What Diabetes Does To Your Heart
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ll get straight to it: researchers (Dr. Jasmine Khor et al.) have found that type 2 diabetes physically remodels the human heart by disrupting energy production, weakening muscle structure, and increasing fibrous tissue (that is also bad), which, together, push the heart towards failure.
So, how does it do that and how can we avoid that unfortunate outcome?
At the heart of things
Type 2 diabetes reshaping the heart fits neatly into the bigger picture of metabolic syndrome, which absolutely bears mentioning because people tend to talk a lot about the parts, without talking about how it all comes together.
Metabolic syndrome is the name given to a cluster of energy-handling (thus: metabolic) problems—high blood sugar, insulin resistance, abdominal fat, abnormal lipids, and high blood pressure—which all strain the same biological systems. And yes, the effect compounds, with each part making the others worse, unless reversed.
In metabolic syndrome, cells across the body become less responsive to insulin, and the heart is no exception: it struggles to switch fuels efficiently, overworks its mitochondria, and gradually stiffens as fibrous tissue builds up. Over time, this energy mismatch and low-grade inflammation quietly remodel the heart muscle, making it less flexible and less efficient at pumping blood.
With that in mind, metabolic syndrome is not just a collection of risk factors on a checklist, but rather also a slow-motion metabolic stress test for the heart—one that can, if neglected, tip the heart from adaptation (i.e. dealing with problems better) into failure (i.e. literally, heart failure).
The aforementioned researchers at the University of Sydney analyzed donated human heart tissue from transplant recipients and compared it with tissue from (formerly)* healthy donors, allowing direct observation in humans rather than merely non-human animal models.
*Formerly healthy because, of course, the donors are dead. But what this means is that they died in otherwise good health, as can happen if accident or incident should befall.
What they found is that diabetes alters how heart cells generate energy by reducing insulin sensitivity in glucose transporters, increasing stress on mitochondria, and worsening the metabolic profile seen in advanced heart failure.
As part of this, diabetes also reduces key proteins involved in contraction and calcium regulation while promoting fibrosis, making the heart muscle stiffer and thus less efficient at pumping blood. These direct, tissue-level changes help explain why people with type 2 diabetes face a much higher risk of heart failure, beyond the shared risk factors alone.
You can read the paper in full, here: Left ventricular myocardial molecular profile of human diabetic ischaemic cardiomyopathy
What to do about it?
Here are some very good starting points:
- What Matters Most For Your Heart? ← perhaps not coincidentally, this is also what matters most for avoiding/reversing type 2 diabetes
- The Two Worst Things For Cardiac Aging
- Three Tweaks To Cut Diabetes Risk By 1/3
Want to learn more?
For a much deeper dive, you might like this excellent book we reviewed a while back:
Why We Get Sick – by Dr. Benjamin Bikman ← the title doesn’t really give it away, but we promise this book is very much specifically about this very topic, the science of how insulin resistance (not even the blood sugar imbalances that may result, but the insulin resistance itself already) leads to an increase in most other health risks (especially of the cardiometabolic variety), and why it’s a bigger problem sooner than people think from blood sugar tests alone, and what to do about it
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Fibromyalgia Is Not An Acceptable Diagnosis

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Efrat Lamandre makes the case that fibromyalgia is less of a useful diagnosis and more of a rubber stamp, much like the role historically often fulfilled by “heart failure” as an official cause of death (because certainly, that heart sure did stop beating). It’s a way of answering the question without answering the question.
…and what to look for instead
Fibromyalgia is characterized by chronic pain, tenderness, sleep disturbances, fatigue, and other symptoms. It’s often considered an “invisible” illness, because it’s the kind that’s easy to dismiss if you’re not the one carrying it. A broken leg, one can point at and see it’s broken; a respiratory infection, one can see its effects and even test for presence of the pathogen and/or its antigens. But fibromyalgia? “It hurts and I’m tired” doesn’t quite cut it.
Much like “heart failure” as a cause of death when nothing else is implicated, fibromyalgia is a diagnosis that gets applied when known causes of chronic pain have been ruled out.
Dr. Lamandre advocates for functional medicine and seeking the underlying causes of the symptoms, rather than the industry standard approach, which is to just manage the symptoms themselves with medications (of course, managing the symptoms with medications has its place; there is no need to suffer needlessly if pain relief can be used; it’s just not a sufficient response).
She notes that potential triggers for fibromyalgia include microbiome imbalances, food sensitivities, thyroid issues, nutrient deficiencies, adrenal fatigue, mitochondrial dysfunction, mold toxicity, Lyme disease, and more. Is this really just one illness? Maybe, but quite possibly not.
In short… If you are given a diagnosis of fibromyalgia, she advises that you insist doctors keep on looking, because that’s not an answer.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Managing Chronic Pain (Realistically!)
- How To Eat To Beat Chronic Fatigue ← yes, including how to do so when you are chronically fatigued. In other words, this isn’t just dietary advice, but rather practical advice too
- When Painkillers Aren’t Helping, These Things Might
Take care!
Share This Post
-

Recent outbreaks highlight the risks of bacterial meningitis and the need to vaccinate
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Outbreaks of bacterial meningococcal disease in England and recent cases in students in New Zealand have raised awareness of this serious and life-threatening disease.
The disease is caused by the bacterium Neisseria meningitidis and presents as meningitis or blood poisoning (septicaemia).
Meningitis is an inflammation of the membranes that cover the brain and spinal cord (meninges), while septicaemia affects the whole body through the presence of bacteria in the blood stream.
Both can be also be caused by other infectious agents, but bacterial meningococcal disease is the most severe form.
Infants, children and young adults are at higher risk. While the disease is largely preventable through vaccination, only one vaccine is currently on the national immunisation schedule in Aotearoa New Zealand.
As part of ongoing research to explain the recent cases, we compared the meningococcal strains involved in both countries and explored the significance of people who carry the bacterium but don’t develop symptoms or disease.
There are several strains of Neisseria meningitidis and most belong to six groups (named A, B, C, W, X and Y). All have an extraordinary ability to swap genetic material between them and switch genes on and off through a process known as phase variation.
This can change the surface of the bacterium, enabling it to escape the body’s immune system.
The strains responsible for both the UK and recent Dunedin cases belong to Group B meningococci. However, the similarity ends there. The UK outbreak strain is known as ST485, while the Dunedin cases were caused by different strains. They differ from the UK strain as well as from each other, suggesting more than one chain of transmission was involved.
The Bexsero vaccine is used to protect people against bacterial meningitis caused by group B strains. It was designed to recognise components in the outer membrane and on the surface of the bacteria.
The strain that caused the UK outbreak is likely covered by the Bexero vaccine because it matches exactly one of the protein antigen sequences used in the vaccine.
But genomic sequencing of the bacteria responsible for one of the Dunedin cases is still pending, while the other case did not yield a bacterial culture.

Students and staff queue to receive antibiotics at the UK University of Kent after an outbreak of meningitis caused the deaths of two people. Carl Court/Getty Images The importance of genome sequencing
Although meningococcal disease can appear as scattered and apparently unrelated cases, these can occasionally build into larger outbreaks.
Strain typing and genome sequencing can help to determine if an apparent outbreak is due to the emergence of a particular strain or a cluster of cases that are genetically unrelated.
Both scenarios can occur if cases share a common risk factor, such as increased close contact and mixing in educational settings such as schools and universities.
Past genomic surveillance in New Zealand has shown the emergence of outbreak strains and helped identify likely resistance to antibiotics. For example, a W group strain variant caused rising numbers of meningococcal disease between 2016 and 2019 in New Zealand and an outbreak in Northland in 2018.
Genome sequencing showed this strain was different from the W strain causing disease in Europe at the time, and the specific 2015 variant also has increased resistance to penicillin.
Healthy people can be carriers
Despite its ability to cause severe disease, the bacterium causing meningococcal disease is often found in people’s throat, without causing symptoms.
About 5% to 30% of the global population are carriers, and most don’t experience any symptoms or disease. We don’t yet fully understand the factors that determine whether disease develops.
Genome sequencing has shown that some highly virulent strains which are associated with outbreaks are rarely identified in samples from healthy carriers. But as yet, attempts to find genomic explanations for differences in bacteria found in outbreaks and healthy carriers remain inconclusive.
The likelihood whether people carry the bacterium is age dependent. It is low in younger children and older people, but high in teenagers and young adults.
The high carriage rate in young adults makes university students a high-risk group for developing the disease. Crowded living conditions also contribute to the high carriage rate, exacerbating the risk.
In New Zealand, both the Bexsero (against group B) and MenQuadfi (against ACWY) vaccines are available to young people moving into boarding school or university halls the first time. In contrast, only one vaccine (against ACWY) is currently funded for university students in England.
Both vaccines are needed to have maximum protection. Conjugate ACWY vaccines may reduce carriage and therefore transmission. Bexsero does not reduce carriage but protects against development of the disease.
Impact of COVID measures on transmission
Lockdowns and border controls introduced during the COVID pandemic reduced transmission of the SARS-CoV2 virus. But they also had a major effect on other diseases, including influenza and other respiratory viruses.
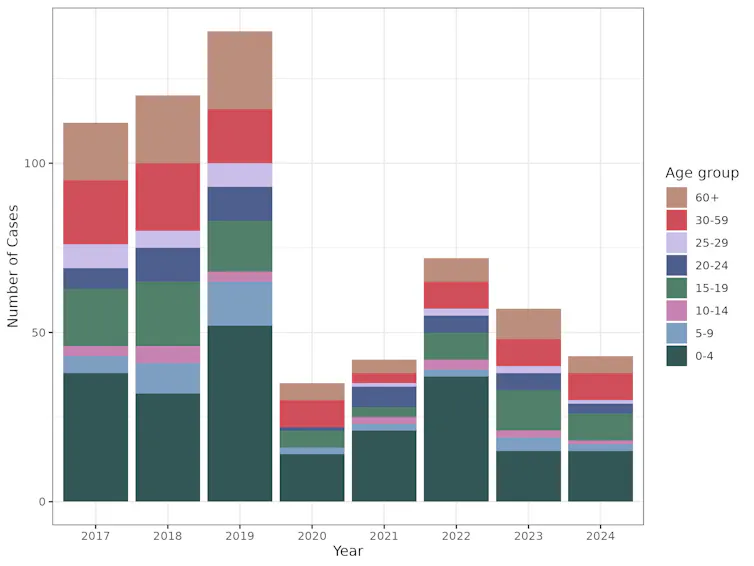
Cases of meningococcal disease were also dramatically reduced during the COVID response, most likely due to reduced contact between individuals and because fewer infected people entered the country.
This graph shows the drop in cases of meningococcal disease, across all age groups, during the period of COVID lockdowns. Data extracted from the PHF Science notifiable disease dashboard for meningococcal disease, CC BY-SA The rebound in cases following relaxation of these strict measures was expected.
This highlights how important it is to be aware of the risks associated with large gatherings, particularly of young people, and the need to vaccinate with the Bexsero vaccine as part of the immunisation schedule as well as MenQuadfi for high-risk groups.
Una Ren, Senior Scientist in Genomics, New Zealand Institute for Public Health and Forensic Science; Nigel French, Distinguished Professor of Infectious Disease Epidemiology and Public Health, Te Kunenga ki Pūrehuroa – Massey University, and Sarah Hannah, Doctoral Candidate in Epidemiology, Te Kunenga ki Pūrehuroa – Massey University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Cocoa vs Biological Aging!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You probably know that chocolate is full of antioxidants, especially flavonoids.
You may well remember: Enjoy Bitter Foods For Your Heart & Brain and, for that matter, Are You Getting The Right Kinds Of Flavonoids?
You probably also know that biological aging (of various kinds) is largely driven by inflammation, which those antioxidants fight.
So, to what degree is the logical conclusion “chocolate is healthy” wishful thinking, and to what degree is it actually as good as it sounds?
Let’s spill the beans
We have written about chocolate before, and its health benefits/myths.
See for example: Chocolate & Health ← one of our earliest mythbusting editions!
And, for that matter: The Truth About Chocolate & Skin Health (which we hadn’t covered previously at the time)
We’ve also tackled chocolate and mental health considerations; see: 12 Foods That Fight Depression & Anxiety and The “Love Drug” ← this one is about phenylethylamine (PEA), an amphetamine-like substance found in chocolate, amongst other sources!
In this latest study, researchers (Dr. Sidong Li et al.) tested cocoa extract supplements in 21,442 adults over 60 as part of the COSMOS trial, focusing on their effect on markers of “inflammaging” (chronic low-grade inflammation linked to aging and cardiovascular disease).
Unlike many studies with such huge participant numbers, this wasn’t an observational study, but actually a huge randomized placebo-controlled trial.
Dr. Li and her team found that daily cocoa extract reduced hsCRP (a key inflammation marker tied to heart disease) by about 8.4% per year compared with placebo, suggesting anti-inflammatory and cardio-protective effects, and also noted that this cocoa extract supplementation reduced cardiovascular mortality by 27%.
So, that’s huge. It’s still not a panacea, though; some other markers (IL-6, TNF-α, IL-10) showed little change overall, though IL-6 decreased slightly in women, while interferon-γ increased, raising new research questions that Dr. Li and her team are eager to explore.
In few words: this very large amount of data, when all’s said and done, supports the value of plant-based, flavanol-rich foods like cocoa, as well as berries, grapes, and tea, in promoting cardiovascular health and reducing inflammatory aging.
You can see the paper itself out in the wild, here: Effects of 2-year cocoa extract supplementation on inflammaging biomarkers in older US adults: findings from the Cocoa Supplement and Multivitamin Outcomes Study randomised clinical trial
Notably, what it does not say is that we should eat chocolate as it is most commonly sold, that is to say, with an astonishing amount of added sugar (which is, obviously, best avoided).
See also: 10 “Healthy” Foods That Are Often Worse Than You Think
Want to get chocolatey?
If you’d like to stock up on cocoa extract supplements, then here’s an example product on Amazon 😎
If you’d like to get the benefits the more traditional way, then here are some chocolate-rich recipes that are actually healthy:
Anti-Inflammatory Brownies | Loaded Mocha Chocolate Parfait 😋
Enjoy!
Share This Post



Related Posts
-

The Light Doctor – by Dr. Martin Moore-Ede
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We (health-conscious people, at least) tend to think a lot about what we eat, what we drink, how we exercise, how we sleep, maybe even what kind of air we breathe.
It’s less common to think much about what kind of light we see, beyond perhaps a general idea that when it is bedtime, maybe the bright screen with all the information in the world (and also everyone we know) is not what will lull us peacefully to sleep.
Dr. Moore-Ede was a surgeon who, after letting a retractor slip during surgery after a year of 36-hour shifts, hung up his MD life and went back to Harvard to do a PhD on the topic of the woes of circadian rhythm disruption.
40 years later, he’s become one of the world’s leading figures in that field (perhaps we could say “luminary”?) and in this book, he brings to us the distilled essence of that learning in its most practical form.
One of the biggest problems, he argues, is lighting that has been optimized for cheapness of production, rather than for health. His preferred solution is (expensive!) lighting that switches between blue-rich white light during the day, to blue-depleted light in the evening, but for those not springing for that, there are sensible workarounds, he does give us the rundown of various kinds of lighting, since not every “energy-efficient lightbulb” is the same technology, and some are much better/worse for general health than others, in various ways, which he describes in detail.
The style is a little sensationalist for this reviewer’s tastes, but informationally there’s a lot in here to make it worthwhile, and as you might expect, there’s a lot of science and a reassuringly extensive bibliography.
Bottom line: this book will help guide you through kitting out your life with lighting that will promote good health rather than drain it.
Click here to check out The Light Doctor, and see your life in a different light!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Four Thousand Weeks – by Oliver Burkeman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is not, strictly speaking, a time management book. It’s more a “contemplating mortality and making things count while still doing the necessaries”.
Burkeman’s premise is that we get around 4,000 weeks of life, on average. If we live to 120, it’s more like 6,200. Unlucky souls may have to do the best they can with 1,000 or so.
The book is thought-provoking; consider:
- how was your last week?
- how will your next week be?
- what if it were your last?
Of course, we cannot necessarily liquidate all our assets and spend next week burning out in style, because then the following week comes. So, what’s the solution?
That’s something Burkeman lays out over the course of the book, with key ideas including passion projects and figuring out what can be safely neglected, but there’s far more there than we could sum up here.
Bottom line: if you ever find yourself struggling to balance what is expected of you with what is of value to you, this book can help you get the most out of your choices.
Click here to check out Four Thousand Weeks, and make yours count!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Blueberries vs Papaya – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing blueberries to papaya, we picked the blueberries.
Why?
In terms of macros, blueberries have rather more fiber, carbs, and for what it’s worth (which isn’t much) protein, making them the more nutritionally-dense option in this category.
In the category of vitamins, blueberries have more of vitamins B1, B2, B3, B6, E, and K, while papaya has more of vitamins A, B5, B9, and C, giving blueberries a 6:4 win here.
Looking at minerals, blueberries have more copper, iron, manganese, phosphorus, and zinc, while papaya has more calcium, magnesium, potassium, and selenium, yielding a more marginal 5:4 victory to blueberries in this round.
In other considerations, blueberries have a much higher polyphenol content, living up to their superfood reputation in this regard, so that’s another point in their favor.
Adding up the sections makes for a total win for blueberries, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: