Beyond Sunscreen: The Ultimate Guide To Photoprotection For Your Skin
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Andrea Suarez, dermatologist, gives us a lot more tools:
Under the sun
Everybody knows to wear sunscreen.
However, Dr. Suarez explains that sunscreen alone isn’t enough, so what more can we do?
First, a quick reminder on different kinds of solar radiation:
- UVA makes up over 95% of UV from the sun, penetrates deeply, accelerates aging and pigmentation, and passes through window glass
- UVB causes sunburn and direct DNA damage, albeit there’s a lot less of it and it’s more easily blocked, even just by windows
Avoiding the sun is of course a fine strategy, and timing counts for UVB but not UVA, because UVB peaks between 10:00 a.m. and 2 p.m. while UVA is constant all day and even on cloudy days, and exposure increases with altitude and near the equator.
Note, however:
- Shade is something of an illusion, and by this we mean: shade can still expose you to about 50% of UVA due to scattering and reflection, meaning umbrellas and trees don’t provide complete protection.
- Clothing, however, can help: in particular, tightly woven, thicker, darker fabrics and materials like polyester or wool provide good protection, while coverage and fabric condition matter more than whether clothing is labeled UPF.
Some quick extra notes on that:
- What’s going on with those UPF ratings: UPF 50 fabric allows only 1/50th of UV through, but regular clothing can perform similarly if dense, dry, and not worn out.
- Wet and worn fabrics: wet, stretched, or aged fabrics lose protective ability, while washing can sometimes improve protection by tightening the weave.
- About hats: wide-brimmed hats offer significantly more protection for your face, ears, and neck compared to baseball caps, with brim width directly affecting coverage, for obvious reasons
As for your eyes:
- Yes, sunglasses help: UV exposure increases risks like cataracts and ocular damage, so look for sunglasses labeled UV 400 or 100% UV protection (price is no indicator of quality, so check the labels).
- The design counts too: wraparound styles reduce side exposure, and of course bigger is better than smaller.
- What we said about windows matters here too: standard windows block UVB but allow UVA through, meaning indoor and car exposure still contributes to cumulative skin damage.
- A special case, however, is car windows: windshields block most UV, but side and rear windows often allow UVA unless treated with UV-blocking films.
Some other things to consider:
- Topical antioxidants: ingredients like vitamin C, vitamin E, ferulic acid, green tea, and niacinamide help neutralize reactive oxygen species generated by UV exposure, and thus also help reduce the harm.
- DNA repair enzymes: compounds like photolyase and T4 endonuclease have been shown to reduce UV-induced DNA damage and precancerous lesions, though they’re not so widely available as the other measures discussed.
- Oral supplements: some supplements can help, for example Polypodium leucotomos extract has evidence for reducing UV sensitivity and inflammation, especially in photosensitive conditions.
- Dietary carotenoids: nutrients like beta-carotene and lycopene from whole foods may support skin resilience, though supplements are less clearly beneficial in this case.
Finally, remember that consistency generally matters most: daily is is much more important than occasional perfect use, because cumulative exposure is what really drives skin damage and cancer risk.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Ageless Aging – by Maddy Dychtwald

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Maddy Dychtwald, herself 73, has spent her career working in the field of aging. She’s not a gerontologist or even a doctor, but she’s nevertheless been up-to-the-ears in the industry for decades, mostly as an organizer, strategist, facilitator, and so forth. As such, she’s had her finger on the pulse of the healthy longevity movement for a long time.
This book was written to address a problem, and the problem is: lifespan is increasing (especially for women), but healthspan has not been keeping up the pace.
In other words: people (especially women) are living longer, but often with more health problems along the way than before.
And mostly, it’s for lack of information (or sometimes: too much competing incorrect information).
Fortunately, information is something that a woman in Dychtwald’s position has an abundance of, because she has researchers and academics in many fields on speed-dial and happy to answer her questions (we get a lot of input from such experts throughout the book—which is why this book is so science-based, despite the author not being a scientist).
The book answers a lot of important questions beyond the obvious “what diet/exercise/sleep/supplements/etc are best for healthy aging” (spoiler: it’s quite consistent with the things we recommend here, because guess what, science is science), questions like how best to prepare for this that or the other, how to get a head start on preventative healthcare for some things, how to avoid being a burden to our families (one can argue that families are supposed to look after each other, but still, it’s a legitimate worry for many, and understandably so), and even how to balance the sometimes conflicting worlds of health and finances.
Unlike many authors, she also talks about the different kinds of aging, and tackles each of them separately and together. We love to see it!
Bottom line: this book is a very good one-stop-shop for all things healthy aging. It’s aimed squarely at women, but most advice goes for men the same too, aside from the section on hormones and such.
Click here to check out Ageless Aging, and plan your future!
Share This Post
-

Don’t Do *This* If You’re Over 50 (And Want Better Sleep)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Michael Breus, sleep specialist, explains:
Don’t make these mistakes
Dr. Breus recommends avoiding…
- Misusing magnesium: magnesium is a helpful sleep aid but must be carefully monitored. Recommended doses are 250mg for women and 300–350 mg for men, with slight adjustments for hot climates or active lifestyles. Overdosing can cause stomach issues, diarrhea, and dehydration, disrupting sleep. He recommends starting with magnesium glycinate for fewer stomach issues, and later mix with magnesium citrate. Always check supplements to avoid excessive magnesium intake.
- Misusing melatonin: melatonin production declines after age 55–60, making low-dose supplementation (0.5–1 mg) beneficial. He recommends, however, avoiding high doses (3–10mg), and he recommends to take it 90 minutes before bedtime. Melatonin interacts with some medications (including some meds for blood pressure or depression), so consult a pharmacist before use to avoid risks like serotonin syndrome.
- Going to bed too early: going to bed too early disrupts circadian rhythms and reduces sleep drive, causing earlier waking. Now, being an “early bird” is a generally healthy thing, but if you’re already getting up at 5am, say, you probably want your schedule to not continue to creep further forwards until you become nocturnal. Set a consistent wake-up time and count 7.5 hours backward (plus a set time to fall asleep, e.g. 20 minutes, but you’ll know what it is for you) to determine bedtime.
- Excessive caffeine consumption: from the heading, it may seem like a no-brainer, but older adults metabolize caffeine 33% slower on average, prolonging its effects. Dr. Breus recommends to reduce intake with “caffeine fading,” switching to half-caffeinated coffee for a while and then considering transitioning to decaf. He also suggests enjoying increasingly lower-caffeine teas, like black tea in the morning, matcha in the afternoon, and herbal tea at night to reduce caffeine’s impact on sleep.
- Falling foul of serotonin: avoid taking 5-HTP supplements with SSRI antidepressants like Prozac or Zoloft due to the risk of serotonin syndrome.
- Consider checking for physical problems: if you regularly wake up tired and/or groggy (despite having ostensibly had enough sleep, and there not being a pharmaceutical explanation for your grogginess), consider screening for sleep apnea. Home sleep tests are a convenient way to identify and treat this common but often undiagnosed condition.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
How to Fall Asleep Faster: CBT-Insomnia Treatment
Take care!
Share This Post
-

Meningitis Outbreak
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Don’t Let Your Guard Down
In the US, meningitis is currently enjoying a 10-year high, with its highest levels of infection since 2014.
This is a big deal, given the 10–15% fatality rate of meningitis, even with appropriate medical treatment.
But of course, not everyone gets appropriate medical treatment, especially because symptoms can become life-threatening in a matter of hours.
Most recent stats gave an 18% fatality rate for the cases with known outcomes in the last year:
CDC Emergency | Increase in Invasive Serogroup Y Meningococcal Disease in the United States
The quick facts:
❝Meningococcal disease most often presents as meningitis, with symptoms that may include fever, headache, stiff neck, nausea, vomiting, photophobia, or altered mental status.
[It can also present] as meningococcal bloodstream infection, with symptoms that may include fever and chills, fatigue, vomiting, cold hands and feet, severe aches and pains, rapid breathing, diarrhea, or, in later stages, a dark purple rash.
While initial symptoms of meningococcal disease can at first be non-specific, they worsen rapidly, and the disease can become life-threatening within hours. Immediate antibiotic treatment for meningococcal disease is critical.
Survivors may experience long-term effects such as deafness or amputations of the extremities.❞
~ Ibid.
The good news (but still don’t let your guard down)
Meningococcal bacteria are, happily, not spread as easily as cold and flu viruses.
The greatest risks come from:
- Close and enduring proximity (e.g. living together)
- Oral, or close-to-oral, contact (e.g. kissing, or coughing nearby)
Read more:
CDC | Meningococcal Disease: Causes & How It Spreads
Is there a vaccine?
There is, but it’s usually only offered to those most at risk, which is usually:
- Children
- Immunocompromised people, especially if HIV+
- People taking certain medications (e.g. Solaris or Ultomiris)
Read more:
CDC | Meningococcal Vaccine Recommendations
Will taking immune-boosting supplements help?
Honestly, probably not, but they won’t harm either. The most important thing is: don’t rely on them—too many people pop a vitamin C supplement and then assume they are immune to everything, and it doesn’t work like that.
On a tangential note, for more general immune health, you might also want to check out:
Beyond Supplements: The Real Immune-Boosters!
The short version:
If you or someone you know experiences the above-mentioned symptoms, even if it does not seem too bad, get thee/them to a doctor, and quickly, because the (very short) clock may be ticking already.
Better safe than sorry.
Share This Post

Related Posts
-

Mammography AI Can Cost Patients Extra. Is It Worth It?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As I checked in at a Manhattan radiology clinic for my annual mammogram in November, the front desk staffer reviewing my paperwork asked an unexpected question: Would I like to spend $40 for an artificial intelligence analysis of my mammogram? It’s not covered by insurance, she added.
I had no idea how to evaluate that offer. Feeling upsold, I said no. But it got me thinking: Is this something I should add to my regular screening routine? Is my regular mammogram not accurate enough? If this AI analysis is so great, why doesn’t insurance cover it?
I’m not the only person posing such questions. The mother of a colleague had a similar experience when she went for a mammogram recently at a suburban Baltimore clinic. She was given a pink pamphlet that said: “You Deserve More. More Accuracy. More Confidence. More power with artificial intelligence behind your mammogram.” The price tag was the same: $40. She also declined.
In recent years, AI software that helps radiologists detect problems or diagnose cancer using mammography has been moving into clinical use. The software can store and evaluate large datasets of images and identify patterns and abnormalities that human radiologists might miss. It typically highlights potential problem areas in an image and assesses any likely malignancies. This extra review has enormous potential to improve the detection of suspicious breast masses and lead to earlier diagnoses of breast cancer.
While studies showing better detection rates are extremely encouraging, some radiologists say, more research and evaluation are needed before drawing conclusions about the value of the routine use of these tools in regular clinical practice.
“I see the promise and I hope it will help us,” said Etta Pisano, a radiologist who is chief research officer at the American College of Radiology, a professional group for radiologists. However, “it really is ambiguous at this point whether it will benefit an individual woman,” she said. “We do need more information.”
The radiology clinics that my colleague’s mother and I visited are both part of RadNet, a company with a network of more than 350 imaging centers around the country. RadNet introduced its AI product for mammography in New York and New Jersey last February and has since rolled it out in several other states, according to Gregory Sorensen, the company’s chief science officer.
Sorensen pointed to research the company conducted with 18 radiologists, some of whom were specialists in breast mammography and some of whom were generalists who spent less than 75% of their time reading mammograms. The doctors were asked to find the cancers in 240 images, with and without AI. Every doctor’s performance improved using AI, Sorensen said.
Among all radiologists, “not every doctor is equally good,” Sorensen said. With RadNet’s AI tool, “it’s as if all patients get the benefit of our very top performer.”
But is the tech analysis worth the extra cost to patients? There’s no easy answer.
“Some people are always going to be more anxious about their mammograms, and using AI may give them more reassurance,” said Laura Heacock, a breast imaging specialist at NYU Langone Health’s Perlmutter Cancer Center in New York. The health system has developed AI models and is testing the technology with mammograms but doesn’t yet offer it to patients, she said.
Still, Heacock said, women shouldn’t worry that they need to get an additional AI analysis if it’s offered.
“At the end of the day, you still have an expert breast imager interpreting your mammogram, and that is the standard of care,” she said.
About 1 in 8 women will be diagnosed with breast cancer during their lifetime, and regular screening mammograms are recommended to help identify cancerous tumors early. But mammograms are hardly foolproof: They miss about 20% of breast cancers, according to the National Cancer Institute.
The FDA has authorized roughly two dozen AI products to help detect and diagnose cancer from mammograms. However, there are currently no billing codes radiologists can use to charge health plans for the use of AI to interpret mammograms. Typically, the federal Centers for Medicare & Medicaid Services would introduce new billing codes and private health plans would follow their lead for payment. But that hasn’t happened in this field yet and it’s unclear when or if it will.
CMS didn’t respond to requests for comment.
Thirty-five percent of women who visit a RadNet facility for mammograms pay for the additional AI review, Sorensen said.
Radiology practices don’t handle payment for AI mammography all in the same way.
The practices affiliated with Boston-based Massachusetts General Hospital don’t charge patients for the AI analysis, said Constance Lehman, a professor of radiology at Harvard Medical School who is co-director of the Breast Imaging Research Center at Mass General.
Asking patients to pay “isn’t a model that will support equity,” Lehman said, since only patients who can afford the extra charge will get the enhanced analysis. She said she believes many radiologists would never agree to post a sign listing a charge for AI analysis because it would be off-putting to low-income patients.
Sorensen said RadNet’s goal is to stop charging patients once health plans realize the value of the screening and start paying for it.
Some large trials are underway in the United States, though much of the published research on AI and mammography to date has been done in Europe. There, the standard practice is for two radiologists to read a mammogram, whereas in the States only one radiologist typically evaluates a screening test.
Interim results from the highly regarded MASAI randomized controlled trial of 80,000 women in Sweden found that cancer detection rates were 20% higher in women whose mammograms were read by a radiologist using AI compared with women whose mammograms were read by two radiologists without any AI intervention, which is the standard of care there.
“The MASAI trial was great, but will that generalize to the U.S.? We can’t say,” Lehman said.
In addition, there is a need for “more diverse training and testing sets for AI algorithm development and refinement” across different races and ethnicities, said Christoph Lee, director of the Northwest Screening and Cancer Outcomes Research Enterprise at the University of Washington School of Medicine.
The long shadow of an earlier and largely unsuccessful type of computer-assisted mammography hangs over the adoption of newer AI tools. In the late 1980s and early 1990s, “computer-assisted detection” software promised to improve breast cancer detection. Then the studies started coming in, and the results were often far from encouraging. Using CAD at best provided no benefit, and at worst reduced the accuracy of radiologists’ interpretations, resulting in higher rates of recalls and biopsies.
“CAD was not that sophisticated,” said Robert Smith, senior vice president of early cancer detection science at the American Cancer Society. Artificial intelligence tools today are a whole different ballgame, he said. “You can train the algorithm to pick up things, or it learns on its own.”
Smith said he found it “troubling” that radiologists would charge for the AI analysis.
“There are too many women who can’t afford any out-of-pocket cost” for a mammogram, Smith said. “If we’re not going to increase the number of radiologists we use for mammograms, then these new AI tools are going to be very useful, and I don’t think we can defend charging women extra for them.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Alzheimer’s Symptoms That Start Outside Your Brain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
…and other items from this week’s health news:
Body & brain
Researchers (Dr. Akhmetzada Kargazhanov et al.) have found that some symptoms of Alzheimer’s disease—especially movement problems—begin outside the brain, in the peripheral nervous system.
In few words: changes in balance, gait, and coordination can appear years before memory loss.
Further, the team found that mutations linked to Alzheimer’s disrupted the neuromuscular junction even without any involvement from the brain or spinal cord, when impaired signaling between nerves and muscles reduces contraction reliability and increases fatigue, directly affecting movement.
This is important in practical terms, because if symptoms start outside the brain, treatments that only target the brain can easily miss a significant part of the disease!
Read in full: Study suggests some Alzheimer’s symptoms may begin outside the brain
Related: How To Reduce Your Alzheimer’s Risk
Do we need GLP-1 receptor agonists at all?
For weight loss, that is, not for diabetes control (which latter thing is what they were invented for, before the world collectively forgot about treating a potentially deadly disorder, in order to focus on a more widely marketable aesthetics angle instead).
Researchers (Dr. Fa Zhang et al.) examined this by investigating a different pathway using GIP and glucagon itself, instead of targeting GLP-1.
What she and her team found is that not only did this work even in animals without GLP-1 receptors, but also, combining GIP and glucagon appears to enhance weight loss more than either alone, likely by both reducing appetite and increasing energy expenditure.
And, importantly, high doses of the new drug were tolerated much better than existing GLP-1-based treatments, which would make a big different to many people when GLP-1 receptor agonist side effects can be very off-putting, so say the least.
Read in full: Weight loss research questions need for GLP-1 drugs
Related: Most People Who Start GLP-1 RAs Quit Them Within A Year (Here’s Why)
Another Promethean endeavor
We’ve written before about the liver’s amazing regenerative abilities, but sometimes, the liver does defy its name (i.e., it dies, and needs replacing before it stops completely).
One of the problems is that patients with end-stage liver disease often need transplants, but shortages mean about 20% die while waiting.
Thus, lab-grown livers are of course a promising avenue of research. To this end, researchers (Dr. Amy Stoddard et al.) developed a method called BOOST whereby instead of growing a full liver in the lab, scientists implant a small engineered “seed” of liver tissue that can expand inside the body.
In other words, they can now grow liver tissue directly inside the body after implantation.
As for how it works: the method rewires gene expression in liver cells (hepatocytes) and support cells so growth can be turned on with a trigger drug and stopped when needed.
Read in full: Growing liver tissue directly in the body could ease donor organ shortage
Related: How To Unfatty A Fatty Liver
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Should You Go Light Or Heavy On Carbs?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Carb-Strong or Carb-Wrong?

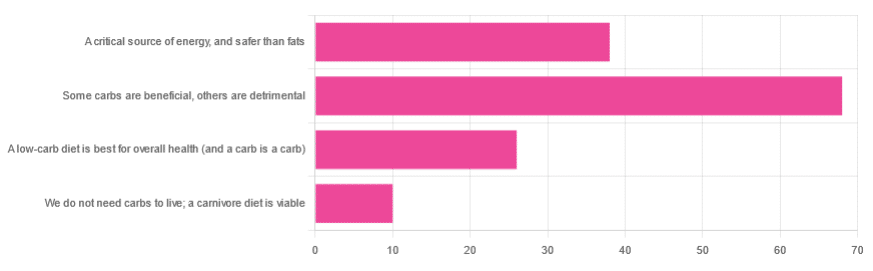
We asked you for your health-related view of carbs, and got the above-depicted, below-described, set of responses
- About 48% said “Some carbs are beneficial; others are detrimental”
- About 27% said “Carbs are a critical source of energy, and safer than fats”
- About 18% said “A low-carb diet is best for overall health (and a carb is a carb)”
- About 7% said “We do not need carbs to live; a carnivore diet is viable”
But what does the science say?
Carbs are a critical source of energy, and safer than fats: True or False?
True and False, respectively! That is: they are a critical source of energy, and carbs and fats both have an important place in our diet.
❝Diets that focus too heavily on a single macronutrient, whether extreme protein, carbohydrate, or fat intake, may adversely impact health.❞
Source: Low carb or high carb? Everything in moderation … until further notice
(the aforementioned lead author Dr. de Souza, by the way, served as an external advisor to the World Health Organization’s Nutrition Guidelines Advisory Committee)
Some carbs are beneficial; others are detrimental: True or False?
True! Glycemic index is important here. There’s a big difference between eating a raw carrot and drinking high-fructose corn syrup:
Which Sugars Are Healthier, And Which Are Just The Same?
While some say grains and/or starchy vegetables are bad, best current science recommends:
- Eat some whole grains regularly, but they should not be the main bulk of your meal (non-wheat grains are generally better)
- Starchy vegetables are not a critical food group, but in moderation they are fine.
To this end, the Mediterranean Diet is the current gold standard of healthful eating, per general scientific consensus:
A low-carb diet is best for overall health (and a carb is a carb): True or False?
True-ish and False, respectively. We covered the “a carb is a carb” falsehood earlier, so we’ll look at “a low-carb diet is best”.
Simply put: it can be. One of the biggest problems facing the low-carb diet though is that adherence tends to be poor—that is to say, people crave their carby comfort foods and eat more carbs again. As for the efficacy of a low-carb diet in the context of goals such as weight loss and glycemic control, the evidence is mixed:
❝There is probably little to no difference in weight reduction and changes in cardiovascular risk factors up to two years’ follow-up, when overweight and obese participants without and with T2DM are randomised to either low-carbohydrate or balanced-carbohydrate weight-reducing diets❞
Source: Low-carbohydrate versus balanced-carbohydrate diets for reducing weight and cardiovascular risk
❝On the basis of moderate to low certainty evidence, patients adhering to an LCD for six months may experience remission of diabetes without adverse consequences.
Limitations include continued debate around what constitutes remission of diabetes, as well as the efficacy, safety, and dietary satisfaction of longer term LCDs❞
~ Dr. Joshua Goldenberg et al.
Source: Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission
❝There should be no “one-size-fits-all” eating pattern for different patient´s profiles with diabetes.
It is clinically complex to suggest an ideal percentage of calories from carbohydrates, protein and lipids recommended for all patients with diabetes.❞
Source: Current Evidence Regarding Low-carb Diets for The Metabolic Control of Type-2 Diabetes
We do not need carbs to live; a carnivore diet is viable: True or False?
False. For a simple explanation:
The Carnivore Diet: Can You Have Too Much Meat?
There isn’t a lot of science studying the effects of consuming no plant products, largely because such a study, if anything other than observational population studies, would be unethical. Observational population studies, meanwhile, are not practical because there are so few people who try this, and those who do, do not persist after their first few hospitalizations.
Putting aside the “Carnivore Diet” as a dangerous unscientific fad, if you are inclined to meat-eating, there is some merit to the Paleo Diet, at least for short-term weight loss even if not necessarily long-term health:
What’s The Real Deal With The Paleo Diet?
For longer-term health, we refer you back up to the aforementioned Mediterranean Diet.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: