How Much Alcohol Does It Take To Increase Cancer Risk?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Alcohol is, of course, unhealthy. Not even the famous “small glass of red” is recommended:
Alcohol also increases all-cause mortality at any dose (even “low-risk drinking”):
Alcohol Consumption Patterns and Mortality Among Older Adults
…and the World Health Organization has declared that the only safe amount of alcohol is zero:
WHO: No level of alcohol consumption is safe for our health
But what of alcohol and cancer? According to the American Association of Cancer Research’s latest report, more than half of Americans do not know that alcohol increases the risk of cancer:
Source: AACR Cancer Progress Report
Why/how does alcohol increase the risk of cancer?
There’s an obvious aspect and a less obvious but very important aspect:
- The obvious: alcohol damages almost every system in the body, and so it’s little surprise if that includes systems whose job it is to keep us safe from cancer.
- The less obvious: alcohol is largely metabolized by certain enzymes that have an impact on DNA repair, such as alcohol dehydrogenases and aldehyde dehydrogenases, amongst others, and noteworthily, acetaldehyde (the main metabolite of alcohol) is itself genotoxic.
Read more: Alcohol & Cancer
This is important, because it means alcohol also increases the risk of cancers other than the obvious head/neck, laryngeal, esophageal, liver, and colorectal cancers.
However, those cancers are of course the most well-represented of alcohol-related cancers, along with breast cancer (this has to do with alcohol’s effect on estrogen metabolism).
If you’re curious about the numbers, and the changes in risk if one reduces/quits/reprises drinking:
❝The increased alcohol-related cancer incidence was associated with dose; those who changed from nondrinking to mild (adjusted hazard ratio [aHR], 1.03; 95% CI, 1.00-1.06), moderate (aHR, 1.10; 95% CI, 1.02-1.18), or heavy (aHR, 1.34; 95% CI, 1.23-1.45) drinking levels had an associated higher risk than those who did not drink.
Those with mild drinking levels who quit drinking had a lower risk of alcohol-related cancer (aHR, 0.96; 95% CI, 0.92-0.99) than those who sustained their drinking levels.
Those with moderate (aHR, 1.07; 95% CI, 1.03-1.12) or heavy (aHR, 1.07; 95% CI, 1.02-1.12) drinking levels who quit drinking had a higher all cancer incidence than those who sustained their levels, but when quitting was sustained, this increase in risk disappeared.
Results of this study showed that increased alcohol consumption was associated with higher risks for alcohol-related and all cancers, whereas sustained quitting and reduced drinking were associated with lower risks of alcohol-related and all cancers.
Alcohol cessation and reduction should be reinforced for the prevention of cancer.❞
Source: Association Between Changes in Alcohol Consumption and Cancer Risk
Worried it’s too late?
If you’re reading this (and thus, evidently, still alive), it isn’t. It’s never too late (nor too early) to reduce, or ideally stop, drinking. Even if you already have cancer, drinking more alcohol will only exacerbate things, and abstaining from alcohol will improve your chances of recovery.
For a reassuring timeline of recovery from alcohol-related damage, see:
What Happens To Your Body When You Stop Drinking Alcohol
Want to stop, but have tried before and find it daunting?
There are a few ways to make it a lot easier:
Rethinking Drinking: How To Reduce Or Quit Alcohol
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Lies That Depression Tells Us

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In this short (6:42) video, psychiatrist Dr. Tracey Marks talks about 8 commonly-believed lies that depression often tells us. They are:
- “I don’t measure up”
- “No one cares about me”
- “I’m better off alone”
- “No one understands”
- “It’s all my fault”
- “I have no reason to be depressed”
- “Nothing matters”
- “I’ll never get better”
Some of these can be reinforced by people around us; it’s easy to believe that “no one understands” if for example the few people we interact with the most don’t understand, or that “I have no reason to be depressed” if people try to cheer you up by pointing out your many good fortunes.
The reality, of course, is that depression is a large, complex, and many-headed beast, with firm roots in neurobiology.
There are things we can do that may ameliorate it… But they also may not, and sometimes life is just going to suck for a while. That doesn’t mean we should give up (that, too, is depression lying to us, per “I’ll never get better”), but it does mean that we should not be so hard on ourselves for not having “walked it off” the way one might “just walk off” a broken leg.
Oh, you can’t “just walk off” a broken leg? Well then, perhaps it’s not surprising if we don’t “just think off” a broken brain, either. The brain can rebuild itself, but that’s a slow process, so buckle in:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to know more?
You might like these previous articles of ours about depression (managing it, and overcoming it):
- The Mental Health First-Aid That You’ll Hopefully Never Need
- Behavioral Activation Against Depression & Anxiety
- The Easiest Way To Take Up Journaling
- Antidepressants: Personalization Is Key!
Take care!
Share This Post
-

What Your Skin Texture Says About Your Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Andrea Suarez, dermatologist, shows us what to watch out for:
To the touch
We (and videos that we share here!) talk a lot about the appearance of various skin conditions, but skin texture is more about the physical feel and surface quality of your skin—including roughness, flaking, bumpy follicular changes, thickening, thinning, crepey fragility, or a doughy or hardened feel—and while many changes are harmless, certain patterns in the certain contexts can be signs of disease, including of the kind that are more than skin-deep.
What different skin textures mean:
- Persistent roughness and flaking: ongoing dry, rough, flaky skin is usually due to barrier dysfunction from overexfoliation, harsh cleansers, hot water, low humidity, or aging, but in some cases is because of hypothyroidism or an essential fatty acid deficiency.
- Velvety dark thickened skin: velvety, dark, thickened plaques in skin folds such as the neck or underarms suggest acanthosis nigricans, a sign of insulin resistance commonly associated with type 2 diabetes, that can appear before blood sugar levels cross diagnostic thresholds.
- Sudden adult acne or oily skin: new-onset oily skin and acne in adulthood may relate to hormonal shifts such as polycystic ovary syndrome (PCOS), hyperandrogenism, perimenopause, or chronic stress affecting cortisol, especially if accompanied by irregular periods, hair changes, or metabolic warning signs.
- Waxy puffy doughy skin: thick, swollen, doughy skin—sometimes progressing to myxedema with mucopolysaccharide buildup—alongside fatigue, cold intolerance, and hair thinning suggests hypothyroidism and often improves with appropriate treatment.
- Fragile crepey easily bruised skin: thin, fragile, crepey skin known as dermatoporosis is most commonly due to cumulative sun damage but can also result from chronic glucocorticoid use, prolonged topical steroid application, or malnutrition.
- Keratosis pilaris: rough follicular bumps (keratosis pilaris) are common and often genetic, but can also be associated with atopic dermatitis, asthma, allergic rhinitis, ichthyosis vulgaris, type 2 diabetes, insulin resistance, Down syndrome, or (rarely) certain medications.
- Phrynoderma: larger, hyperpigmented, hard follicular bumps called phrynoderma are generally linked to vitamin A deficiency and can occur with malabsorption, chronic illness, or severe dietary restriction.
- Skin tags: a few skin tags are common and harmless, but numerous tags—especially alongside acanthosis nigricans—can be a sign of insulin resistance due to elevated insulin-like growth factor stimulating epidermal proliferation (i.e. too many skin cells being made in one place).
- Scleredema: non-pitting, woody skin thickening on the upper back and neck is called scleredema has three variants (post-streptococcal, monoclonal gammopathy–associated, and diabeticorum); the diabetic form most often seen in long-standing, poorly controlled diabetes.
Some quick myths to bust, while we’re at it: textural changes don’t indicate toxin buildup, liver failure, candida overgrowth, or leaky gut, as these claims are common online myths often used to market unnecessary products.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Share This Post
-

Heart Health vs Systemic Stress
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
At The Heart Of Good Health

This is Dr. Michelle Albert. She’s a cardiologist with a decades-long impressive career, recently including a term as the president of the American Heart Association. She’s the current Admissions Dean at UCSF Medical School. She’s accumulated enough awards and honors that if we list them, this email will not fit in your inbox without getting clipped.
What does she want us to know?
First, lifestyle
Although Dr. Albert is also known for her work with statins (which found that pravastatin may have anti-inflammatory effects in addition to lipid-lowering effects, which is especially good news for women, for whom the lipid-lowering effects may be less useful than for men), she is keen to emphasize that they should not be anyone’s first port-of-call unless “first” here means “didn’t see the risk until it was too late and now LDL levels are already ≥190 mg/dL”.
Instead, she recommends taking seriously the guidelines on:
- getting plenty of fruit, vegetables, whole grains, lean protein
- avoiding red meat, processed meats, refined carbohydrates, and sweetened beverages
- getting your 150 minutes per week of moderate exercise
- avoiding alcohol, and definitely abstaining from smoking
See also: These Top Five Things Make The Biggest Difference To Health
Next, get your house in order
No, not your home gym—though sure, that too!
But rather: after the “Top Five Things” we linked just above, the sixth on the list would be “reduce stress”. Indeed, as Dr. Albert says:
❝Heart health is not just about the physical heart but also about emotional well-being. Stress management is crucial for a healthy heart❞
~ Dr. Michelle Albert
This is where a lot of people would advise mindfulness meditation, CBT, somatic therapies, and the like. And these things are useful! See for example:
No-Frills, Evidence-Based Mindfulness
…and:
However, Dr. Albert also advocates for awareness of what some professionals have called “Shit Life Syndrome”.
This is more about socioeconomic factors. There are many of those that can’t be controlled by the individual, for example:
❝Adverse maternal experiences such as depression, economic issues and low social status can lead to poor cognitive outcomes as well as cardiovascular disease.
Many jarring statistics illuminate a marked wealth gap by race and ethnicity… You might be thinking education could help bridge that gap. But it is not that simple.
While education does increase wealth, the returns are not the same for everyone. Black persons need a post-graduate degree just to attain similar wealth as white individuals with a high school degree.❞
~ Dr. Michelle Albert
Read in full: AHA president: The connection between economic adversity and cardiovascular health
What this means in practical terms (besides advocating for structural change to tackle the things such as the racism that has been baked into a lot of systems for generations) is:
Be aware not just of your obvious health risk factors, but also your socioeconomic risk factors, if you want to have good general health outcomes.
So for example, let’s say that you, dear reader, are wealthy and white, in which case you have some very big things in your favor, but are you also a woman? Because if so…
Women and Minorities Bear the Brunt of Medical Misdiagnosis
See also, relevant for some: Obesity Discrimination In Healthcare Settings ← you’ll need to scroll to the penultimate section for this one.
In other words… If you are one of the majority of people who is a woman and/or some kind of minority, things are already stacked against you, and not only will this have its own direct harmful effect, but also, it’s going to make your life harder and that stress increases CVD risk more than salt.
In short…
This means: tackle not just your stress, but also the things that cause that. Look after your finances, gather social support, know your rights and be prepared to self-advocate / have someone advocate for you, and go into medical appointments with calm well-prepared confidence.
Take care!
Share This Post


-

Anticancer: A New Way Of Life – by Dr. David Servan-Schreiber
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A cancer survivor himself, Dr. Servan-Schreiber found himself unimpressed with the advice he was given upon diagnosis, and set out to find better. This, he achieved.
He first provides an introductory overview of cancer, and then devotes most of the book to detailing how to create a “terrain” (the environment of your body and all that you do with/to it) that is hostile to cancer.
This includes things like diet, of course, but also exercise (the right way!), mindset, and much more. He doesn’t cover much about standard medical treatments, as he assumes the reader will already be advised about those by their oncologist, and in any case, such treatments are constantly changing as new discoveries are made. It’s worth mentioning that while he advocates strongly for complementary medicine, he does also make clear it should be just that—complementary—and not a replacement for regular treatments in cases where such are recommended.
The style is comprehensible pop-science, written for the lay reader, and yet with copious scientific references—more than 30 pages thereof. But as well as that, it’s a personal account, often revisiting his own cancer journey to illustrate one point or another, be it something that went well for him or badly, there’s always something to learn.
Bottom line: this book is important for anyone facing cancer, and useful for anyone who simply would like to improve their odds in a more informed fashion. As he notes, “all of us have cancer cells in our bodies, but not all of us will develop cancer”, and it’s good to try to be on the healthiest side of that.
Click here to check out Anticancer, and live an anticancer life!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Self-Care That’s Not Just Self-Indulgence
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Self-Care That’s Not Just Self-Indulgence
Self-care is often seen as an excuse for self-indulgence. Worse, it’s often used as an excuse for self-indulgence—in ways that can end up making us feel worse.
It’s a bit like dietary “cheat days”. If your diet needs cheat days, your diet probably isn’t right for you!
How to recognize the difference between self-care and self-indulgence?
Statistically, the majority of our subscribers are parents (whose children are now mostly grown up, but still, the point is that parenting experience has been gleaned), and/or are or have been caregivers of some form or other.
When a small child is ill, we (hopefully!) look after them carefully:
- We don’t expect too much of them, but…
- …we do expect them to adhere to things consistent with their recovery.
Critically: an important part of self-care is that it actually should be care.
Let’s spell something out: neglect is not care!
How this works for physical and mental health
If you overdo it in physical exercise, it’s right and correct to take a break to recover, and during that time, do things that will hasten one’s recovery. For example:
Overdone It? How To Speed Up Recovery After Exercise
But it’s well-known that if you just do nothing, your condition will likely deteriorate. Also, “a break to recover” is going to be as short as is necessary to recover. Then you’ll ease back into exercise, but you will get back to it.
For mental health it’s just the same. If we for whatever reason need to take a step back, it’s right and correct to do take a break to recover, and during that time, do things that will hasten one’s recovery.
Sometimes, if for example it’s just a case of burnout, rest is the best medicine, and even rest can be an active process. See for example:
How To Rest More Efficiently (Yes, Really)
So the question to ask, when it comes to self-care vs self-indulgence, is:
“Is this activity helping me to get better?”
Some examples:
Probably not great self-care activities:
- Oversleeping (unless you were sleep-deprived, in which case, it’s better to get an earlier night than a later morning, if possible)
- Overeating (comfort-eating is a thing, but your actual problems will still be there)
- Mindless activities (mindless scrolling, TV-watching, game-playing, etc)
Probably better self-care activities:
- Enjoyable physical activity (whatever that may be for you)
- Preparing your favorite food, and then enjoying it mindfully
- Engaging in a personal project that might not be that important, but it’s fulfilling to you (hobbies etc can fall into this category)
- Scheduling some time, and committing some resources, to tackling whatever problem(s) you are facing that’s prompting you to need this self-care.
- Doing the tasks you want to hide away from, but making them fun.
What’s your go-to self-care? We love to hear from you, so feel free to hit “reply” to this email, or use the handy feedback form at the bottom!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
I’ve recovered from a cold but I still have a hoarse voice. What should I do?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cold, flu, COVID and RSV have been circulating across Australia this winter. Many of us have caught and recovered from one of these common upper respiratory tract infections.
But for some people their impact is ongoing. Even if your throat isn’t sore anymore, your voice may still be hoarse or croaky.
So what happens to the voice when we get a virus? And what happens after?
Here’s what you should know if your voice is still hoarse for days – or even weeks – after your other symptoms have resolved.
Why does my voice get croaky during a cold?
A healthy voice is normally clear and strong. It’s powered by the lungs, which push air past the vocal cords to make them vibrate. These vibrations are amplified in the throat and mouth, creating the voice we hear.
The vocal cords are two elastic muscles situated in your throat, around the level of your laryngeal prominence, or Adam’s apple. (Although everyone has one, it tends to be more pronounced in males.) The vocal cords are small and delicate – around the size of your fingernail. Any small change in their structure will affect how the voice sounds.
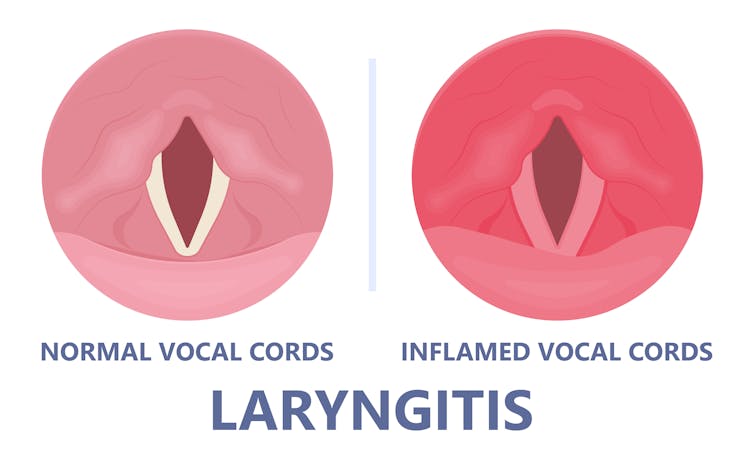
When the vocal cords become inflamed – known as laryngitis – your voice will sound different. Laryngitis is a common part of upper respiratory tract infections, but can also be caused through misuse.
Viruses such as the common cold can inflame the vocal cords. Pepermpron/Shutterstock Catching a virus triggers the body’s defence mechanisms. White blood cells are recruited to kill the virus and heal the tissues in the vocal cords. They become inflamed, but also stiffer. It’s harder for them to vibrate, so the voice comes out hoarse and croaky.
In some instances, you may find it hard to speak in a loud voice or have a reduced pitch range, meaning you can’t go as high or loud as normal. You may even “lose” your voice altogether.
Coughing can also make things worse. It is the body’s way of trying to clear the airways of irritation, including your own mucus dripping onto your throat (post-nasal drip). But coughing slams the vocal cords together with force.
Chronic coughing can lead to persistent inflammation and even thicken the vocal cords. This thickening is the body trying to protect itself, similar to developing a callus when a pair of new shoes rubs.
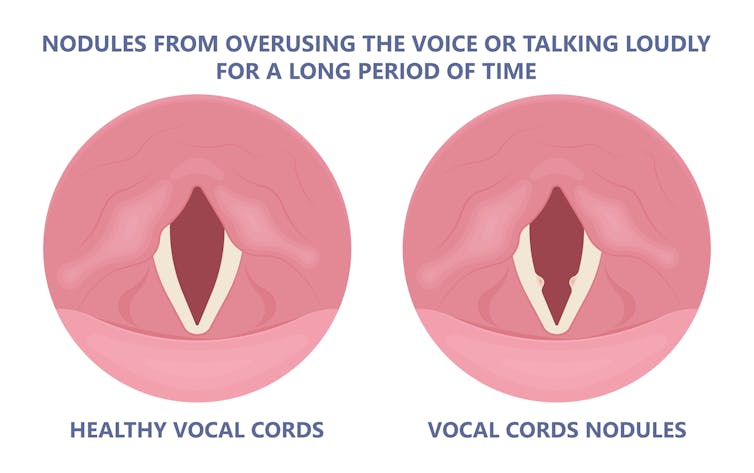
Thickening on your vocal cords can lead to physical changes in the vocal cords – such as developing a growth or “nodule” – and further deterioration of your voice quality.
Coughing and exertion can cause inflamed vocal cords to thicken and develop nodules. Pepermpron/Shutterstock How can you care for your voice during infection?
People who use their voices a lot professionally – such as teachers, call centre workers and singers – are often desperate to resume their vocal activities. They are more at risk of forcing their voice before it’s ready.
The good news is most viral infections resolve themselves. Your voice is usually restored within five to ten days of recovering from a cold.
Occasionally, your pharmacist or doctor may prescribe cough suppressants to limit additional damage to the vocal cords (among other reasons) or mucolytics, which break down mucus. But the most effective treatments for viral upper respiratory tract infections are hydration and rest.
Drink plenty of water, avoid alcohol and exposure to cigarette smoke. Inhaling steam by making yourself a cup of hot water will also help clear blocked noses and hydrate your vocal cords.
Rest your voice by talking as little as possible. If you do need to talk, don’t whisper – this strains the muscles.
Instead, consider using “confidential voice”. This is a soft voice – not a whisper – that gently vibrates your vocal cords but puts less strain on your voice than normal speech. Think of the voice you use when communicating with someone close by.
During the first five to ten days of your infection, it is important not to push through. Exerting the voice by talking a lot or loudly will only exacerbate the situation. Once you’ve recovered from your cold, you can speak as you would normally.
What should you do if your voice is still hoarse after recovery?
If your voice hasn’t returned to normal after two to three weeks, you should seek medical attention from your doctor, who may refer you to an ear nose and throat specialist.
If you’ve developed a nodule, the specialist would likely refer you to a speech pathologist who will show you how to take care of your voice. Many nodules can be treated with voice therapy and don’t require surgery.
You may have also developed a habit of straining your vocal cords, if you forced yourself to speak or sing while they were inflamed. This can be a reason why some people continue to have a hoarse voice even when they’ve recovered from the cold.
In those cases, a speech pathologist may play a valuable role. They may teach you to exercises that make voicing more efficient. For example, lip trills (blowing raspberries) are a fun and easy way you can learn to relax the voice. This can help break the habit of straining your voice you may have developed during infection.
Yeptain Leung, Postdoctoral Research and Lecturer of Speech Pathology, School of Health Sciences, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: