

Ozempic Helps People Walk Further
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There’s often a catch-22 when it comes to exercise: it’s important for good health, and/but people with ill health usually cannot exercise much.
A recent (published today, at time of writing, the 29th of March 2025, never let it be said we don’t bring you the very most up-to-date health science!) study by Dr. Neda Rasouli et al. has shown there is a possible way through that catch-22, depending on the nature of the illness.
This study followed 792 people across 112 outpatient clinical trial sites in 20 countries in North America, Asia, and Europe, with type 2 diabetes and peripheral artery disease.
What they found
Patients taking semaglutide (specifically, 1mg Ozempic) enjoyed a 21% median increase in walking distance, as well as some bonus benefits, namely:
- Weight reduction: the semaglutide group saw a greater reduction in body weight (–4.1 kg; P < 0 .0001)
- HbA1c levels: semaglutide lowered HbA1c by 1 percentage point (P < 0.0001)
- Blood pressure: systolic blood pressure decreased by 3.2 mmHg (P = 0.0042)
You may be wondering what that “P =” means: it’s the probability of this occurring by random chance, on a scale from zero (impossible outcome) to 1 (unavoidable outcome).
For example:
“We hypothesized that singing the happy birthday song before tossing a coin would result in it landing on heads. We sang the happy birthday song and tossed the coin; it landed on heads (P = 0.5)”
In science, generally speaking anything with a probability of under 0.05 (expressed as: “P < 0.05”) is considered a statistically significant result.
All this to say, the cited figures of, for example, P < 0.0001, are very significant indeed.
On which note, that 21% median increase in walking distance? P < 0.0004.
As for side effects? Serious adverse events related to the drug occurred in 1% of the semaglutide group vs 2% in the placebo group. So, that seems quite safe indeed.
You can find the paper itself here:
Want to learn more?
Check out:
- The Doctor Who Wants Us To Exercise Less, & Move More
- Walking… Better.
- 5 Ways To Naturally Boost The “Ozempic Effect”
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Our blood-brain barrier stops bugs and toxins getting to our brain. Here’s how it works

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
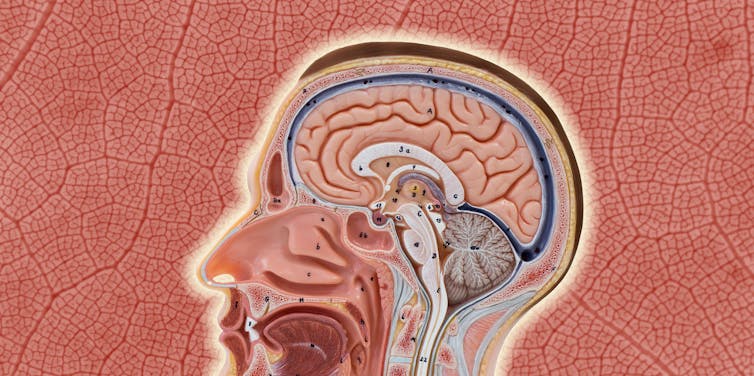
Our brain is an extremely complex and delicate organ. Our body fiercely protects it by holding onto things that help it and keeping harmful things out, such as bugs that can cause infection and toxins.
It does that though a protective layer called the blood-brain barrier. Here’s how it works, and what it means for drug design.

The Conversation, Rattiya Thongdumhyu/Shutterstock, Petr Ganaj/Pexels First, let’s look at the circulatory system
Adults have roughly 30 trillion cells in their body. Every cell needs a variety of nutrients and oxygen, and they produce waste, which needs to be taken away.
Our circulatory system provides this service, delivering nutrients and removing waste.
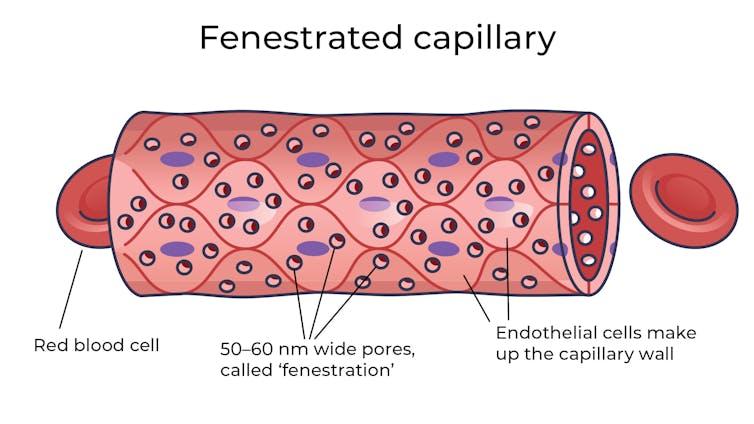
Fenestrated capillaries let nutrients and waste pass through. Vectormine/Shutterstock Where the circulatory system meets your cells, it branches down to tiny tubes called capillaries. These tiny tubes, about one-tenth the width of a human hair, are also made of cells.
But in most capillaries, there are some special features (known as fenestrations) that allow relatively free exchange of nutrients and waste between the blood and the cells of your tissues.
It’s kind of like pizza delivery
One way to think about the way the circulation works is like a pizza delivery person in a big city. On the really big roads (vessels) there are walls and you can’t walk up to the door of the house and pass someone the pizza.
But once you get down to the little suburban streets (capillaries), the design of the streets means you can stop, get off your scooter and walk up to the door to deliver the pizza (nutrients).
We often think of the brain as a spongy mass without much blood in it. In reality, the average brain has about 600 kilometres of blood vessels.
The difference between the capillaries in most of the brain and those elsewhere is that these capillaries are made of specialised cells that are very tightly joined together and limit the free exchange of anything dissolved in your blood. These are sometimes called continuous capillaries.
Continuous capillaries limit the free exchange of anything dissolved in your blood. Vectormine/Shutterstock This is the blood brain barrier. It’s not so much a bag around your brain stopping things from getting in and out but more like walls on all the streets, even the very small ones.
The only way pizza can get in is through special slots and these are just the right shape for the pizza box.
The blood brain barrier is set up so there are specialised transporters (like pizza box slots) for all the required nutrients. So mostly, the only things that can get in are things that there are transporters for or things that look very similar (on a molecular scale).
The analogy does fall down a little bit because the pizza box slot applies to nutrients that dissolve in water. Things that are highly soluble in fat can often bypass the slots in the wall.
Why do we have a blood-brain barrier?
The blood brain barrier is thought to exist for a few reasons.
First, it protects the brain from toxins you might eat (think chemicals that plants make) and viruses that often can infect the rest of your body but usually don’t make it to your brain.
It also provides protection by tightly regulating the movement of nutrients and waste in and out, providing a more stable environment than in the rest of the body.
Lastly, it serves to regulate passage of immune cells, preventing unnecessary inflammation which could damage cells in the brain.
What it means for medicines
One consequence of this tight regulation across the blood brain barrier is that if you want a medicine that gets to the brain, you need to consider how it will get in.
There are a few approaches. Highly fat-soluble molecules can often pass into the brain, so you might design your drug so it is a bit greasy.
The blood-brain barrier stops many medicines getting into the brain. Ron Lach/Pexels Another option is to link your medicine to another molecule that is normally taken up into the brain so it can hitch a ride, or a “pro-drug”, which looks like a molecule that is normally transported.
Using it to our advantage
You can also take advantage of the blood brain barrier.
Opioids used for pain relief often cause constipation. They do this because their target (opioid receptors) are also present in the nervous system of the intestines, where they act to slow movement of the intestinal contents.
Imodium (Loperamide), which is used to treat diarrhoea, is actually an opioid, but it has been specifically designed so it can’t cross the blood brain barrier.
This design means it can act on opioid receptors in the gastrointestinal tract, slowing down the movement of contents, but does not act on brain opioid receptors.
In contrast to Imodium, Ozempic and Victoza (originally designed for type 2 diabetes, but now popular for weight-loss) both have a long fat attached, to improve the length of time they stay in the body.
A consequence of having this long fat attached is that they can cross the blood-brain barrier, where they act to suppress appetite. This is part of the reason they are so effective as weight-loss drugs.
So while the blood brain barrier is important for protecting the brain it presents both a challenge and an opportunity for development of new medicines.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

5 Proven Tips To Walk Longer Without Pain Or Discomfort
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Alyssa Kuhn, arthritis expert, explains how to reduce joint pain and improve mobility:
Be in tune with your body
There’s a step-by-step approach here:
- Warm up before walking: (caveat: only works if you actually do it!) because warming up your joints and muscles helps prevent stiffness, pain, and early fatigue. Do a few minutes of gentle movements such as:
- Forward and backward steps: step one foot forwards and backwards without pausing, about 10–20 times per side, to loosen your hips and improve blood flow.
- Side steps: step side to side 20–30 times to activate your outer hip muscles and stabilize your knees.
- Heel and toe raises: lift both your heels, then both sets of toes (you’re allowed to put your heels down in order to lift your toes!), to warm up your calves and shin muscles, 10–20 times total.
- Writer’s note: if you dance something like Salsa, you can get those all in very quickly and easily with a 2–3 minute song! You don’t even have to setenta complicado or anything, the basic step is fine 😉
- Activate your core: a strong core improves posture, balance, and walking confidence. So: stand with your back against a wall, feet slightly forwards. Flatten your lower back into the wall and raise one arm, then the other, without letting your back arch.
- Strengthen (generally) your other key muscles: muscle strength supports your joints and endurance. Prioritize squats, which can include chair squats—standing up and sitting down—because they work your thighs, glutes, and hamstrings.
- Increase your distance gradually: add only 1–2 minutes to your walk each time to help your body adapt and avoid flare-ups. This may seem impractical when walking often has a particular fixed destination in mind, but you can make your route slightly longer, or pace at home a little before setting out, that kind of thing.
- Listen to your body: pain, stiffness, or tightness are signals to modify your approach, not to push through. Pause or stretch briefly if discomfort arises. Recognize that your capacity may vary from day to day—especially with joint issues—so adapt accordingly to prevent setbacks and be content make steady progress in the big picture.
For more on all of this, including visual demonstrations of the exercises, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
How To Make Downhill Walking Easier On The Knees
Take care!
Share This Post
- Warm up before walking: (caveat: only works if you actually do it!) because warming up your joints and muscles helps prevent stiffness, pain, and early fatigue. Do a few minutes of gentle movements such as:
-

The “Love Drug”
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Get PEA-Brained!
Today we’ll be looking at phenylethylamine, or PEA, to its friends.
Not to be mistaken for the related amino acid phenylalanine! Both ultimately have effects on the dopaminergic system, but the process and benefits are mostly quite different.
We thought we’d do this one in the week of Valentine’s Day, because of its popular association with love:
❝Phenylethylamine (PEA), an amphetamine-like substance that has been alluringly labeled the “chemical of love,” makes the best case for the love-chocolate connection since it has been shown that people in love may actually have higher levels of PEA in their brain, as surmised from the fact that their urine is richer in a metabolite of this compound. In other words, people thrashing around in the throes of love pee differently from others.❞
Source: Office for Science and Society | The Chemical of Love
What is it?
It’s an amino acid. Because we are mammals, we can synthesize it inside our bodies, so it’s not considered an “essential amino acid”, i.e. one that we need to get from our diet. It is found in some foods, though, including:
- Other animals, especially other mammals
- Various beans, legumes, nuts, seeds. In particular almonds, soybeans, lentils, and chickpeas score highly
- Fermented foods
- Chocolate (popular lore holds this to be a good source of PEA; science finds it to be a fair option, but not in the same ballpark as the other items)
Fun fact: the reason Marvel’s Venom has a penchant for eating humans and chocolate is (according to the comics) because phenylethylamine is an essential amino acid for it.
What does it do for us?
It’s a Central Nervous System (CNS) stimulant, and also helps us synthesize critical neurotransmitters such as dopamine, norepinephrine (adrenaline) and serotonin:
It works similarly, but not identically, to amphetamines:
Is it safe?
We normally do this after the benefits, but “it works similarly to amphetamines” may raise an eyebrow or two, so let’s do it here:
- It is recommended to take no more than 500mg/day, with 100mg–500mg being typical doses
- It is not recommended to take it at all if you have, or have a predisposition to, any kind of psychotic disorder (especially schizophrenia, or bipolar disorder wherein you sometimes experience mania)
- This isn’t a risk for most people, but if you fall into the above category, the elevated dopamine levels could nudge you into a psychotic/manic episode that you probably don’t want.
See for example: Does phenylethylamine cause schizophrenia?
There are other contraindications too, so speak with your doctor/pharmacist before trying it.
On the other hand, if you are considering ADHD medication, then phenylethylamine could be a safer thing to try first, to see if it helps, before going to the heavy guns of actual amphetamines (as are commonly prescribed for ADHD). Same goes for depression and antidepressants.
What can I expect from PEA?
More dopamine, norepinephrine, and serotonin. Mostly the former two. Which means, you can expect stimulation.
For focus and attention, it’s so effective that it has been suggested (as we mentioned above) as a safer alternative to ADHD meds:
β-phenylethylamine, a small molecule with a large impact
…and may give similar benefits to people without ADHD, namely improved focus, attention, and mental stamina:
It also improves mood:
❝Phenylethylamine (PEA), an endogenous neuroamine, increases attention and activity in animals and has been shown to relieve depression in 60% of depressed patients. It has been proposed that PEA deficit may be the cause of a common form of depressive illness.
Effective dosage did not change with time. There were no apparent side effects. PEA produces sustained relief of depression in a significant number of patients, including some unresponsive to the standard treatments. PEA improves mood as rapidly as amphetamine but does not produce tolerance.❞
Source: Sustained antidepressant effect of PEA replacement
Where can I get it?
We don’t sell it, but here is an example product on Amazon for your convenience 😎
Enjoy!
Share This Post



Related Posts
-
The Pills That Reduce Alcohol Consumption
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Alcohol is, of course, unhealthy. Not even the famous “small glass of red” is recommended:
Can We Drink To Good Health? ← this was mostly about the purported heart health benefits, and the answer to the question is: no, we cannot, and as WHO has declared, “the only safe amount of alcohol is zero”)
See also: How Much Alcohol Does It Take To Increase Cancer Risk? ← the answer is “any” (although, the risk is dose-dependent, so if not abstaining completely, less is still better than more)
A lot of why people think that moderate drinking is healthy, that widespread popular belief stems from flawed associative studies that compared the following two categories of people:
- non-drinkers, including many former heavy drinkers who stopped because they realized the harm they were doing to themselves
- light drinkers, who have been able to continue drinking because of their otherwise good health
In other words, they looked at now-teetotal former alcoholics whose health was ruined by drinking and concluded “aha, non-drinkers have bad health; clearly some drinking is best”.
You can read more about this and how that flawed research was later disproven once the confounding variables were removed, here: Are You Making This Alcohol Mistake?
Drugs to the rescue!
“Take drugs to reduce the consumption of alcohol (another drug)” may seem like odd advice, but we’re not talking narcotics here.
Although! The drugs in question are active on the dopamine system, so yes, it is actually rather relevant. In other words, they reduce alcohol cravings (and thus, alcohol consumption), by improving dopamine signalling, which means people are less likely to reach for a bottle to self-medicate in order to try to get certain parts of the brain to light up.
Here some readers may be thinking “but I’m not trying to self-medicate; I just like enjoying the drink”, and if that’s you, then well, consider double-checking, for example:
The Alcohol Experiment – by Annie Grace ← it’s a 30-day no-alcohol challenge. If it’s not a dependency, you can do it no problem, right? Compare how willing you are (or not) to do this challenge, compared to, say, abstaining from some other thing that you frequently enjoy but isn’t addictive.
For example, this writer drinks, on average, 6 cups of spearmint tea per day. I love it. But it’s not addictive, and if challenged to skip it, I wouldn’t be counting the days or having to plan coping strategies.
So, with the knowledge in mind that alcohol is indeed addictive and does hijack dopamine circuitry (and more), a team of researchers (Dr. Andrea de Bejczy et al.) investigated the combination of two existing medications (varenicline, for smoking cessation, and bupropion, an antidepressant that works on the dopamine system) in treating alcohol use disorder.
The study
It was respectably large (n=384) 13-week randomized controlled trial, with adults aged 25–70 years with moderate-to-severe alcohol use disorder. About two thirds of the participants were male, the rest were female.
As for how effective it was: compared to placebo, the combination of both drugs reduced a blood alcohol biomarker (B-PEth) by about 39% and the percentage of self-reported heavy drinking days by about 31%.
It’s worthy of note also that actually varenicline achieved this reduction when tested alone, too; adding buproprion didn’t increase the effectiveness but did decrease the side effects:
❝Nausea is a well-known and troublesome side effect of treatment with varenicline. It was surprising but very encouraging to see that nausea decreased when bupropion was added. The fact that the combination treatment is more tolerable for patients increases the chances that they will complete the full course of treatment❞
~ Dr. Andrea de Bejczy
You can read the paper in full, here: Efficacy and safety of varenicline and bupropion, in combination and alone, for alcohol use disorder: a randomized, double-blind, placebo-controlled multicentre trial
And if you’d prefer a drug-free approach, check out: Rethinking Drinking: How To Reduce Or Quit Alcohol
Worried you’ve already done too much harm?
It’s never too early to quit drinking, but it’s also never too late:
What Happens To Your Body When You Stop Drinking Alcohol ← for a detailed timeline which parts of your body recover when
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Many Nonprofit (Wink, Wink) Hospitals Are Rolling in Money
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One owns a for-profit insurer, a venture capital company, and for-profit hospitals in Italy and Kazakhstan; it has just acquired its fourth for-profit hospital in Ireland. Another owns one of the largest for-profit hospitals in London, is partnering to build a massive training facility for a professional basketball team, and has launched and financed 80 for-profit start-ups. Another partners with a wellness spa where rooms cost $4,000 a night and co-invests with “leading private equity firms.”
Do these sound like charities?
These diversified businesses are, in fact, some of the country’s largest nonprofit hospital systems. And they have somehow managed to keep myriad for-profit enterprises under their nonprofit umbrella — a status that means they pay little or no taxes, float bonds at preferred rates, and gain numerous other financial advantages.
Through legal maneuvering, regulatory neglect, and a large dollop of lobbying, they have remained tax-exempt charities, classified as 501(c)(3)s.
“Hospitals are some of the biggest businesses in the U.S. — nonprofit in name only,” said Martin Gaynor, an economics and public policy professor at Carnegie Mellon University. “They realized they could own for-profit businesses and keep their not-for-profit status. So the parking lot is for-profit; the laundry service is for-profit; they open up for-profit entities in other countries that are expressly for making money. Great work if you can get it.”
Many universities’ most robust income streams come from their technically nonprofit hospitals. At Stanford University, 62% of operating revenue in fiscal 2023 was from health services; at the University of Chicago, patient services brought in 49% of operating revenue in fiscal 2022.
To be sure, many hospitals’ major source of income is still likely to be pricey patient care. Because they are nonprofit and therefore, by definition, can’t show that thing called “profit,” excess earnings are called “operating surpluses.” Meanwhile, some nonprofit hospitals, particularly in rural areas and inner cities, struggle to stay afloat because they depend heavily on lower payments from Medicaid and Medicare and have no alternative income streams.
But investments are making “a bigger and bigger difference” in the bottom line of many big systems, said Ge Bai, a professor of health care accounting at the Johns Hopkins University Bloomberg School of Public Health. Investment income helped Cleveland Clinic overcome the deficit incurred during the pandemic.
When many U.S. hospitals were founded over the past two centuries, mostly by religious groups, they were accorded nonprofit status for doling out free care during an era in which fewer people had insurance and bills were modest. The institutions operated on razor-thin margins. But as more Americans gained insurance and medical treatments became more effective — and more expensive — there was money to be made.
Not-for-profit hospitals merged with one another, pursuing economies of scale, like joint purchasing of linens and surgical supplies. Then, in this century, they also began acquiring parts of the health care systems that had long been for-profit, such as doctors’ groups, as well as imaging and surgery centers. That raised some legal eyebrows — how could a nonprofit simply acquire a for-profit? — but regulators and the IRS let it ride.
And in recent years, partnerships with, and ownership of, profit-making ventures have strayed further and further afield from the purported charitable health care mission in their community.
“When I first encountered it, I was dumbfounded — I said, ‘This not charitable,’” said Michael West, an attorney and senior vice president of the New York Council of Nonprofits. “I’ve long questioned why these institutions get away with it. I just don’t see how it’s compliant with the IRS tax code.” West also pointed out that they don’t act like charities: “I mean, everyone knows someone with an outstanding $15,000 bill they can’t pay.”
Hospitals get their tax breaks for providing “charity care and community benefit.” But how much charity care is enough and, more important, what sort of activities count as “community benefit” and how to value them? IRS guidance released this year remains fuzzy on the issue.
Academics who study the subject have consistently found the value of many hospitals’ good work pales in comparison with the value of their tax breaks. Studies have shown that generally nonprofit and for-profit hospitals spend about the same portion of their expenses on the charity care component.
Here are some things listed as “community benefit” on hospital systems’ 990 tax forms: creating jobs; building energy-efficient facilities; hiring minority- or women-owned contractors; upgrading parks with lighting and comfortable seating; creating healing gardens and spas for patients.
All good works, to be sure, but health care?
What’s more, to justify engaging in for-profit business while maintaining their not-for-profit status, hospitals must connect the business revenue to that mission. Otherwise, they pay an unrelated business income tax.
“Their CEOs — many from the corporate world — spout drivel and turn somersaults to make the case,” said Lawton Burns, a management professor at the University of Pennsylvania’s Wharton School. “They do a lot of profitable stuff — they’re very clever and entrepreneurial.”
The truth is that a number of not-for-profit hospitals have become wealthy diversified business organizations. The most visible manifestation of that is outsize executive compensation at many of the country’s big health systems. Seven of the 10 most highly paid nonprofit CEOs in the United States run hospitals and are paid millions, sometimes tens of millions, of dollars annually. The CEOs of the Gates and Ford foundations make far less, just a bit over $1 million.
When challenged about the generous pay packages — as they often are — hospitals respond that running a hospital is a complicated business, that pharmaceutical and insurance execs make much more. Also, board compensation committees determine the payout, considering salaries at comparable institutions as well as the hospital’s financial performance.
One obvious reason for the regulatory tolerance is that hospital systems are major employers — the largest in many states (including Massachusetts, Pennsylvania, Minnesota, Arizona, and Delaware). They are big-time lobbying forces and major donors in Washington and in state capitals.
But some patients have had enough: In a suit brought by a local school board, a judge last year declared that four Pennsylvania hospitals in the Tower Health system had to pay property taxes because its executive pay was “eye popping” and it demonstrated “profit motives through actions such as charging management fees from its hospitals.”
A 2020 Government Accountability Office report chided the IRS for its lack of vigilance in reviewing nonprofit hospitals’ community benefit and recommended ways to “improve IRS oversight.” A follow-up GAO report to Congress in 2023 said, “IRS officials told us that the agency had not revoked a hospital’s tax-exempt status for failing to provide sufficient community benefits in the previous 10 years” and recommended that Congress lay out more specific standards. The IRS declined to comment for this column.
Attorneys general, who regulate charity at the state level, could also get involved. But, in practice, “there is zero accountability,” West said. “Most nonprofits live in fear of the AG. Not hospitals.”
Today’s big hospital systems do miraculous, lifesaving stuff. But they are not channeling Mother Teresa. Maybe it’s time to end the community benefit charade for those that exploit it, and have these big businesses pay at least some tax. Communities could then use those dollars in ways that directly benefit residents’ health.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Medications That Shouldn’t Be Taken Long-term (With Natural Alternatives)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Leonid Kim helps us avoid hurting our organs and more:
Swaps to consider
Body
- PPIs (usually prescribed for heartburn): drugs like omeprazole and esomeprazole reduce stomach acid but long-term use is associated with kidney injury, magnesium deficiency (on which note, do be aware of: How’s Your Magnesium Depletion Score?), and a 65% increased odds of vitamin B12 deficiency after 2 or more years. If you are going to supplement B12, by the way, that’s a good idea for a lot of people, but do avoid making a common mistake that many make in this regard: Which B Vitamins? It Makes A Difference ← in short, the most common vitamer of B12, cyanocobalamin, isn’t that effective, and you might want to spring for methylcobalamin, hydroxycobalamin, and/or adenosylcobalamin, all three of which are active vitamers of B12 that the body can use much more efficiently. You may be wondering why, then, cyanocobalamin is the most common: simple, it’s cheaper to produce!
- Heartburn alternatives: reduce visceral fat to lower stomach pressure, practice diaphragmatic breathing to strengthen the lower esophageal sphincter, and improve gastric emptying with walking after meals, and ginger tea. See also: Acid Reflux After Meals? Here’s How To Stop It Naturally
- Z-drugs (sleep medications): drugs like zolpidem act on the GABA system to induce sleep but can lead to dependence within weeks, and are linked to complex sleep behaviors like sleepwalking, cooking, or driving while asleep. Needless to say, those things are not good for the health.
- Sleep alternatives: maintain consistent sleep and wake times and get morning light exposure within 30 minutes of waking to regulate your circadian rhythm. If you do want something to take, though, swing by: Safe Effective Sleep Aids For Seniors
- Anticholinergics: drugs like diphenhydramine, oxybutynin, and amitriptyline are used for allergies, bladder issues, sleep, and depression and are associated with a 46% increased risk of dementia after 3 or more months of use, with risk increasing alongside cumulative exposure.
- Anticholinergic alternatives: switch to second-generation antihistamines when appropriate (see: Antihistamines’ Generation Gap) and use bladder training and pelvic floor muscle training, which can reduce incontinence episodes by 60 to 80% in women. You might also want to take note of: Foods Linked To Urinary Incontinence In Middle-Age (& Foods That Avert It)
- Gabapentin: originally approved for seizures and postherpetic nerve pain but widely used for other conditions, with long-term use associated with cognitive slowing (we wrote about that here: The Painkiller That Increases Cognitive Impairment Risk By 85%), dizziness, impaired balance, and physical dependence.
- Neuropathy alternatives: address underlying causes like blood sugar control, improve insulin resistance with diet and exercise, and correct vitamin deficiencies to reduce nerve damage and pain (learn more: Peripheral Neuropathy: How To Avoid It, Manage It, Treat It).
For less on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Are You Taking PIMs? Getting Off The Overmedication Train ← “PIMs” stands for “potentially inappropriate medications”, be they prescribed in error, or to treat a side effect of some other medication, or to treat something that has now long-since passed.
Also, for that matter:
Before You Reach For That Tylenol… ← Tylenol (paracetamol/acetaminophen) is intended for occasional use only, and can cause severe problems if used chronically (not to mention death, if overused)
And while we’re doing painkillers, you might also want to check out:
The Commonly-Prescribed Painkiller That Barely Works (And Is Dangerous)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- PPIs (usually prescribed for heartburn): drugs like omeprazole and esomeprazole reduce stomach acid but long-term use is associated with kidney injury, magnesium deficiency (on which note, do be aware of: How’s Your Magnesium Depletion Score?), and a 65% increased odds of vitamin B12 deficiency after 2 or more years. If you are going to supplement B12, by the way, that’s a good idea for a lot of people, but do avoid making a common mistake that many make in this regard: Which B Vitamins? It Makes A Difference ← in short, the most common vitamer of B12, cyanocobalamin, isn’t that effective, and you might want to spring for methylcobalamin, hydroxycobalamin, and/or adenosylcobalamin, all three of which are active vitamers of B12 that the body can use much more efficiently. You may be wondering why, then, cyanocobalamin is the most common: simple, it’s cheaper to produce!


