A person in Texas caught bird flu after mixing with dairy cattle. Should we be worried?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The United States’ Centers for Disease Control and Prevention (CDC) has issued a health alert after the first case of H5N1 avian influenza, or bird flu, seemingly spread from a cow to a human.
A farm worker in Texas contracted the virus amid an outbreak in dairy cattle. This is the second human case in the US; a poultry worker tested positive in Colorado in 2022.
The virus strain identified in the Texan farm worker is not readily transmissible between humans and therefore not a pandemic threat. But it’s a significant development nonetheless.
Some background on bird flu
There are two types of avian influenza: highly pathogenic or low pathogenic, based on the level of disease the strain causes in birds. H5N1 is a highly pathogenic avian influenza.
H5N1 first emerged in 1997 in Hong Kong and then China in 2003, spreading through wild bird migration and poultry trading. It has caused periodic epidemics in poultry farms, with occasional human cases.
Influenza A viruses such as H5N1 are further divided into variants, called clades. The unique variant causing the current epidemic is H5N1 clade 2.3.4.4b, which emerged in late 2020 and is now widespread globally, especially in the Americas.
In the past, outbreaks could be controlled by culling of infected birds, and H5N1 would die down for a while. But this has become increasingly difficult due to escalating outbreaks since 2021.
Wild animals are now in the mix
Waterfowl (ducks, swans and geese) are the main global spreaders of avian flu, as they migrate across the world via specific routes that bypass Australia. The main hub for waterfowl to migrate around the world is Quinghai lake in China.
But there’s been an increasing number of infected non-waterfowl birds, such as true thrushes and raptors, which use different flyways. Worryingly, the infection has spread to Antarctica too, which means Australia is now at risk from different bird species which fly here.
H5N1 has escalated in an unprecedented fashion since 2021, and an increasing number of mammals including sea lions, goats, red foxes, coyotes, even domestic dogs and cats have become infected around the world.
Wild animals like red foxes which live in peri-urban areas are a possible new route of spread to farms, domestic pets and humans.
Dairy cows and goats have now become infected with H5N1 in at least 17 farms across seven US states.
What are the symptoms?
Globally, there have been 14 cases of H5N1 clade 2.3.4.4b virus in humans, and 889 H5N1 human cases overall since 2003.
Previous human cases have presented with a severe respiratory illness, but H5N1 2.3.4.4b is causing illness affecting other organs too, like the brain, eyes and liver.
For example, more recent cases have developed neurological complications including seizures, organ failure and stroke. It’s been estimated that around half of people infected with H5N1 will die.
The case in the Texan farm worker appears to be mild. This person presented with conjunctivitis, which is unusual.
Food safety
Contact with sick poultry is a key risk factor for human infection. Likewise, the farm worker in Texas was likely in close contact with the infected cattle.
The CDC advises pasteurised milk and well cooked eggs are safe. However, handling of infected meat or eggs in the process of cooking, or drinking unpasteurised milk, may pose a risk.
Although there’s no H5N1 in Australian poultry or cattle, hygienic food practices are always a good idea, as raw milk or poorly cooked meat, eggs or poultry can be contaminated with microbes such as salmonella and E Coli.
If it’s not a pandemic, why are we worried?
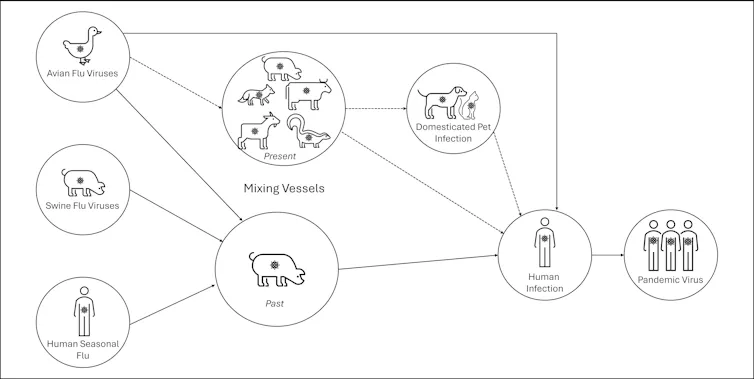
Scientists have feared avian influenza may cause a pandemic since about 2005. Avian flu viruses don’t easily spread in humans. But if an avian virus mutates to spread in humans, it can cause a pandemic.
One concern is if birds were to infect an animal like a pig, this acts as a genetic mixing vessel. In areas where humans and livestock exist in close proximity, for example farms, markets or even in homes with backyard poultry, the probability of bird and human flu strains mixing and mutating to cause a new pandemic strain is higher.
The cows infected in Texas were tested because farmers noticed they were producing less milk. If beef cattle are similarly affected, it may not be as easily identified, and the economic loss to farmers may be a disincentive to test or report infections.
How can we prevent a pandemic?
For now there is no spread of H5N1 between humans, so there’s no immediate risk of a pandemic.
However, we now have unprecedented and persistent infection with H5N1 clade 2.3.4.4b in farms, wild animals and a wider range of wild birds than ever before, creating more chances for H5N1 to mutate and cause a pandemic.
Unlike the previous epidemiology of avian flu, where hot spots were in Asia, the new hot spots (and likely sites of emergence of a pandemic) are in the Americas, Europe or in Africa.
Pandemics grow exponentially, so early warnings for animal and human outbreaks are crucial. We can monitor infections using surveillance tools such as our EPIWATCH platform.
The earlier epidemics can be detected, the better the chance of stamping them out and rapidly developing vaccines.
Although there is a vaccine for birds, it has been largely avoided until recently because it’s only partially effective and can mask outbreaks. But it’s no longer feasible to control an outbreak by culling infected birds, so some countries like France began vaccinating poultry in 2023.
For humans, seasonal flu vaccines may provide a small amount of cross-protection, but for the best protection, vaccines need to be matched exactly to the pandemic strain, and this takes time. The 2009 flu pandemic started in May in Australia, but the vaccines were available in September, after the pandemic peak.
To reduce the risk of a pandemic, we must identify how H5N1 is spreading to so many mammalian species, what new wild bird pathways pose a risk, and monitor for early signs of outbreaks and illness in animals, birds and humans. Economic compensation for farmers is also crucial to ensure we detect all outbreaks and avoid compromising the food supply.
C Raina MacIntyre, Professor of Global Biosecurity, NHMRC L3 Research Fellow, Head, Biosecurity Program, Kirby Institute, UNSW Sydney; Ashley Quigley, Senior Research Associate, Global Biosecurity, UNSW Sydney; Haley Stone, PhD Candidate, Biosecurity Program, Kirby Institute, UNSW Sydney; Matthew Scotch, Associate Dean of Research and Professor of Biomedical Informatics, College of Health Solutions, Arizona State University, and Rebecca Dawson, Research Associate, The Kirby Institute, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Garden Cress vs Watercress – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing garden cress to watercress, we picked the garden cress.
Why?
While watercress is (rightly!) popularly viewed as a superfood for its nutritional density, the garden variety actually outperforms it.
In terms of macros first, garden cress has more protein, carbs, and fiber, while also having the lower glycemic index. Not that anyone’s getting blood sugar spikes from eating any kind of cress, but still, by the numbers, this is a clear win on the whole for garden cress in the category of macros.
When it comes to vitamins, garden cress has a lot (tens of times) more of vitamins A, B2, B3, B6, B7, B9, C, K, and choline, while watercress has (slightly) more of vitamins B1, B5, and E. An easy win for garden cress.
In the category of minerals, garden cress has more copper, iron, magnesium, manganese, phosphorus, and potassium, while watercress has more calcium. Another clear win for garden cress.
Taking a quick peep at polyphenols in case there’s anything to offset the above, garden cress has 13x more kaempferol (13mg/100g to watercress’s 1mg/100g), and/but watercress, in its favor, has quercetin (at 4mg/100g), which garden cress doesn’t. So, we say this category is also a win for garden cress, but watercress has its merits too.
👆 Let’s clarify: those numbers are all very good, and garden cress’s 13mg/100g kaempferol is absurdly high; most such quotients of most edible plants are orders of magnitude smaller; not to shoehorn in another vegetable, but just to give an example, savoy cabbage, which won on nutritional density vs bok choi recently, has 0.26mg/100g kaempferol and 0.12mg/100g quercetin (which were already very respectable numbers), so you see the difference in cress’s exceptionally generous delivery of these polyphenols!
Adding up the sections makes for an overwhelming win for garden cress!
Want to learn more?
You might like to read:
Sprout Your Seeds, Grains, Beans, Etc ← cress is a great example of this!
Take care!
Share This Post
-
Brussels Sprouts vs Spirulina – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing Brussels sprouts to spirulina, we picked the sprouts.
Why?
Pitting these two well-known superfoods against each other, we get the following:
Looking at the macros first, spirulina has a little more protein, while sprouts have more carbs and nearly 10x the fiber. So, we call this a win for sprouts.
In terms of vitamins, sprouts have a lot more of vitamins A, B6, B9, C, E, K, and choline, while spirulina has a little more of vitamins B1, B2, and B3. An easy win for sprouts.
In the category of minerals, sprouts have more calcium, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while spirulina has more copper and iron. Another clear win for sprouts.
Adding up the sections makes the winner very clear: Brussels sprouts enjoy a well-earned victory.
Want to learn more?
You might like to read:
Take care!
Share This Post
-
Entertaining Harissa Traybake
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
No, it’s not entertaining in the sense that it will tell you jokes or perhaps dance for you, but rather: it can be easily prepared in advance, kept in the fridge for up to 3 days, and reheated when needed as part of a spread when entertaining, leaving you more time to spend with your houseguests.
Aside from its convenience, it is of course nutritious and delicious:
You will need
- 14 oz cherry tomatoes
- 2 cans chickpeas, drained and rinsed (or 2 cups cooked chickpeas, drained and rinsed)
- 2 eggplants, cut into ¾” cubes
- 1 red onion, roughly chopped
- 1 bulb garlic
- 2 tbsp extra virgin olive oil
- 1 tbsp harissa paste
- 1 tbsp ras el-hanout
- 1 tsp MSG or 2 tsp low-sodium salt
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 400℉ / 200℃
2) Mix the onion, eggplant, and garlic (whole cloves; just peel them and put them in) with the olive oil in a mixing bowl, ensuring everything is coated evenly.
3) Add in 1 tbsp of the harissa paste, 1 tbsp of the ras-el hanout, and half of the MSG/salt, and again mix thoroughly to coat evenly.
4) Bake in the oven, in a walled tray, for about 30 minutes, giving things a stir/jiggle halfway through to ensure they cook evenly.
5) Add the cherry tomatoes to the tray, and return to the oven for another 10 minutes.
6) Mix the chickpeas with the other 1 tbsp of the harissa paste, the other 1 tbsp of the ras-el hanout, and the other half of the MSG/salt, and add to the tray, returning it to the oven for a final 10 minutes.
7) Serve hot, or set aside for later, refrigerating once cool enough to do so. When you do serve, we recommend serving with a yogurt, cucumber, and mint dip, and perhaps flatbreads (you can use our Healthy Homemade Flatbreads recipe):

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Eat More (Of This) For Lower Blood Pressure
- Lycopene’s Benefits For The Gut, Heart, Brain, & More
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Share This Post


Related Posts
-
What’s Your Plant Diversity Score?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We speak often about the importance of dietary diversity, and of that, especially diversity of plants in one’s diet, but we’ve never really focused on it as a main feature, so that’s what we’re going to do today.
Specifically, you may have heard the advice to “eat 30 different kinds of plants per week”. But where does that come from, and is it just a number out of a hat?
The magic number?
It is not, in fact, a number out of a hat. It’s from a big (n=11,336) study into what things affect the gut microbiome for better or for worse. It was an observational population study, championing “citizen science” in which volunteers tracked various things and collected and sent in various samples for analysis.
The most significant finding of this study was that those who consumed more than 30 different kinds of plants per week, had a much better gut microbiome than those who consumed fewer than 10 different kinds of plants per week (there is a bell curve at play, and it gets steep around 10 and 30):
American Gut: an Open Platform for Citizen Science Microbiome Research
Why do I care about having a good gut microbiome?
Gut health affects almost every other kind of health; it’s been called “the second brain” for the various neurotransmitters and other hormones it directly makes or indirectly regulates (which in turn affect every part of your body), and of course there is the vagus nerve connecting it directly to the brain, impacting everything from food cravings to mood swings to sleep habits.
See also:
Any other benefits?
Yes there are! Let’s not forget: as we see often in our “This or That” section, different foods can be strong or weak in different areas of nutrition, so unless we want to whip out a calculator and database every time we make food choices, a good way to cover everything is to simply eat a diverse diet.
And that goes not just for vitamins and minerals (which would be true of animal products also), but in the case of plants, a wide range of health-giving phytochemicals too:
Measuring Dietary Botanical Diversity as a Proxy for Phytochemical Exposure
Ok, I’m sold, but 30 is a lot!
It is, but you don’t have to do all 30 in your first week of focusing on this, if you’re not already accustomed to such diversity. You can add in one or two new ones each time you go shopping, and build it up.
As for “what counts”: we’re counting unprocessed or minimally-processed plants. So for example, an apple is an apple, as are dried apple slices, as is apple sauce. Any or all of those would count as 1 plant type.
Note also that we’re counting types, not totals. If you’re having apple slices with apple sauce, for some reason? That still only counts as 1.
However, while apple sauce still counts as apples (minimally processed), you cannot eat a cake and say “that’s 2 because there was wheat and sugar cane somewhere in its dim and distant history”.
Nor is your morning espresso a fruit (by virtue of coffee beans being the fruit of the plant, botanically speaking). However, it would count as 1 plant type if you eat actual coffee beans—this writer has been known to snack on such; they’re only healthy in very small portions though, because their saturated fat content is a little high.
You, however, count grains in general, as well as nuts and seeds, not just fruits and vegetables. As for herbs and spices, they count for ¼ each, except for salt, which might get lumped in with spices but is of course not a plant.
How to do it
There’s a reason we’re doing this in our Saturday Life Hacks edition. Here are some tips for getting in far more plants than you might think, a lot more easily than you might think:
- Buy things ready-mixed. This means buying the frozen mixed veg, the frozen mixed chopped fruit, the mixed nuts, the mixed salad greens etc. This way, when you’re reaching for one pack of something, you’re getting 3–5 different plants instead of one.
- Buy things individually, and mix them for storage. This is a more customized version of the above, but in the case of things that keep for at least a while, it can make lazy options a lot more plentiful. Suddenly, instead of rice with your salad you’re having sorghum, millet, buckwheat, and quinoa. This trick also works great for dried berries that can just be tipped into one’s morning oatmeal. Or, you know, millet, oats, rye, and barley. Suddenly, instead of 1 or 2 plants for breakfast you have maybe 7 or 8.
- Keep a well-stocked pantry of shelf-stable items. This is good practice anyway, in case of another supply-lines shutdown like at the start of the COVID-19 pandemic. But for plant diversity, it means that if you’re making enchiladas, then instead using kidney beans because that’s what’s in the cupboard, you can raid your pantry for kidney beans, black beans, pinto beans, fava beans, etc etc. Yes, all of them; that’s a list, not a menu.
- Shop in the discount section of the supermarket. You don’t have shop exclusively there, but swing by that area, see what plants are available for next to nothing, and buy at least one of each. Figure out what to do with it later, but the point here is that it’s a good way to get suggestions of plants that you weren’t actively looking for—and novelty is invariably a step into diversity.
- Shop in a different store. You won’t be able to beeline the products you want on autopilot, so you’ll see other things on the way. Also, they may have things your usual store doesn’t.
- Shop in person, not online—at least as often as is practical. This is because when shopping for groceries online, the store will tend to prioritize showing you items you’ve bought before, or similar items to those (i.e. actually the same item, just a different brand). Not good for trying new things!
- Consider a meal kit delivery service. Because unlike online grocery shopping, this kind of delivery service will (usually) provide you with things you wouldn’t normally buy. Our sometimes-sponsor Purple Carrot is a fine option for this, but there are plenty of others too.
- Try new recipes, especially if they have plants you don’t normally use. Make a note of the recipe, and go out of your way to get the ingredients; if it seems like a chore, reframe it as a little adventure instead. Honestly, it’s things like this that keep us young in more ways than just what polyphenols can do!
- Hide the plants. Whether or not you like them; hide them just because it works in culinary terms. By this we mean; blend beans into that meaty sauce; thicken the soup with red lentils, blend cauliflower into the gravy. And so on.
One more “magic 30”, while we’re at it…
30g fiber per day makes a big (positive) difference to many aspects of health. Obviously, plants are where that comes from, so there’s a big degree of overlap here, but most of the tips we gave are different, so for double the effectiveness, check out:
Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How to Change – by Katy Milkman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes it seems that we know everything we should be doing… We have systems and goals and principles, we know about the importance of habits, and we do our best to live them. Yet, somehow, life has other plans for us and things don’t quite come together they way they did in our genius masterplan.
So, what happened? And more importantly, what are we supposed to do about this? Katy Milkman has answers, right from the start.
Sometimes, it can be as simple as when we try to implement a change. It’s not that there’s a “wrong time” for a good change, so much that there are times that are much more likely to succeed than others… and those times can be identified and used.
Sometimes we’re falling prey to vices—which she explains how to overcome—such as:
- Impulsivity
- Procrastination
- Forgetfulness
- Laziness
We also learn some counterintuitive truths about what can boost or sabotage our confidence along the way!
Milkman writes in a compelling, almost narrative style, that makes for very easy reading. The key ideas, built up to by little (ostensibly true) stories and then revealed, become both clear and memorable. Most importantly, applicable.
Bottom line: this is a great troubleshooting guide for when you know how everything should be working, but somehow, it just doesn’t—and you’d like to fix that.
Click here to check out “How To Change” on Amazon, and get those changes rolling!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Managing Sibling Relationships In Adult Life
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Managing Sibling Relationships In Adult Life
After our previous main feature on estrangement, a subscriber wrote to say:
❝Parent and adult child relationships are so important to maintain as you age, but what about sibling relationships? Adult choices to accept and move on with healthier boundaries is also key for maintaining familial ties.❞
And, this is indeed critical for many of us, if we have siblings!
Writer’s note: I don’t have siblings, but I do happen to have one of Canada’s top psychologists on speed-dial, and she has more knowledge about sibling relationships than I do, not to mention a lifetime of experience both personally and professionally. So, I sought her advice, and she gave me a lot to work with.
Today I bring her ideas, distilled into my writing, for 10almonds’ signature super-digestible bitesize style.
A foundation of support
Starting at the beginning of a sibling story… Sibling relationships are generally beneficial from the get-go.
This is for reasons of mutual support, and an “always there” social presence.
Of course, how positive this experience is may depend on there being a lack of parental favoritism. And certainly, sibling rivalries and conflict can occur at any age, but the stakes are usually lower, early in life.
Growing warmer or colder
Generally speaking, as people age, sibling relationships likely get warmer and less conflictual.
Why? Simply put, we mature and (hopefully!) get more emotionally stable as we go.
However, two things can throw a wrench into the works:
- Long-term rivalries or jealousies (e.g., “who has done better in life”)
- Perceptions of unequal contribution to the family
These can take various forms, but for example if one sibling earns (or otherwise has) much more or much less than another, that can cause resentment on either or both sides:
- Resentment from the side of the sibling with less money: “I’d look after them if our situations were reversed; they can solve my problems easily; why do they resent that and/or ignore my plight?”
- Resentment from the side of the sibling with more money: “I shouldn’t be having to look after my sibling at this age”
It’s ugly and unpleasant. Same goes if the general job of caring for an elderly parent (or parents) falls mostly or entirely on one sibling. This can happen because of being geographically closer or having more time (well… having had more time. Now they don’t, it’s being used for care!).
It can also happen because of being female—daughters are more commonly expected to provide familial support than sons.
And of course, that only gets exacerbated as end-of-life decisions become relevant with regard to parents, and tough decisions may need to be made. And, that’s before looking at conflicts around inheritance.
So, all that seems quite bleak, but it doesn’t have to be like that.
Practical advice
As siblings age, working on communication about feelings is key to keeping siblings close and not devolving into conflict.
Those problems we talked about are far from unique to any set of siblings—they’re just more visible when it’s our own family, that’s all.
So: nothing to be ashamed of, or feel bad about. Just, something to manage—together.
Figure out what everyone involved wants/needs, put them all on the table, and figure out how to:
- Make sure outright needs are met first
- Try to address wants next, where possible
Remember, that if you feel more is being asked of you than you can give (in terms of time, energy, money, whatever), then this discussion is a time to bring that up, and ask for support, e.g.:
“In order to be able to do that, I would need… [description of support]; can you help with that?”
(it might even sometimes be necessary to simply say “No, I can’t do that. Let’s look to see how else we can deal with this” and look for other solutions, brainstorming together)
Some back-and-forth open discussion and even negotiation might be necessary, but it’s so much better than seething quietly from a distance.
The goal here is an outcome where everyone’s needs are met—thus leveraging the biggest strength of having siblings in the first place:
Mutual support, while still being one’s own person. Or, as this writer’s psychology professor friend put it:
❝Circling back to your original intention, this whole discussion adds up to: siblings can be very good or very bad for your life, depending on tons of things that we talked about, especially communication skills, emotional wellness of each person, and the complexity of challenges they face interdependently.❞
Our previous main feature about good communication can help a lot:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: