What’s the difference between vegan and vegetarian?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
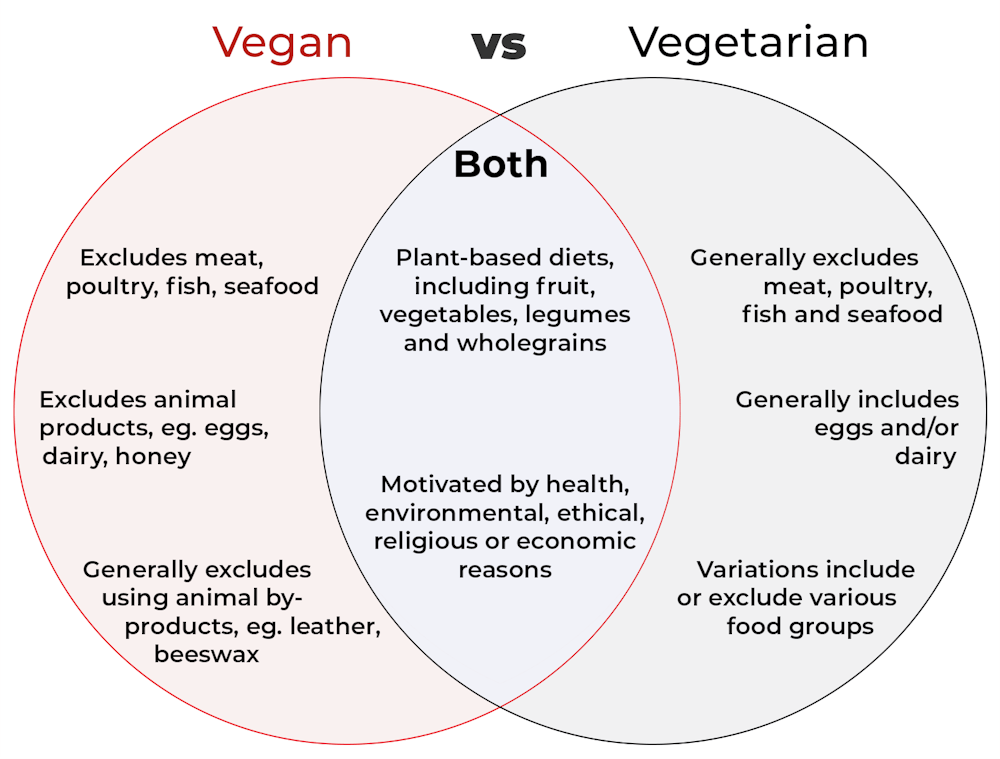
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?

What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.

So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Get Better Sleep: Beyond The Basics

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First though, for the sake of being methodical, let’s quickly note the basics:
- Aim for 7–9 hours per night
- Set a regular bedtime and (equally important!) regular getting-up time
- Have a 2-hour wind-down period before bed, to decompress from any stresses of the day
- Minimal device/screen usage before bed
- Abstain from stimulants for as long before bed as reasonably possible (caffeine elimination halflife is 4–8 hours depending on your genes, call it 6 hours average to eliminate half (not the whole lot), and you’ll see it’s probably best to put a cap on it earlier rather than later).
- Abstain from alcohol, ideally entirely, but allow at least 1hr/unit before bed. So for example, 1hr for a 1oz single shot of spirits, or 2–3 hours for a glass of wine (depending on size), or 3–4 hours for a martini (depending on recipe). Not that that is not the elimination time, nor even the elimination halflife of alcohol, it’s just a “give your body a chance at least” calculation. If you like to have a drink to relax before bed, then well, only you can decide what you like more: that or actually getting restorative sleep.
- Consider a warm bath/shower before bed, if that suits your schedule.
- Wash and change your bedsheets more often than seems necessary. Or if that’s too onerous, at least change the pillowcases more often, which makes quite a difference already.
- Lower the temperature of your bedroom shortly before bedtime; this will help cue the body to produce melatonin
- Make your bedroom as dark as reasonably possible. Invest in blackout blinds/curtains, and remove any pesky electronics, or at least cover their little LEDs if it’s something that reasonably needs to remain on.
Ok, now, onwards…
Those 7–9 hours? Yes, it goes for you too.
A lot of people mistake getting 6 hours sleep per night for only needing 6 hours sleep per night. Sure, you may still be alive after regularly getting 6 hours, but (unless you have a rare mutation of the ADRB1 gene) it will be causing harm, and yes, that includes later in life; we don’t stop needing so much sleep, even stop getting it:
Why You Probably Need More Sleep
With this in mind, it becomes important to…
Prioritize your sleep—which means planning for it!
When does your bedtime routine start? According to sleep scientist Dr. Lisa Matricciani, it starts before breakfast. This is because the things we do earlier in the day can greatly affect the amount (and quality) of sleep we get later. For example, a morning moderate-to-intense exercise session greatly improves sleep at night:
Planning Ahead For Better Sleep
As for quality, that is as important as quantity, and it’s not just about “soundness” of sleep:
The 6 Dimensions Of Sleep (And Why They Matter)
“What gets measured, gets done” goes for sleep too
Sleep-deprived people usually underestimate how sleep-deprived they are. This is for the same reason as why drunk people usually underestimate how drunk they are—to put it in words that go for both situations: a cognitively impaired person lacks the cognitive function to realize how cognitively impaired they are.
Here’s the science on that, by the way:
How Sleep-Deprived Are You, Really?
For that reason, we recommend using sleep-tracking software (there are many apps for that) on your phone or, ideally, a wearable device (such as a smartwatch or similar).
A benefit of doing so is that we don’t think “well, I slept from 10pm to 6am, so that’s 8 hours”, if our device tells us we slept between 10:43pm and 5:56 am with 74% sleep efficiency because we woke up many times.
As an aside, sleep efficiency should be about 85%, by the way. Why not 100%, you ask? It’s because if your body is truly out like a light for the entire night, something is wrong (either you were very sleep-deprived, or you have been drugged, that kind of thing). See also:
An unbroken night’s sleep is a myth. Here’s what good sleep looks like.
So waking up during the night is normal, and nothing to worry about per se. If you do find trouble getting back to sleep, though:
How to Fall Back Asleep After Waking Up in the Middle of the Night
Be careful about how you try to supplement sleep
This goes both for taking substances of various kinds, and napping. Some sleep aids can help, but many are harmful and/or do not really work as such; here’s a rundown of examples of those:
Safe Effective Sleep Aids For Seniors?
And when it comes to napping, timing is everything:
How To Nap Like A Pro (No More “Sleep Hangovers”!)
Want to know a lot more?
This is the book on sleep:
Why We Sleep – by Dr. Matthew Walker
Enjoy!
Share This Post
-

Accessing the Healing Power of the Vagus Nerve – by Dr. Stanley Rosenberg
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are a lot of books out there about using vagus nerve stimulation to improve various aspects of one’s mental and physical health, but often they boil down to “massage this and relax”.
In this case, the book makes heavy use of the ideas described in a book we’ve reviewed previously: The Polyvagal Theory – by Dr. Stephen Porges
That book is considered the book on this topic, so… Why read this one when that one is right there?
The main reason you might want to read this book rather than that one, is that that one’s a very dense and technical 386 pages, whereas this one’s at the heavy-end-of-pop-science, and 296 pages. This distinction makes it a lot easier for the layperson to read—the other, while published for the public, was very clearly written for academics.
A second reason you might want to read this book rather than that one is that this one is written with practical intent; while Dr. Porges’ book was focused on “how this works”, Dr. Rosenberg’s book is focused on “how to use this to achieve specific, practical ends”.
As to what those are: the list of things the author claims these techniques will cure is too long to go into each item here, but we will say that it doesn’t look to us like the evidence is here for all of these claims. In many cases the author relies on anecdotal case studies, and in equally many (often the same) cases, it might be fairer to say that the techniques support the body’s natural processes rather than that it, say, will treat a hernia or fix bipolar disorder. Maybe one day evidence will be found to demonstrate that these exercises can indeed do those things, but it’s not today.
Bottom line: in this reviewer’s opinion, the author makes some overly bold claims about the results one can expect, but that doesn’t take away from the fact that this is still an excellent practical guide to vagus nerve stimulation, and in many ways a much more accessible introduction to polyvagal theory than Dr. Porges’ magnum opus, while still being head and shoulders above most books about the vagus nerve.
Share This Post
-

Taking prescription opioids for too long can be harmful. Here’s how to cut back and stop
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Opioids, such as oxycodone, morphine, codeine, tramadol and fentanyl, are commonly prescribed to manage pain. You might be given a prescription when experiencing pain, or after surgery or an injury.
But while opioids may relieve pain in the short term, they provide little to no lasting improvement in pain or function beyond a few weeks for people whose pain isn’t caused by cancer.
Opioids can also cause side effects such as nausea, constipation and drowsiness, as well as serious risks such as dependence and overdose.
Over the past decade, Australia has introduced initiatives to reduce opioid use and related harm. This includes new guidelines that recommend reducing the dose or stopping opioids when the risks of continuing outweigh the benefits.
Many people can reduce or stop opioids without their pain worsening. Some people even experience less pain. However, for some people, reducing or stopping opioids can result in worse pain, mental health crises and even suicide.
Our new research, published today in the New England Journal of Medicine, explains how to safely reduce and stop taking prescription opioids.

Maskot/Getty Images How do you know when it’s time to stop? Then what?
Determining whether it is appropriate to reduce or stop opioids depends on several factors unique to each person. These include:
- why opioids were prescribed
- how long they’ve been used
- what other treatments you’ve tried
- how the medication affects your pain, function and quality of life
- your life circumstances.
If it’s appropriate to trial reducing or stopping opioids, guidelines from Australia, the United Kingdom and the United States emphasise the following principles:
1) Shared decision-making
Shared decision-making is where health-care professionals and patients work together to set goals, weigh risks and benefits, and make informed choices.
This means collaboratively designing an opioid reduction plan that reflects the person’s needs, preferences and circumstances, rather than imposing a one-size-fits-all approach.
Research shows shared decision-making may lead to better outcomes, and patients value this process.
2) Reduce gradually
Stopping opioids suddenly can cause withdrawal symptoms such as anxiety, insomnia, and stomach upset. Rapid dose reductions can also increase the risk of overdose, mental distress and suicide.
To avoid these risks, opioids should be reduced gradually over weeks, months or even longer. The process should be flexible, allowing for pauses or adjustments to the reduction plan if needed.
When someone takes lower doses of opioids over time, their body’s tolerance decreases. If they return to a higher dose, there is a risk of overdose. For this reason, health-care professionals may recommend having naloxone available. This is a medication that can reverse an opioid overdose.
3) Set up other supports
Supportive strategies should be used before, during and after reducing opioids. These can include:
- physical therapies such as physiotherapy
- psychological approaches such as mindfulness
- non-opioid medications
- mental health support from health-care professionals, friends and family
- education about pain self-management.
The evidence supporting specific interventions is often limited or uncertain. Choosing a strategy will depend on your individual preferences and access. The best approach is likely a combination of several different supports.
4) See your health-care provider for ongoing monitoring
Regular monitoring from a health-care professional is recommended during and after opioid reduction to assess pain, function, withdrawal symptoms and wellbeing.
This can help to ensure that any issues are identified early and are addressed.
If someone experiences a clear decline in their quality of life, for example, it may be necessary to pause or stop the taper and revisit it later, provide extra supports or implement strategies to manage withdrawal symptoms.
We need a health system that supports this process
Making opioid reduction safer and more effective requires putting these principles into practice. But many patients and health-care professionals still face challenges when doing so.
It’s best practice to access a team-based pain management program with support from a doctor, physiotherapist and psychologist, among other providers, to manage pain and reduce the use of opioids. But access to these services remains limited in many parts of Australia.
Not everyone has access to team-based pain management. Hispanolistic/Getty Images Consumer organisations and professional bodies have called for greater access to team-based pain services so more people, especially those living in rural and under-served areas, can access support.
Australian health-care professionals have also requested more education and training in pain management, prescribing and opioid reduction, as well as stronger evidence about what works, for whom and why. This is so they’re better able to tailor their care to each person’s needs.
Other strategies such as reducing the amount of opioids prescribed – including after surgery – have also been proposed to help prevent long-term opioid use and the need for reduction plans later on.
Aili Langford, Pharmacist, Lecturer, NHMRC Emerging Leadership Fellow, Sydney Pharmacy School, The University of Sydney, University of Sydney and Christine Lin, Professor, Institute for Musculoskeletal Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post




Related Posts
-
Rebuilding Better Bones At 55
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Doug Lucas shares a case study of a woman who went from osteoporotic to not within one year. Here’s how she did it:
From within
Ruth is a 55-year-old, small-framed, underweight woman with a strong family history of osteoporosis and multiple fractures.
Her risk factors included: negligible resistance training, recent fractures, early menopause, estrogen deficiency, and an ill-managed long-term vegan diet with low protein intake.
Note: the “ill-managed” there is, if you’ll pardon the pun, load-bearing. That is to say: a vegan diet is totally fine if you do it right, just as an omnivorous diet is totally fine if you do it right.
- In the case of an omnivorous diet, doing it right = avoiding red meat, avoiding processed meat, keeping saturated fat to a respectable minimum, remembering to get enough plants too
- Otherwise, you’ll have problems with your gut, heart, and more
- In the case of a vegan diet, doing it right = getting enough calcium, vitamin D, vitamin K, and protein
- Otherwise, you’ll have problems with your bones
Ruth’s situation, in numbers: spine T-score declined from –3.5 to –4.1 before treatment, with hips around –2.6, placing her at very high fracture risk.
For any unfamiliar with how these scores work, those are standard deviations from the norm (i.e. a score of zero would be the absolute norm) for one’s age, sex, menopause status if applicable, and broad ethnic grouping.
In Ruth’s case, the biggest issue was hormonal: she had a fear of HRT that stemmed from a mother’s early metastatic breast cancer, which had nothing to do with HRT, but there was that very misleading and popularly misrepresented study that caused a lot of people to believe it was causing cancer.
So, after some reassurances, individualized HRT was started with estrogen, progesterone, testosterone, and DHEA, with appropriate monitoring along the way.
In the category of dietary factors, gut rehabilitation enabled higher protein tolerance, while supplements were streamlined to focus on metabolism, detoxification, and cardiovascular support. Her protein intake was increased from 30–40g per day to over 100g per day.
As for exercise, her running was replaced with a gradual reintroduction of resistance training after her vertebral fracture, starting with bodyweight work, then weighted vests, and osteogenic loading devices.
Her results so far, by the time this video was made (one year after she began working on this):
- spine bone mineral density improved about 10%
- hips improved 7.4%, moving out of the osteoporosis range
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
21% Stronger Bones in a Year at 62? Yes, It’s Possible (No Calcium Supplements Needed!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- In the case of an omnivorous diet, doing it right = avoiding red meat, avoiding processed meat, keeping saturated fat to a respectable minimum, remembering to get enough plants too
-
What is retinol? And will it make my acne flare? 3 experts unpack this trendy skincare ingredient
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Retinol skincare products suddenly seem to be everywhere, promising clear, radiant and “youthful” skin.
But what’s the science behind these claims? And are there any risks?
You may have also heard retinol can increase your risk of sunburn and even make acne worse.
For some people, retinol may help reduce the appearance of fine lines. But it won’t be suitable for everyone. Here’s what you need to know.
Irina Kvyatkovskaya/Shutterstock What is retinol?
Retinol is part of a family of chemical compounds called retinoids. These are derived from or related to Vitamin A, a nutrient essential for healthy skin, vision and immune function.
All retinoids work because enzymes in our skin convert them into their “active” form, retinoic acid.
You can buy retinol in creams and other topical products over the counter.
These are often promoted as “anti-ageing” because retinol can help reduce the appearance of fine lines, wrinkles and even out skin tone (for example, sun spots or acne scars).
It also has an exfoliating effect, meaning it can help unclog pores.
Stronger retinoid treatments that target acne will require a prescription because they contain retinoic acid, which is regulated as a drug in the United States, European Union, United Kingdom and Australia.
How is retinol used in skincare?
One of the most common claims about retinol is that it helps to reduce visible signs of ageing.
How does this work?
With age, the skin’s barrier becomes weaker, making it more prone to dryness, injury and irritation.
Retinol can help counteract this natural thinning by stimulating the proliferation of keratinocytes – cells that form the outer skin layer and protect against damage and water loss.
Retinol also stimulates the production of collagen (a key protein that creates a scaffolding that keeps skin firm and elastic) and fibroblasts (cells that produce collagen and support skin structure).
It also increases how fast the skin sheds old cells and replaces them with new ones.
Over time, these processes help reduce fine lines, fade dark spots and even out skin tone. It can also make skin appear clearer.
While effective, this doesn’t happen overnight.
You may have also heard about a “retinol purge” – a temporary flare of acne when you first start using topical retinoids.
Studies have found the skin may become irritated and acne temporarily worsen in some cases. But more research needs to be done to understand this link.
The idea of a retinol purge is popular on social media. TikTok, CC BY-NC-ND So, is retinol safe?
At typical skincare concentrations (0.1–0.3%), side effects tend to be mild.
Most people who experience irritation (such as redness, dryness, or peeling) when starting retinol are able to build tolerance over time. This process is often called “retinisation”.
However, retinol increases the skin’s sensitivity to UV radiation (known as photosensitivity). This heightened reactivity can lead to sunburn, irritation and an increased risk of hyperpigmentation (spots or patches of darker colour).
For this reason, daily use of broad-spectrum sunscreen (SPF30 or higher) is strongly recommended while using retinol products.
Who should avoid retinol?
Teenagers and children generally don’t need retinol unless specifically prescribed by a doctor, for example, for acne treatment.
People with sensitive skin or conditions such as eczema (dry, itchy and inflamed skin) and rosacea (chronic redness and sensitivity) may find retinol too irritating.
Using retinol products alongside other skincare treatments, such as alpha-hydroxy acids, can over-exfoliate your skin and damage it.
Importantly, the active form of retinol, retinoic acid, is teratogenic (meaning it can cause birth defects). Over-the-counter retinol products are also not recommended during pregnancy or breastfeeding.
Choose and store retinol products wisely
Since retinol is classified as a cosmetic ingredient, companies are not required to disclose its concentration in their products.
The European Union is expected to introduce new regulations that will cap the concentration of retinol in cosmetic facial products to 0.3%.
These are precautionary measures aimed to limit exposure for vulnerable groups, such as pregnant women, given the risk of birth defects.
It’s therefore recommended to use products that clearly state the retinol concentration is between 0.1% and 0.3%.
Retinol is also a notoriously unstable molecule that degrades with exposure to air, light or heat.
Choosing a product with airtight, light-protective packaging will help with potential degradation problems that could lead to inactivity or harm.
What’s the safest way to try retinol?
The key is to go low and slow: a pea-sized amount of a low-concentration product (0.1%) once or twice a week, preferably at night (to avoid UV exposure), and then the frequency and concentration can be increased (to a maximum of 0.3%) as the skin adjusts.
Using a moisturiser after retinol helps to reduce dryness and irritation.
Wearing sunscreen every day is a must when using retinol to avoid the photosensitivity.
If you experience persistent redness, burning, or peeling, it’s better to stop using the product and consult your doctor or a dermatologist for personalised advice.
Laurence Orlando, Senior Lecturer, Product Formulation and Development, Analytical Methods, Monash University; Zanfina Ademi, Professor of Health Economics, Monash University, and Zoe Porter, Lecturer, Pharmacy and Pharmaceutical Science, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

It’s Not Hysteria – by Dr. Karen Tan
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Firstly, who this book is aimed at: in case it wasn’t clear, this book assumes you have, or at least have had, a uterus. If that’s not you, then well, it’ll still be an interesting read but it won’t be about your reproductive health.
Secondly, about that “reproductive health”: it’s mostly not actually about reproductive health literally, but rather, the health of one’s reproductive organs and the things that they affect—which is a lot more than the ability to reproduce!
Dr. Tang takes us on a (respectably in-depth) tour of the relevant anatomy, before moving on to physiology, before continuing to pathology (i.e. things that can go wrong, and often do), and finally various treatment options, including elective procedures, and the pros and cons thereof.
She also talks the reader through talking about things with gynecologists and other healthcare providers, and making sure concerns are not dismissed out-of-hand (something that happens a lot, of course).
The style throughout is quite detailed prose, but without being difficult at all to read, and (assuming one is interested in the topic) it’s very engaging.
Bottom line: if you would like to know more about uteri and everything that is (or commonly/unfortunately) can be attached to them, the effects they have on the rest of the body and health, and what can be done about things not being quite right, then this is a good book for that.
Click here to check out It’s Not Hysteria, and understand more of what’s going on down there!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: