drinks virus-contaminated milk?
Not yet. Cow’s milk, as well as powdered milk and infant formula, sold in stores is considered safe because the law requires all milk sold commercially to be pasteurized. That process of heating milk at high temperatures kills bacteria, viruses, and other teeny organisms. Tests have identified fragments of H5N1 viruses in milk from grocery stores but confirm that the virus bits are dead and, therefore, harmless.
Unpasteurized “raw” milk, however, has been shown to contain living H5N1 viruses, which is why the FDA and other health authorities strongly advise people not to drink it. Doing so could cause a person to become seriously ill or worse. But even then, a pandemic is unlikely to be sparked because the virus — in its current form — does not spread efficiently from person to person, as the seasonal flu does.
Q: What should be done?
A lot! Because of a lack of surveillance, the U.S. Department of Agriculture and other agencies have allowed the H5N1 bird flu to spread under the radar in cattle. To get a handle on the situation, the USDA recently ordered all lactating dairy cattle to be tested before farmers move them to other states, and the outcomes of the tests to be reported.
But just as restricting covid tests to international travelers in early 2020 allowed the coronavirus to spread undetected, testing only cows that move across state lines would miss plenty of cases.
Such limited testing won’t reveal how the virus is spreading among cattle — information desperately needed so farmers can stop it. A leading hypothesis is that viruses are being transferred from one cow to the next through the machines used to milk them.
To boost testing, Fred Gingrich, executive director of a nonprofit organization for farm veterinarians, the American Association of Bovine Practitioners, said the government should offer funds to cattle farmers who report cases so that they have an incentive to test. Barring that, he said, reporting just adds reputational damage atop financial loss.
“These outbreaks have a significant economic impact,” Gingrich said. “Farmers lose about 20% of their milk production in an outbreak because animals quit eating, produce less milk, and some of that milk is abnormal and then can’t be sold.”
The government has made the H5N1 tests free for farmers, Gingrich added, but they haven’t budgeted money for veterinarians who must sample the cows, transport samples, and file paperwork. “Tests are the least expensive part,” he said.
If testing on farms remains elusive, evolutionary virologists can still learn a lot by analyzing genomic sequences from H5N1 viruses sampled from cattle. The differences between sequences tell a story about where and when the current outbreak began, the path it travels, and whether the viruses are acquiring mutations that pose a threat to people. Yet this vital research has been hampered by the USDA’s slow and incomplete posting of genetic data, Worobey said.
The government should also help poultry farmers prevent H5N1 outbreaks since those kill many birds and pose a constant threat of spillover, said Maurice Pitesky, an avian disease specialist at the University of California-Davis.
Waterfowl like ducks and geese are the usual sources of outbreaks on poultry farms, and researchers can detect their proximity using remote sensing and other technologies. By zeroing in on zones of potential spillover, farmers can target their attention. That can mean routine surveillance to detect early signs of infections in poultry, using water cannons to shoo away migrating flocks, relocating farm animals, or temporarily ushering them into barns. “We should be spending on prevention,” Pitesky said.
Q: OK it’s not a pandemic, but what could happen to people who get this year’s H5N1 bird flu?
No one really knows. Only one person in Texas has been diagnosed with the disease this year, in April. This person worked closely with dairy cows, and had a mild case with an eye infection. The CDC found out about them because of its surveillance process. Clinics are supposed to alert state health departments when they diagnose farmworkers with the flu, using tests that detect influenza viruses, broadly. State health departments then confirm the test, and if it’s positive, they send a person’s sample to a CDC laboratory, where it is checked for the H5N1 virus, specifically. “Thus far we have received 23,” Shah said. “All but one of those was negative.”
State health department officials are also monitoring around 150 people, he said, who have spent time around cattle. They’re checking in with these farmworkers via phone calls, text messages, or in-person visits to see if they develop symptoms. And if that happens, they’ll be tested.
Another way to assess farmworkers would be to check their blood for antibodies against the H5N1 bird flu virus; a positive result would indicate they might have been unknowingly infected. But Shah said health officials are not yet doing this work.
“The fact that we’re four months in and haven’t done this isn’t a good sign,” Worobey said. “I’m not super worried about a pandemic at the moment, but we should start acting like we don’t want it to happen.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: