Can Ginkgo Tea Be Made Safe? (And Other Questions)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I’d be interested in OTC prostrate medication safety and effectiveness.❞
Great idea! Sounds like a topic for a main feature one day soon, but while you’re waiting, you might like this previous main feature we did, about a supplement that performs equally to some prescription BPH meds:
❝Was very interested in the article on ginko bilboa as i moved into a home that has the tree growing in the backyard. Is there any way i can process the leaves to make a tea out of it.❞
Glad you enjoyed! First, for any who missed it, here was the article on Ginkgo biloba:
Ginkgo Biloba, For Memory And, Uh, What Else Again?
Now, as that article noted, Ginkgo biloba seeds and leaves are poisonous. However, there are differences:
The seeds, raw or roasted, contain dangerous levels of a variety of toxins, though roasting takes away some toxins and other methods of processing (boiling etc) take away more. However, the general consensus on the seeds is “do not consume; it will poison your liver, poison your kidneys, and possibly give you cancer”:
Ginkgo biloba L. seed; A comprehensive review of bioactives, toxicants, and processing effects
The leaves, meanwhile, are much less poisonous with their ginkgolic acids, and their other relevant poison is very closely related to that of poison ivy, involving long-chain alkylphenols that can be broken down by thermolysis, in other words, heat:
However, this very thorough examination of the potential health benefits and risks of ginkgo tea, comes to the general conclusion “this is not a good idea, and is especially worrying in elders, and/or if taking various medications”:
In summary:
- Be careful
- Avoid completely if you have a stronger-than-usual reaction to poison ivy
- If you do make tea from it, green leaves appear to be safer than yellow ones
- If you do make tea from it, boil and stew to excess to minimize toxins
- If you do make tea from it, doing a poison test is sensible (i.e. start with checking for a skin reaction to a topical application on the inside of the wrist, then repeat at least 6 hours later on the lips, then at least 6 hours later do a mouth swill, then at least 12 hours later drink a small amount, etc, and gradually build up to “this is safe to consume”)
For safety (and legal) purposes, let us be absolutely clear that we are not advising you that it is safe to consume a known poisonous plant, and nor are we advising you to do so.
But the hopefully only-ever theoretical knowledge of how to do a poison test is a good life skill, just in case
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Is Rabies The Most Lethal Infectious Disease?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We may not hear of epidemics or pandemics, but…
In bite-size terms…
Rabies is caused by viruses in the Lyssavirus genus, especially the classical rabies virus, which infects the mammalian nervous system and thus can (and all-too-often does) spread through mammals.
Transmission usually occurs through saliva entering tissue via a bite, but even just saliva contacting vulnerable areas can also pose a risk, and infections closer to the head can progress more quickly because the virus travels towards the brain through nerves.
Why rabies is hard to stop: rabies virions can remain hidden for days, months, or (rarely) even years, while suppressing parts of the immune response, and travel inside nerve cells at up to 10cm per day, which helps shield them from immune defenses too.
Once the virus reaches the central nervous system, symptoms begin rapidly as the infection spreads through nervous tissue, initially causing flu-like illness before progressing into severe neurological disease.
Why rabies is so deadly: rabies viruses usually avoid triggering strong inflammation in the brain, preventing immune cells and many therapies from reaching infected tissue effectively, and once symptoms appear, rabies is almost always fatal.
Pre-exposure and post-exposure rabies vaccinations are highly effective if (and usually only if) administered before symptoms develop, preventing the virus from reaching the central nervous system. In contrast, very few people have survived symptomatic rabies, usually after intensive medical care and often with lasting neurological damage.
For this reason, even merely possible exposures, such as waking to find a bat in a bedroom, merit urgent medical evaluation—precisely because rabies prevention is only reliably effective before symptoms begin.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Lyssavirus is rare, but deadly. What should you do if a bat bites you?
Take care!
Share This Post
-

What are ‘collarium’ sunbeds? Here’s why you should stay away
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Reports have recently emerged that solariums, or sunbeds – largely banned in Australia because they increase the risk of skin cancer – are being rebranded as “collarium” sunbeds (“coll” being short for collagen).
Commercial tanning and beauty salons in Queensland, New South Wales and Victoria are marketing collariums, with manufacturers and operators claiming they provide a longer lasting tan and stimulate collagen production, among other purported benefits.
A collarium sunbed emits both UV radiation and a mix of visible wavelength colours to produce a pink or red light. Like an old-school sunbed, the user lies in it for ten to 20 minute sessions to quickly develop a tan.
But as several experts have argued, the providers’ claims about safety and effectiveness don’t stack up.
Why were sunbeds banned?
Commercial sunbeds have been illegal across Australia since 2016 (except for in the Northern Territory) under state-based radiation safety laws. It’s still legal to sell and own a sunbed for private use.
Their dangers were highlighted by young Australians including Clare Oliver who developed melanoma after using sunbeds. Oliver featured in the No Tan Is Worth Dying For campaign and died from her melanoma at age 26 in 2007.
Sunbeds lead to tanning by emitting UV radiation – as much as six times the amount of UV we’re exposed to from the summer sun. When the skin detects enough DNA damage, it boosts the production of melanin, the brown pigment that gives you the tanned look, to try to filter some UV out before it hits the DNA. This is only partially successful, providing the equivalent of two to four SPF.
Essentially, if your body is producing a tan, it has detected a significant amount of DNA damage in your skin.
Research shows people who have used sunbeds at least once have a 41% increased risk of developing melanoma, while ten or more sunbed sessions led to a 100% increased risk.
In 2008, Australian researchers estimated that each year, sunbeds caused 281 cases of melanoma, 2,572 cases of squamous cell carcinoma (another common type of skin cancer), and $3 million in heath-care costs, mostly to Medicare.
How are collarium sunbeds supposed to be different?
Australian sellers of collarium sunbeds imply they are safe, but their machine descriptions note the use of UV radiation, particularly UVA.
UVA is one part of the spectrum of UV radiation. It penetrates deeper into the skin than UVB. While UVB promotes cancer-causing mutations by discharging energy straight into the DNA strand, UVA sets off damage by creating reactive oxygen species, which are unstable compounds that react easily with many types of cell structures and molecules. These damage cell membranes, protein structures and DNA.
Evidence shows all types of sunbeds increase the risk of melanoma, including those that use only UVA.
Some manufacturers and clinics suggest the machine’s light spectrum increases UV compatibility, but it’s not clear what this means. Adding red or pink light to the mix won’t negate the harm from the UV. If you’re getting a tan, you have a significant amount of DNA damage.
Collagen claims
One particularly odd claim about collarium sunbeds is that they stimulate collagen.
Collagen is the main supportive tissue in our skin. It provides elasticity and strength, and a youthful appearance. Collagen is constantly synthesised and broken down, and when the balance between production and recycling is lost, the skin loses strength and develops wrinkles. The collagen bundles become thin and fragmented. This is a natural part of ageing, but is accelerated by UV exposure.

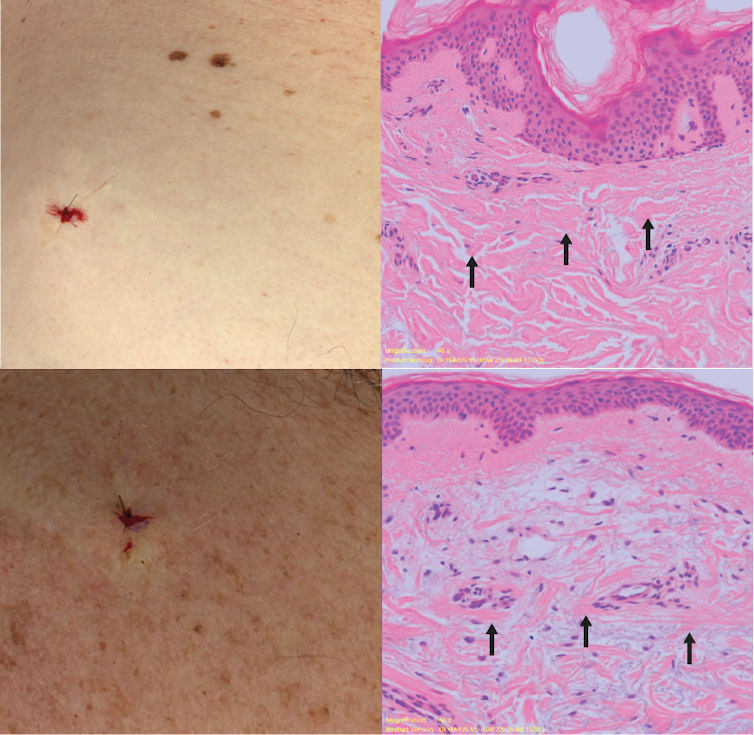
Sun-protected skin (top) has thick bands of pink collagen (arrows) in the dermis, as seen on microscopic examination. Chronically sun-damaged skin (bottom) has much thinner collagen bands.
Katie Lee/UQThe reactive oxygen species generated by UVA light damage existing collagen structures and kick off a molecular chain of events that downgrades collagen-producing enzymes and increases collagen-destroying enzymes. Over time, a build-up of degraded collagen fragments in the skin promotes even more destruction.
While there is growing evidence red light therapy alone could be useful in wound healing and skin rejuvenation, the UV radiation in collarium sunbeds is likely to undo any benefit from the red light.
What about phototherapy?
There are medical treatments that use controlled UV radiation doses to treat chronic inflammatory skin diseases like psoriasis.
The anti-collagen effects of UVA can also be used to treat thickened scars and keloids. Side-effects of UV phototherapy include tanning, itchiness, dryness, cold sore virus reactivation and, notably, premature skin ageing.
These treatments use the minimum exposure necessary to treat the condition, and are usually restricted to the affected body part to minimise risks of future cancer. They are administered under medical supervision and are not recommended for people already at high risk of skin cancer, such as people with atypical moles.
So what happens now?
It looks like many collariums are just sunbeds rebranded with red light. Queensland Health is currently investigating whether these salons are breaching the state’s Radiation Safety Act, and operators could face large fines.
As the 2024 Australians of the Year – melanoma treatment pioneers Georgina Long and Richard Scolyer – highlighted in their acceptance speech, “there is nothing healthy about a tan”, and we need to stop glamorising tanning.
However, if you’re desperate for the tanned look, there is a safer and easy way to get one – out of a bottle or by visiting a salon for a spray tan.

Katie Lee, PhD Candidate, Dermatology Research Centre, The University of Queensland and Anne Cust, Professor of Cancer Epidemiology, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
What’s the link between talcum powder and cancer?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More than 1,300 Victorians have joined a class action against Johnson & Johnson alleging its talcum powder products left them with ovarian cancer, mesothelioma (cancer affecting the lungs) and other cancers affecting the reproductive organs.
This follows lawsuits in the United Kingdom and the United States, including a prominent case in California. In December 2025, Johnson & Johnson was forced to pay two women US$40 million after a jury found its baby powder was dangerous and that it had failed to warn consumers.
Talc is a naturally occurring mineral mined in many parts of the world. People can come into contact with it during mining and processing, industrial applications, and more commonly, through its use in cosmetics and body powders.
People use talc on their genitals to absorb moisture, reduce friction, disguise odours, or to reduce skin rashes and chafing. Talc increases the opaqueness of face powders and cosmetics, leaving skin feeling smooth and soft.
So how is it linked to cancer? And what does the scientific evidence say?
Contamination with asbestos
Since the 1970s, questions have emerged about whether talc could be contaminated with asbestos. Asbestos is a cancer-causing agent that can affect the lungs when inhaled.
Talc and asbestos are minerals often found close to each other in the Earth, so there is potential for talc to be contaminated with asbestos during the mining process.
Since the 1970s, manufacturers have attempted to produce pure talcum powder free from asbestos. However, it’s unclear how routinely samples are tested and the extent of contamination over the past 50 years.
In 2023, Johnson & Johnson stopped selling talc in its products worldwide, including in Australia, switching instead to a cornflour base. Other manufacturers still sell talcum powder and it’s still used in cosmetics, as well as industrially.
What does the science say about the cancer link?
Two cancers have a possible link with talc use:
- lung cancer, due to the potential to inhale talc particles, which can occur with some types of jobs
- ovarian cancer, due to regular use of talcum powder in the genital area.
Some human studies have found products containing talc are linked with higher rates of ovarian cancer. Other studies have found no link.
Studies that examined the use of talc on the genital area found no evidence to suggest a link between talc and uterine or cervical cancer.
But there are several challenges to overcome when studying the link between talcum powder and cancer. It can be difficult to recall details about talc use (brand, amount, and so on) many years later. Some people who developed cancer will have died before being identified and studied, so won’t be included.
However, when researchers investigated how often participants used talc powder and compared those who used it frequently with those who didn’t, they found an increased risk of ovarian cancer among frequent users.
So what does it all mean?
When there are differing results from multiple studies, those results can be summarised together to answer the research question. So what does all the currently available evidence say about the relationship between talc usage and ovarian cancer?
This summary study concludes there appears to be a weak risk of some types of ovarian cancer, meaning it’s linked to a small increase in risk, but the reasons why remain unclear.
The evidence suggests talc does not increase the risk of other gynaecological cancers, such as uterine and cervical.
Talc contaminated with asbestos is clearly linked to an increased risk of lung cancer. However, cosmetic use of talc doesn’t seem to increase the risk of lung cancer because users don’t breathe it in.
In 2024 the World Health Organization (WHO) updated its advice to say that talc is “probably carcinogenic” which means it probably causes cancer in humans. This is the second-highest risk level for cancer, which includes the herbicide glyphosate (Roundup) and red meat.
If you use talcum powder and are concerned about an increased risk of cancer, it’s recommended you stop using it or limit how much you use. As with all decisions in life, consider the balance between potential harms and benefits, especially if you’ve used talc for a long time and want to minimise your risk of getting cancer.
Tam Ha, Associate Professor of Cancer Epidemiology, University of Wollongong
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post


Related Posts
-

Why Doctors Skip Breakfast – by Dr. Gregory Charlop
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book is what it claims to be in the subtitle: “[a collection of] wellness tips to reverse aging, treat depression, and get a good night’s sleep”. It’s not delivered quite like that though—one might expect this to be a page-a-day reader with one tip per page, for example, and it isn’t.
Instead, Dr. Charlop oscillates between telling stories (of the anecdotal variety, though they do come across as illustrative fictions rather than actual case studies with names changed) and sharing his thoughts on various topics, much as one might if talking to a friend or other small social audience in a casual manner.
As such, it’s very easy-reading, while at the same time not being necessarily conducive to skimming, as then one may miss the information buried in the text.
The knowledge itself is probably not anything that regular readers of 10almonds won’t have read before, but it can be good to have a reminder in any case; it’s easy to let things slip, get distracted from a good habit and then not reprise it, that sort of thing, so books like this can function as a timely prompt to make use of various wellness tools and techniques.
As for practicality, some things can be done quickly and easily (such as the intermittent fasting alluded to by the title, for example) whereas others will require investing more time and/or money, but all are at least worthy of consideration.
The style is, as we say, casual—but there is a bibliography and list of further references, so that’s a point in its favor, especially as the book itself is not very long or information-dense.
Bottom line: while there is nothing groundbreaking here, this book will provide a refresher on what for 10almonds readers might be considered the basics, plus some pet interests of the author’s (such as red light therapy and ketamine, which while they have their place, cannot be described as “the basics” of good health; the former is a very nice extra, and the latter has its pros and cons).
Click here to check out Why Doctors Skip Breakfast, and see how your health habits measure up!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Gravitas – by Caroline Goyder
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A no-nonsense guide to (more than!) public speaking that isn’t just “tell jokes in your speech and imagine the audience naked”.
Because this isn’t just about speech-writing or speech delivery, so much as giving you important life skills. The kind that weren’t taught in school, but that nevertheless make a huge impact on success… whether you’re giving a presentation or hosting a party or negotiating a deal or just attending a social event. Or making a phonecall, even.
Whereas a lot of books of this kind treat “the audience” as a nebulous and purely responsive passive crowd of extras, Goyder does better. People are individuals, even if they’re all facing the same way for a moment. She works with that! She also teaches how to deal with not just hecklers, but also simply those people who sap your confidence and find fault with you and anything you do or say.b
Bottom line is: if you for whatever reason communicate with people, and would like them to think better of you, this is the book for you.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Anti-Allergy Nasal Spray That Kills COVID & More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s a surprising headline, because the primary function of an anti-allergy medication is generally to dial down the immune system.
Thus, if you want to defend against a virus, then one would expect that the last thing you’d want to squirt up your nose (aside, perhaps, from the virus itself) would be an anti-allergen.
And yet…
Azelastine’s antiviral powers
Researchers (Dr. Thorsten Lehr et al.) investigated the effects of a common anti-allergy nasal spray (azelastine) against various kinds of respiratory virus infection, including COVID.
What they did: 450 participants were split into two groups; 227 used azelastine nasal spray three times daily for 56 days, 223 used a placebo spray.
What they found: only 2.2% of the azelastine group got infected with SARS-CoV-2 versus 6.7% in the placebo group, a very statistically-significant threefold difference.
They further found: only 1.8% of the azelastine group got infected with rhinovirus versus 6.3% in the placebo group, reflecting the anti-COVID result.
But COVID and rhinovirus are both enteroviruses, and enterovirus can often be beaten with measures that don’t work on other viruses, because the chemical “envelope” that contains them can be disrupted—not something one can do vs an unenveloped virus (such as influenza) which doesn’t have an envelope to disrupt.
So, how does it perform vs flu? There’s good and bad news:
- Good news: azelastine does have anti-viral properties that work against flu also
- Bad news: or rather, good for the study participants but bad for science—the overall number of cases of flu in this study population was too low for statistical significance.
For azelastine’s antiviral-vs-flu properties, see this older, in vitro study:
Antiviral Potential of Azelastine against Major Respiratory Viruses
For the study we’ve been talking about today, you can find the paper itself here:
Azelastine Nasal Spray for Prevention of SARS-CoV-2 Infections
How useful is this?
The researchers emphasize (as researchers always do) the need for larger, multicentre studies to confirm results and test effectiveness against other respiratory pathogens, but as it stands, they are confident enough to say that this could serve as a cheap, accessible preventive option, particularly for vulnerable groups and/or during travel and high-risk periods (i.e. when there’s a local spike in cases, and/or you will be unavoidably in a high-risk situation, e.g. being in a closed environment with many people for a while).
If you’d like some, you can get it from your local pharmacy or online; we don’t sell it, but here’s an example product for your convenience.
There, of course, also other ways to improve the odds to keep yourself and your loved ones safe:
Vaccines are considered the “gold standard” against COVID and many other infectious diseases, for their very high rate of efficacy, clear science, and at least moderately lasting effects (i.e., it’s not something like handwashing*, which must be redone very frequently).
Since vaccines are not without their popular misunderstanders, we have written a little about that, here: Vaccine Mythbusting
*See also: The Truth About Handwashing ← for another mythbusting edition, covering what actually works against what, and what doesn’t—as well as the disparity between people’s self-reports of handwashing, and how often/well they actually wash their hands!
So, those are important ones, but still not the only things we can do; consider for example: Beyond Supplements: The Real Immune-Boosters! ← most people don’t know these things and the huge difference they make
And for that matter: Why Some People Get Sick More (And How To Not Be One Of Them) ← for a very prophylactic approach
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: