Recent outbreaks highlight the risks of bacterial meningitis and the need to vaccinate
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Outbreaks of bacterial meningococcal disease in England and recent cases in students in New Zealand have raised awareness of this serious and life-threatening disease.
The disease is caused by the bacterium Neisseria meningitidis and presents as meningitis or blood poisoning (septicaemia).
Meningitis is an inflammation of the membranes that cover the brain and spinal cord (meninges), while septicaemia affects the whole body through the presence of bacteria in the blood stream.
Both can be also be caused by other infectious agents, but bacterial meningococcal disease is the most severe form.
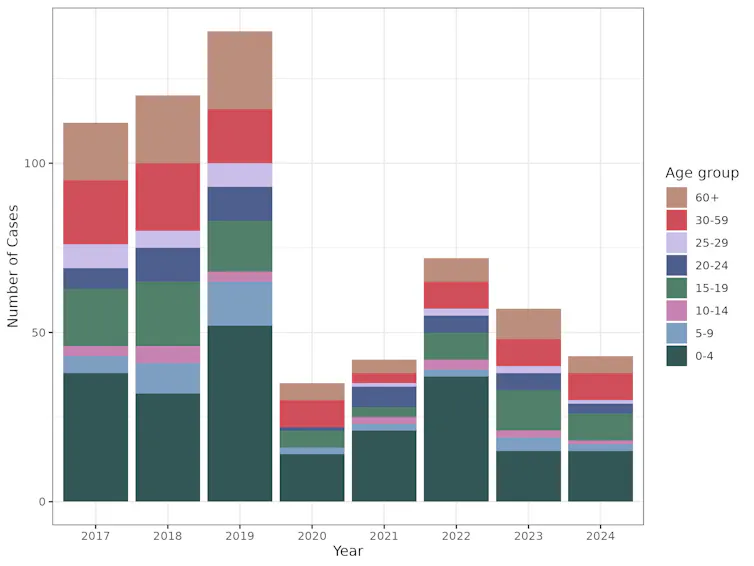
Infants, children and young adults are at higher risk. While the disease is largely preventable through vaccination, only one vaccine is currently on the national immunisation schedule in Aotearoa New Zealand.
As part of ongoing research to explain the recent cases, we compared the meningococcal strains involved in both countries and explored the significance of people who carry the bacterium but don’t develop symptoms or disease.
There are several strains of Neisseria meningitidis and most belong to six groups (named A, B, C, W, X and Y). All have an extraordinary ability to swap genetic material between them and switch genes on and off through a process known as phase variation.
This can change the surface of the bacterium, enabling it to escape the body’s immune system.
The strains responsible for both the UK and recent Dunedin cases belong to Group B meningococci. However, the similarity ends there. The UK outbreak strain is known as ST485, while the Dunedin cases were caused by different strains. They differ from the UK strain as well as from each other, suggesting more than one chain of transmission was involved.
The Bexsero vaccine is used to protect people against bacterial meningitis caused by group B strains. It was designed to recognise components in the outer membrane and on the surface of the bacteria.
The strain that caused the UK outbreak is likely covered by the Bexero vaccine because it matches exactly one of the protein antigen sequences used in the vaccine.
But genomic sequencing of the bacteria responsible for one of the Dunedin cases is still pending, while the other case did not yield a bacterial culture.

The importance of genome sequencing
Although meningococcal disease can appear as scattered and apparently unrelated cases, these can occasionally build into larger outbreaks.
Strain typing and genome sequencing can help to determine if an apparent outbreak is due to the emergence of a particular strain or a cluster of cases that are genetically unrelated.
Both scenarios can occur if cases share a common risk factor, such as increased close contact and mixing in educational settings such as schools and universities.
Past genomic surveillance in New Zealand has shown the emergence of outbreak strains and helped identify likely resistance to antibiotics. For example, a W group strain variant caused rising numbers of meningococcal disease between 2016 and 2019 in New Zealand and an outbreak in Northland in 2018.
Genome sequencing showed this strain was different from the W strain causing disease in Europe at the time, and the specific 2015 variant also has increased resistance to penicillin.
Healthy people can be carriers
Despite its ability to cause severe disease, the bacterium causing meningococcal disease is often found in people’s throat, without causing symptoms.
About 5% to 30% of the global population are carriers, and most don’t experience any symptoms or disease. We don’t yet fully understand the factors that determine whether disease develops.
Genome sequencing has shown that some highly virulent strains which are associated with outbreaks are rarely identified in samples from healthy carriers. But as yet, attempts to find genomic explanations for differences in bacteria found in outbreaks and healthy carriers remain inconclusive.
The likelihood whether people carry the bacterium is age dependent. It is low in younger children and older people, but high in teenagers and young adults.
The high carriage rate in young adults makes university students a high-risk group for developing the disease. Crowded living conditions also contribute to the high carriage rate, exacerbating the risk.
In New Zealand, both the Bexsero (against group B) and MenQuadfi (against ACWY) vaccines are available to young people moving into boarding school or university halls the first time. In contrast, only one vaccine (against ACWY) is currently funded for university students in England.
Both vaccines are needed to have maximum protection. Conjugate ACWY vaccines may reduce carriage and therefore transmission. Bexsero does not reduce carriage but protects against development of the disease.
Impact of COVID measures on transmission
Lockdowns and border controls introduced during the COVID pandemic reduced transmission of the SARS-CoV2 virus. But they also had a major effect on other diseases, including influenza and other respiratory viruses.
Cases of meningococcal disease were also dramatically reduced during the COVID response, most likely due to reduced contact between individuals and because fewer infected people entered the country.
The rebound in cases following relaxation of these strict measures was expected.
This highlights how important it is to be aware of the risks associated with large gatherings, particularly of young people, and the need to vaccinate with the Bexsero vaccine as part of the immunisation schedule as well as MenQuadfi for high-risk groups.
Una Ren, Senior Scientist in Genomics, New Zealand Institute for Public Health and Forensic Science; Nigel French, Distinguished Professor of Infectious Disease Epidemiology and Public Health, Te Kunenga ki Pūrehuroa – Massey University, and Sarah Hannah, Doctoral Candidate in Epidemiology, Te Kunenga ki Pūrehuroa – Massey University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Topping Up Testosterone?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Testosterone Drop
Testosterone levels decline amongst men over a certain age. Exactly when depends on the individual and also how we measure it, but the age of 45 is a commonly-given waypoint for the start of this decline.
(the actual start is usually more like 20, but it’s a very small decline then, and speeds up a couple of decades later)
This has been called “the male menopause”, or “the andropause”.
Both terms are a little misleading, but for lack of a better term, “andropause” is perhaps not terrible.
Why “the male menopause” is misleading:
To call it “the male menopause” suggests that this is when men’s menstruation stops. Which for cis men at the very least, is simply not a thing they ever had in the first place, to stop (and for trans men it’s complicated, depending on age, hormones, surgeries, etc).
Why “the andropause” is misleading:
It’s not a pause, and unlike the menopause, it’s not even a stop. It’s just a decline. It’s more of an andro-pitter-patter-puttering-petering-out.
Is there a better clinical term?
Objectively, there is “late-onset hypogonadism” but that is unlikely to be taken up for cultural reasons—people stigmatize what they see as a loss of virility.
Terms aside, what are the symptoms?
❝Andropause or late-onset hypogonadism is a common disorder which increases in prevalence with advancing age. Diagnosis of late-onset of hypogonadism is based on presence of symptoms suggestive of testosterone deficiency – prominent among them are sexual symptoms like…❞
…and there we’d like to continue the quotation, but if we list the symptoms here, it won’t get past a lot of filters because of the words used. So instead, please feel free to click through:
Source: Andropause: Current concepts
Can it be safely ignored?
If you don’t mind the sexual symptoms, then mostly, yes!
However, there are a few symptoms we can mention here that are not so subjective in their potential for harm:
- Depression
- Loss of muscle mass
- Increased body fat
Depression kills, so this does need to be taken seriously. See also:
The Mental Health First-Aid That You’ll Hopefully Never Need
(the above is a guide to managing depression, in yourself or a loved one)
Loss of muscle mass means being less robust against knocks and falls later in life
Loss of muscle mass also means weaker bones (because the body won’t make bones stronger than it thinks they need to be, so bone will follow muscle in this regard—in either direction)
See also:
- Resistance Is Useful! (Especially As We Get Older)
- Protein vs Sarcopenia
- Fall Special (How to Proof Yourself Against Falls)
Increased body fat means increased risk of diabetes and heart disease, as a general rule of thumb, amongst other problems.
Will testosterone therapy help?
That’s something to discuss with your endocrinologist, but for most men whose testosterone levels are lower than is ideal for them, then yes, taking testosterone to bring them [back] to “normal” levels can make you happier and healthier (though it’s certainly not a cure-all).
See for example:
Testosterone Therapy Improves […] and […] in Hypogonadal Men
(Sorry, we’re not trying to be clickbaity, there are just some words we can’t use without encountering software problems)
Here’s a more comprehensive study that looked at 790 men aged 65 or older, with testosterone levels below a certain level. It looked at the things we can’t mention here, as well as physical function and general vitality:
❝The increase in testosterone levels was associated with significantly increased […] activity, as assessed by the Psychosexual Daily Questionnaire (P<0.001), as well as significantly increased […] desire and […] function.
The percentage of men who had an increase of at least 50 m in the 6-minute walking distance did not differ significantly between the two study groups in the Physical Function Trial but did differ significantly when men in all three trials were included (20.5% of men who received testosterone vs. 12.6% of men who received placebo, P=0.003).
Testosterone had no significant benefit with respect to vitality, as assessed by the Functional Assessment of Chronic Illness Therapy–Fatigue scale, but men who received testosterone reported slightly better mood and lower severity of depressive symptoms than those who received placebo❞
Source: Effects of Testosterone Treatment in Older Men
We strongly recommend, by the way, when a topic is of interest to you to read the paper itself, because even the extract above contains some subjectivity, for example what is “slightly better”, and what is “no significant benefit”.
That “slightly better mood and lower severity of depressive symptoms”, for example, has a P value of 0.004 in their data, which is an order of magnitude more significant than the usual baseline for significance (P<0.05).
And furthermore, that “no significant benefit with respect to vitality” is only looking at either the primary outcome aggregated goal or the secondary FACIT score whose secondary outcome had a P value of 0.06, which just missed the cut-off for significance, and neglects to mention that all the other secondary outcome metrics for men involved in the vitality trial were very significant (ranging from P=0.04 to P=0.001)
Click here to see the results table for the vitality trial
Will it turn me into a musclebound angry ragey ‘roidmonster?
Were you that kind of person before your testosterone levels declined? If not, then no.
Testosterone therapy seeks only to return your testosterone levels to where they were, and this is done through careful monitoring and adjustment. It’d take a lot more than (responsible) endocrinologist-guided hormonal therapy to turn you into Marvel’s “Wolverine”.
Is testosterone therapy safe?
A question to take to your endocrinologist because everyone’s physiology is different, but a lot of studies do support its general safety for most people who are prescribed it.
As with anything, there are risks to be aware of, though. Perhaps the most critical risk is prostate cancer, and…
❝In a large meta-analysis of 18 prospective studies that included over 3500 men, there was no association between serum androgen levels and the risk of prostate cancer development
For men with untreated prostate cancer on active surveillance, TRT remains controversial. However, several studies have shown that TRT is not associated with progression of prostate cancer as evidenced by either PSA progression or gleason grade upstaging on repeat biopsy.
Men on TRT should have frequent PSA monitoring; any major change in PSA (>1 ng/mL) within the first 3-6 months may reflect the presence of a pre-existing cancer and warrants cessation of therapy❞
Those are some select extracts, but any of this may apply to you or your loved one, we recommend to read in full about this and other risks:
Risks of testosterone replacement therapy in men
See also: Prostate Health: What You Should Know
Beyond that… If you are prone to baldness, then taking testosterone will increase that tendency. If that’s a problem for you, then it’s something to know about. There are other things you can take/use for that in turn, so maybe we’ll do a feature on those one of these days!
For now, take care!
Share This Post
-

How to host a meal if one of your guests has an eating disorder or is anxious around food
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As the festive season approaches, perhaps you’re thinking of hosting friends and family.
You know at least one person who’ll attend who becomes anxious around food and another with an eating disorder.
So, how to host and make sure everyone feels comfortable and supported?
Perhaps you’ve already hosted someone with food anxiety or an eating disorder without even knowing.

fauxels/Pexels First, some definitions
Food anxiety refers to fear or anxiety in response to eating food. This could relate to certain textures and smells, or fear of choking or vomiting. These fears and anxieties can be intense and are associated with mental health conditions, including avoidant/restrictive food intake disorder.
For others, anxiety about food might be based on fear of the impact food could have on their body shape and size. This kind of food anxiety is closely associated with diagnosable eating disorders such as anorexia nervosa and bulimia nervosa.
Eating disorders are among the most rapidly increasing mental health diagnoses in the world, and can be present at any shape or size. These disorders involve negative thoughts about one’s weight, shape and eating. Behaviours people can experience include skipping meals, or feeling like they can’t stop eating.
Eating disorders can have significant impacts on someone’s life, including withdrawing from social circles and hobbies. They’re associated with high mortality rates.
Just because someone experiences some food anxiety, it does not mean they have a mental health diagnosis. It’s also important to consider how this anxiety impacts their life and the level of distress it causes them.
Hiding is common
It’s likely you’ve shared a meal with someone who has an eating disorder, who might be in recovery, or has anxiety around food. A lot of the time, you may not be able to tell, and they might try to hide it because of shame or guilt.
Your nephew at last week’s family barbecue might have binge eating disorder. The cousin who you caught up with for dinner might have a fear of choking and only eats soft foods.
You might not have noticed as people tend to be skilled at hiding their food anxiety. Some common strategies include avoiding shared mealtimes, only choosing certain foods, or saying they have already eaten and aren’t hungry.
So, if you’ll likely share a meal with someone with food anxiety or an eating disorder in the future, how can you host compassionately?
Is it worth adjusting the menu?
Unless someone has made specific requests, it is OK to roll on as usual. It can be helpful to invite guests to bring anything that meets their specific needs. Having variety and allowing people to serve themselves may also reduce food anxiety.
The goal of this meal is not to solve someone’s food anxiety, but to create a safe eating environment for all.
What not to say
At mealtimes, it might be common to comment on the amount or type of food someone is eating, or the way they eat it.
This “food talk” might be comments such as, “why are you only eating potatoes?” These comments can draw unwanted attention to someone’s food choices, increasing food anxiety.
Then there are comments on people’s bodies, shapes and sizes. Or sometimes people comment on the need to diet or skip meals after eating.
For example, people might say “that was so much food, you won’t need dinner tonight”.
While some of these comments may not be intended to hurt, these attitudes often perpetuate harmful messages about what we should and should not eat, how much we should eat, and even how we should look.
These comments can even contribute to body dissatisfaction, a key risk factor in developing eating disorders. Negative food and body talk can also contribute to increased anxiety.
Even commenting on your own eating and body can be a problem. For instance saying, “I need to skip dinner to make up for eating all this” might hurt the people you’re sharing a meal with, particularly if they have an eating disorder. This is because it reinforces and normalises food restriction.
A good rule of thumb is to avoid commenting on people’s food and bodies. And that goes for complimenting someone’s body.
What to say instead
As a guest or a host, you can contribute to developing a safe culture around food for everyone. This includes replying to unsolicited food or body comments, whether aimed at you or someone else.
Sometimes replying can be tricky for the person with a food anxiety or eating disorder, so you can also speak up even when the comment isn’t directed at you.
You can say:
- Would it be OK if we didn’t chat about my/their food/weight/body at the moment?
- I’m working hard to focus less on my body at the moment. Let’s talk about something else.
- I find it uncomfortable when you mention my/my friend’s weight/body/eating.
- I hear what you’re saying, but let’s steer clear from discussing my/their appearance/weight/eating.
Some of these suggestions might sound awkward, so offer them gently and personalise however you need.
Why this is important
Ultimately, setting boundaries with family and friends helps create more balance and compassion in how we talk about food and bodies. This can challenge some of the outdated and harmful messages that have become normalised.
Sharing mealtimes are important opportunities to connect with loved ones. Let’s make these experiences safe and inclusive.
If this article raised any concerns for you or someone you know, contact the Butterfly Foundation on 1800 33 4673.
Kathleen de Boer, Clinical Psychologist, Lecturer in Clinical Psychology, Swinburne University of Technology; Courtney P. McLean, Research Fellow, School of Psychological Sciences, Monash University, and Inge Gnatt, Psychologist, Lecturer in Psychology, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Younger You – by Kara Fitzgerald
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, a note about the author: she is a naturopathic doctor, a qualification not recognized in most places. Nevertheless, she clearly knows a lot of stuff, and indeed has been the lead research scientist on a couple of studies, one of which was testing the protocol that would later go into this book.
Arguably, there’s a conflict of interest there, but it’s been peer reviewed and the science seems perfectly respectable. After an 8-week interventional trial, subjects enjoyed a reversal of DNA methylation (one of various possible markers of biological aging) comparable to being 3 years younger.
Where the value of this book lies is in optimizing one’s diet in positive fashion. In other words, what to include rather than what to exclude, but the “include” list is quite extensive so you’re probably not going to be reaching for a donut by the time you’ve eaten all that. In particular, she’s optimized the shopping list for ingredients that contain her DNA methylation superstars most abundantly; those nutrients being: betaine choline, curcumin, epigallocatechin gallate, quercetin, rosmarinic acid, and vitamins B9 and B12.
To make this possible, she sets out not just shopping list but also meal plans, and challenges the reader to do an 8-week intervention of our own.
Downside: it is quite exacting if you want to follow it 100%.
Bottom line: this is a very informative, science-based book. It can make you biologically younger at least by DNA methylation standards, if the rather specific diet isn’t too onerous for you.
Click here to check out Younger You, and enjoy a younger you!
Share This Post


-
What Flexible Dieting Really Means
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Flexibility Is The Dish Of The Day

This is Alan Aragon. Notwithstanding not being a “Dr. Alan Aragon”, he’s a research scientist with dozens of peer-reviewed nutrition science papers to his name, as well as being a personal trainer and fitness educator. Most importantly, he’s an ardent champion of making people’s pursuit of health and fitness more evidence-based.
We’ll be sharing some insights from a book of his that we haven’t reviewed yet, but we will link it at the bottom of today’s article in any case.
What does he want us to know?
First, get out of the 80s and into the 90s
In the world of popular dieting, the 80s were all about calorie-counting and low-fat diets. They did not particularly help.
In the 90s, it was discovered that not only was low-fat not the way to go, but also, regardless of the diet in question, rigid dieting leads to “disinhibition”, that is to say, there comes a point (usually not far into a diet) whereby one breaks the diet, at which point, the floodgates open and the dieter binges unhealthily.
Aragon would like to bring our attention to a number of studies that found this in various ways over the course of the 90s measuring various different metrics including rigid vs flexible dieting’s impacts on BMI, weight gain, weight loss, lean muscle mass changes, binge-eating, anxiety, depression, and so forth), but we only have so much room here, so here’s a 1999 study that’s pretty much the culmination of those:
Flexible vs. Rigid Dieting Strategies: Relationship with Adverse Behavioral Outcomes
So in short: trying to be very puritan about any aspect of dieting will not only not work, it will backfire.
Next, get out of the 90s into the 00s
…which is not only fun if you read “00s” out loud as “naughties”, but also actually appropriate in this case, because it is indeed important to be comfortable being a little bit naughty:
In 2000, Dr. Marika Tiggemann found that dichotomous perceptions of food (e.g. good/bad, clean/dirty, etc) were implicated as a dysfunctional cognitive style, and predicted not only eating disorders and mood disorders, but also adverse physical health outcomes:
Dieting and Cognitive Style: The Role of Current and Past Dieting Behaviour and Cognitions
This was rendered clearer, in terms of physical health outcomes, by Dr. Susan Byrne & Dr. Emma Dove, in 2009:
❝Weight loss was negatively associated with pre-treatment depression and frequency of treatment attendance, but not with dichotomous thinking. Females who regard their weight as unacceptably high and who think dichotomously may experience high levels of depression irrespective of their actual weight, while depression may be proportionate to the degree of obesity among those who do not think dichotomously❞
Aragon’s advice based on all this: while yes, some foods are better than others, it’s more useful to see foods as being part of a spectrum, rather than being absolutist or “black and white” about it.
Next: hit those perfect 10s… Imperfectly
The next decade expanded on this research, as science is wont to do, and for this one, Aragon shines a spotlight on Dr. Alice Berg’s 2018 study with obese women averaging 69 years of age, in which…
In other words (and in fact, to borrow Dr. Berg’s words from that paper),
❝encouraging a flexible approach to eating behavior and discouraging rigid adherence to a diet may lead to better intentional weight loss for overweight and obese older women❞
You may be wondering: what did this add to the studies from the 90s?
And the key here is: rather than being observational, this was interventional. In other words, rather than simply observing what happened to people who thought one way or another, this study took people who had a rigid, dichotomous approach to food, and gave them a 6-month behavioral intervention (in other words, support encouraging them to be more flexible and open in their approach to food), and found that this indeed improved matters for them.
Which means, it’s not a matter of fate or predisposition, as it could have been back in the 90s, per “some people are just like that; who’s to say which factor causes which”. Instead, now we know that this is an approach that can be adopted, and it can be expected to work.
Beyond weight loss
Now, so far we’ve talked mostly about weight loss, and only touched on other health outcomes. This is because:
- weight loss a very common goal for many
- it’s easy to measure so there’s a lot of science for it
Incidentally, if it’s a goal of yours, here’s what 10almonds had to say about that, along with two follow-up articles for other related goals:
Spoiler: we agree with Aragon, and recommend a relaxed and flexible approach to all three of these things
Aragon’s evidence-based approach to nutrition has found that this holds true for other aspects of healthy eating, too. For example…
To count or not to count?
It’s hard to do evidence-based anything without counting, and so Aragon talks a lot about this. Indeed, he does a lot of counting in scientific papers of his own, such as:
and
The effect of protein timing on muscle strength and hypertrophy: a meta-analysis
…as well as non-protein-related but diet-related topics such as:
But! For the at-home health enthusiast, Aragon recommends that the answer to the question “to count or not to count?” is “both”:
- Start off by indeed counting and tracking everything that is important to you (per whatever your current personal health intervention is, so it might be about calories, or grams of protein, or grams of carbs, or a certain fat balance, or something else entirely)
- Switch to a more relaxed counting approach once you get used to the above. By now you probably know the macros for a lot of your common meals, snacks, etc, and can tally them in your head without worrying about weighing portions and knowing the exact figures.
- Alternatively, count moderately standardized portions of relevant foods, such as “three servings of beans or legumes per day” or “no more than one portion of refined carbohydrates per day”
- Eventually, let habit take the wheel. Assuming you have established good dietary habits, this will now do you just fine.
This latter is the point whereby the advice (that Aragon also champions) of “allow yourself an unhealthy indulgence of 10–20% of your daily food”, as a budget of “discretionary calories”, eventually becomes redundant—because chances are, you’re no longer craving that donut, and at a certain point, eating foods far outside the range of healthiness you usually eat is not even something that you would feel inclined to do if offered.
But until that kicks in, allow yourself that budget of whatever unhealthy thing you enjoy, and (this next part is important…) do enjoy it.
Because it is no good whatsoever eating that cream-filled chocolate croissant and then feeling guilty about it; that’s the dichotomous thinking we had back in the 80s. Decide in advance you’re going to eat and enjoy it, then eat and enjoy it, then look back on it with a sense of “that was enjoyable” and move on.
The flipside of this is that the importance of allowing oneself a “little treat” is that doing so actively helps ensure that the “little treat” remains “little”. Without giving oneself permission, then suddenly, “well, since I broke my diet, I might as well throw the whole thing out the window and try again on Monday”.
On enjoying food fully, by the way:
Mindful Eating: How To Get More Nutrition Out Of The Same Food
Want to know more from Alan Aragon?
Today we’ve been working heavily from this book of his; we haven’t reviewed it yet, but we do recommend checking it out:
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Tahini vs Hummus – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing tahini to hummus, we picked the tahini.
Why?
Both are great! But tahini is so nutritionally dense, that it makes even the wonder food that is hummus look bad next to it.
In terms of macros, tahini is higher in everything except water. So, higher in protein, carbs, fats, and fiber. In terms of those fats, the fat breakdown is similar for both, being mostly polyunsaturated and monounsaturated, with a small percentage of saturated. Tahini has the lower glycemic index, but both are so low that it makes no practical difference.
In terms of vitamins, tahini has more of vitamins A, B1, B2, B3, B5, B9, E, and choline, while hummus is higher in vitamin B6.
This is a good reason to embellish hummus with some red pepper (vitamin A), a dash of lemon (vitamin C), etc, but we’re judging these foods in their most simple states, for fairness.
When it comes to minerals, tahini has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Meanwhile, hummus is higher in sodium.
Note: hummus is a good source of all those minerals too! Tahini just has more.
In short… Enjoy both, but tahini is the more nutritionally dense by far. On the other hand, if for whatever reason you’re looking for something lower in carbs, fats, and calories, then hummus is where it’s at.
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Could not getting enough sleep increase your risk of type 2 diabetes?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Not getting enough sleep is a common affliction in the modern age. If you don’t always get as many hours of shut-eye as you’d like, perhaps you were concerned by news of a recent study that found people who sleep less than six hours a night are at higher risk of type 2 diabetes.
So what can we make of these findings? It turns out the relationship between sleep and diabetes is complex.
The study
Researchers analysed data from the UK Biobank, a large biomedical database which serves as a global resource for health and medical research. They looked at information from 247,867 adults, following their health outcomes for more than a decade.
The researchers wanted to understand the associations between sleep duration and type 2 diabetes, and whether a healthy diet reduced the effects of short sleep on diabetes risk.
As part of their involvement in the UK Biobank, participants had been asked roughly how much sleep they get in 24 hours. Seven to eight hours was the average and considered normal sleep. Short sleep duration was broken up into three categories: mild (six hours), moderate (five hours) and extreme (three to four hours). The researchers analysed sleep data alongside information about people’s diets.
Some 3.2% of participants were diagnosed with type 2 diabetes during the follow-up period. Although healthy eating habits were associated with a lower overall risk of diabetes, when people ate healthily but slept less than six hours a day, their risk of type 2 diabetes increased compared to people in the normal sleep category.
The researchers found sleep duration of five hours was linked with a 16% higher risk of developing type 2 diabetes, while the risk for people who slept three to four hours was 41% higher, compared to people who slept seven to eight hours.
One limitation is the study defined a healthy diet based on the number of servings of fruit, vegetables, red meat and fish a person consumed over a day or a week. In doing so, it didn’t consider how dietary patterns such as time-restricted eating or the Mediterranean diet may modify the risk of diabetes among those who slept less.
Also, information on participants’ sleep quantity and diet was only captured at recruitment and may have changed over the course of the study. The authors acknowledge these limitations.
Why might short sleep increase diabetes risk?
In people with type 2 diabetes, the body becomes resistant to the effects of a hormone called insulin, and slowly loses the capacity to produce enough of it in the pancreas. Insulin is important because it regulates glucose (sugar) in our blood that comes from the food we eat by helping move it to cells throughout the body.
We don’t know the precise reasons why people who sleep less may be at higher risk of type 2 diabetes. But previous research has shown sleep-deprived people often have increased inflammatory markers and free fatty acids in their blood, which impair insulin sensitivity, leading to insulin resistance. This means the body struggles to use insulin properly to regulate blood glucose levels, and therefore increases the risk of type 2 diabetes.
Further, people who don’t sleep enough, as well as people who sleep in irregular patterns (such as shift workers), experience disruptions to their body’s natural rhythm, known as the circadian rhythm.
This can interfere with the release of hormones like cortisol, glucagon and growth hormones. These hormones are released through the day to meet the body’s changing energy needs, and normally keep blood glucose levels nicely balanced. If they’re compromised, this may reduce the body’s ability to handle glucose as the day progresses.
These factors, and others, may contribute to the increased risk of type 2 diabetes seen among people sleeping less than six hours.
Millions of people around the world have diabetes. WESTOCK PRODUCTIONS/Shutterstock While this study primarily focused on people who sleep eight hours or less, it’s possible longer sleepers may also face an increased risk of type 2 diabetes.
Research has previously shown a U-shaped correlation between sleep duration and type 2 diabetes risk. A review of multiple studies found getting between seven to eight hours of sleep daily was associated with the lowest risk. When people got less than seven hours sleep, or more than eight hours, the risk began to increase.
The reason sleeping longer is associated with increased risk of type 2 diabetes may be linked to weight gain, which is also correlated with longer sleep. Likewise, people who don’t sleep enough are more likely to be overweight or obese.
Good sleep, healthy diet
Getting enough sleep is an important part of a healthy lifestyle and may reduce the risk of type 2 diabetes.
Based on this study and other evidence, it seems that when it comes to diabetes risk, seven to eight hours of sleep may be the sweet spot. However, other factors could influence the relationship between sleep duration and diabetes risk, such as individual differences in sleep quality and lifestyle.
While this study’s findings question whether a healthy diet can mitigate the effects of a lack of sleep on diabetes risk, a wide range of evidence points to the benefits of healthy eating for overall health.
The authors of the study acknowledge it’s not always possible to get enough sleep, and suggest doing high-intensity interval exercise during the day may offset some of the potential effects of short sleep on diabetes risk.
In fact, exercise at any intensity can improve blood glucose levels.
Giuliana Murfet, Casual Academic, Faculty of Health, University of Technology Sydney and ShanShan Lin, Senior Lecturer, School of Public Health, University of Technology Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: