Our blood-brain barrier stops bugs and toxins getting to our brain. Here’s how it works
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
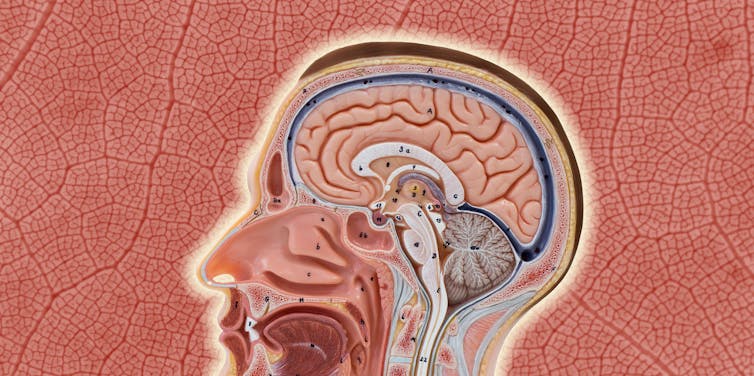
Our brain is an extremely complex and delicate organ. Our body fiercely protects it by holding onto things that help it and keeping harmful things out, such as bugs that can cause infection and toxins.
It does that though a protective layer called the blood-brain barrier. Here’s how it works, and what it means for drug design.
First, let’s look at the circulatory system
Adults have roughly 30 trillion cells in their body. Every cell needs a variety of nutrients and oxygen, and they produce waste, which needs to be taken away.
Our circulatory system provides this service, delivering nutrients and removing waste.
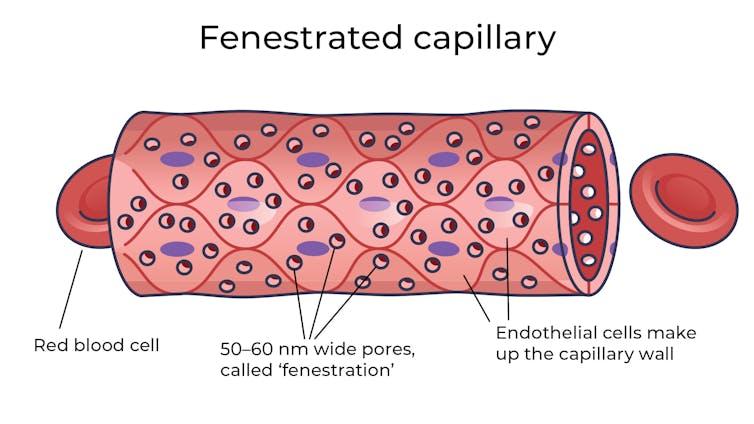
Where the circulatory system meets your cells, it branches down to tiny tubes called capillaries. These tiny tubes, about one-tenth the width of a human hair, are also made of cells.
But in most capillaries, there are some special features (known as fenestrations) that allow relatively free exchange of nutrients and waste between the blood and the cells of your tissues.
It’s kind of like pizza delivery
One way to think about the way the circulation works is like a pizza delivery person in a big city. On the really big roads (vessels) there are walls and you can’t walk up to the door of the house and pass someone the pizza.
But once you get down to the little suburban streets (capillaries), the design of the streets means you can stop, get off your scooter and walk up to the door to deliver the pizza (nutrients).
We often think of the brain as a spongy mass without much blood in it. In reality, the average brain has about 600 kilometres of blood vessels.
The difference between the capillaries in most of the brain and those elsewhere is that these capillaries are made of specialised cells that are very tightly joined together and limit the free exchange of anything dissolved in your blood. These are sometimes called continuous capillaries.

This is the blood brain barrier. It’s not so much a bag around your brain stopping things from getting in and out but more like walls on all the streets, even the very small ones.
The only way pizza can get in is through special slots and these are just the right shape for the pizza box.
The blood brain barrier is set up so there are specialised transporters (like pizza box slots) for all the required nutrients. So mostly, the only things that can get in are things that there are transporters for or things that look very similar (on a molecular scale).
The analogy does fall down a little bit because the pizza box slot applies to nutrients that dissolve in water. Things that are highly soluble in fat can often bypass the slots in the wall.
Why do we have a blood-brain barrier?
The blood brain barrier is thought to exist for a few reasons.
First, it protects the brain from toxins you might eat (think chemicals that plants make) and viruses that often can infect the rest of your body but usually don’t make it to your brain.
It also provides protection by tightly regulating the movement of nutrients and waste in and out, providing a more stable environment than in the rest of the body.
Lastly, it serves to regulate passage of immune cells, preventing unnecessary inflammation which could damage cells in the brain.
What it means for medicines
One consequence of this tight regulation across the blood brain barrier is that if you want a medicine that gets to the brain, you need to consider how it will get in.
There are a few approaches. Highly fat-soluble molecules can often pass into the brain, so you might design your drug so it is a bit greasy.

Another option is to link your medicine to another molecule that is normally taken up into the brain so it can hitch a ride, or a “pro-drug”, which looks like a molecule that is normally transported.
Using it to our advantage
You can also take advantage of the blood brain barrier.
Opioids used for pain relief often cause constipation. They do this because their target (opioid receptors) are also present in the nervous system of the intestines, where they act to slow movement of the intestinal contents.
Imodium (Loperamide), which is used to treat diarrhoea, is actually an opioid, but it has been specifically designed so it can’t cross the blood brain barrier.
This design means it can act on opioid receptors in the gastrointestinal tract, slowing down the movement of contents, but does not act on brain opioid receptors.
In contrast to Imodium, Ozempic and Victoza (originally designed for type 2 diabetes, but now popular for weight-loss) both have a long fat attached, to improve the length of time they stay in the body.
A consequence of having this long fat attached is that they can cross the blood-brain barrier, where they act to suppress appetite. This is part of the reason they are so effective as weight-loss drugs.
So while the blood brain barrier is important for protecting the brain it presents both a challenge and an opportunity for development of new medicines.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

But First, Inner Peace – by Case Kenny

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Thinking positively and vividly imagining a Ferrari parked in your driveway will not, in fact, cause it to manifest there.
You know what that method does work for, though? Feelings.
This book is essentially a guided thought-and-feeling modelling system that, consisting of 60 chapters to be taken one-per-day, aims to rewire your mind for inner peace.
This is not, however, just a matter of “imagine peacefulness”, or nice-sounding platitudes. Rather, at the end of each chapter there is an exercise and journaling prompts; effectively, work to do along the way.
Weighing in at 438 pages, this is a sizeable book, but part of that is because of the space to write answers to journaling prompts. Still, it’s not exactly a pamphlet, either—there is serious and extensive content here too.
Like any daily reader, you can zip through it all at once if you like, but a benefit to doing the chapter-a-day approach is that it sets a habit of mindful reflection, and gives you a chance to implement each thing, one per day, building up new habits in that regard, too. In contrast, reading it all in one sitting wouldn’t give that.
Bottom line: without inner peace, we don’t have much. Treat yourself—you deserve it.
Click here to check out But First, Inner Peace, and enjoy inner peace!
Share This Post
-

Kale vs Red Cabbage – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing kale to red cabbage, we picked the kale.
Why?
While red cabbage has its own merits, this one wasn’t close:
In terms of macros, kale has more fiber, carbs, and protein, winning this category.
In the category of vitamins, kale has a lot more of vitamins A, B1, B2, B3, B6, B7, B9, C, E, and K, while red cabbage has more of vitamin B5 and choline; an easy win for kale.
Looking at minerals, kale has a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while red cabbage is not higher in any minerals—handing kale the victory here.
In other considerations, kale has more polyphenols, especially quercetin and kaempferol, winning one more round.
Adding up the sections gives a clear overall win for kale, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
- Brain Food? The Eyes Have It! ← this is about the abundant carotenoids (especially lutein) in dark leafy greens, such as kale
- Fight Inflammation & Protect Your Brain, With Quercetin
- What Does Kaempferol Do, Anyway?
Enjoy!
Share This Post
-
Asparagus vs Sweetcorn – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing asparagus to sweetcorn, we picked the asparagus.
Why?
In terms of macros, sweetcorn starts off strong with slightly more protein and notably more carbs for the same fiber, while still keeping glycemic index low, so we say this first round is a marginal win for corn.
In the category of vitamins, asparagus has a lot more of vitamins A (yes, really, 4x more!), B2, B7, B9, E, and K (138x the amount for this one), while sweetcorn has more of vitamins B2, B5, and C, giving asparagus an overwhelming win here.
For anyone wondering “why are we so surprised about the vitamin A?”, it’s because vitamin A makes things yellow, and corn is yellow while asparagus is green. But, there are more factors that affect the color of each plant, that’s all.
Looking at minerals, asparagus has more calcium, copper, iron, potassium, selenium, and zinc, while corn has more magnesium, phosphorus, and potassium, yielding a compelling 5:3 win to asparagus (especially with asparagus having 12x the calcium; do not underestimate green things as a source of calcium; where do you think cows get theirs from?).
In other considerations, asparagus has a higher polyphenol content (with quercetin scoring notably), while sweetcorn is high in carotenoids such as lutein (whence the yellow color, by the way). So, we’ll call it a tie in this round.
Adding up the sections makes for an overall win for asparagus on tie-breaks (both plants won two sections each, but asparagus had the greater margins of difference by far), but by all means enjoy either or both, as diversity is best!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Share This Post


Related Posts
-
Apple vs Starfruit – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apples to starfruit, we picked the starfruit.
Why?
In terms of macros, apples have 2x the carbs while starfruit have slightly more fiber and protein; by most people’s macro standards that’s a win for starfruit.
In the category of vitamins, apples have more of vitamins B2 and B6, while starfruit has more of vitamins B3, B5, B7, B9, and C, winning in this round.
Looking at minerals, apples have more calcium and iron, while starfruit has more copper, magnesium, manganese, phosphorus, potassium, selenium, and zinc, winning a third round in a row.
In other considerations, there are not really other considerations unless you have an allergy; both have comparably modest polyphenol profiles, and neither has any known exciting medicinal properties. So, a tie here.
Adding up the sections makes for a clear overall win for starfruit, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Stevia vs Acesulfame Potassium – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing stevia to acesulfame potassium, we picked the stevia.
Why?
You may be wondering: is acesulfame potassium a good source of potassium?
And the answer is: no, it is not. Obviously, it does contain potassium, but let’s do some math here:
- Acesulfame potassium is 200x sweeter than sugar
- Therefore replacing a 15g teaspoon of sugar = 75mg acesulfame potassium
- Acesulfame potassium’s full name is “potassium 6-methyl-2,2-dioxo-2H-1,2λ6,3-oxathiazin-4-olate”
- That’s just one potassium atom in there with a lot of other stuff
- Acesulfame potassium has a molar mass of 201.042 g/mol
- Potassium itself has a molar mass of 39.098 g/mol
- Therefore acesulfame potassium is 100(39.098/201.042) = 19.45% potassium by mass
- So that 75mg of acesulfame potassium contains just under 15mg of potassium, which is less than 0.5% of your recommended daily amount of potassium. Please consider eating a fruit instead.
So, that’s that, and the rest of the nutritional values of both sweeteners are just a lot of zeros.
What puts stevia ahead? Simply, based on studies available so far, moderate consumption of stevia improves gut microdiversity, whereas acesulfame potassium harms gut microdiversity:
- The Effects of Stevia Consumption on Gut Bacteria: Friend or Foe?
- The Artificial Sweetener Acesulfame Potassium Affects the Gut Microbiome
Want to give stevia a try?
Here’s an example product on Amazon
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
5 Chair Exercises For Stronger Hips & Easier Walking
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sitting doesn’t have to be all bad:
Are you sitting comfortably?
Then we’ll begin:
- Seated march: sit tall in a firm chair, and lift your knees (alternating one and then the other and repeat), keeping your core engaged and avoiding leaning backwards; if needed, begin by lifting only your heels—this will still activate the fronts of your hips.
- Benefits: strengthens the hip flexors and core, helping with walking, taking larger steps, and overall hip function.
- Seated side step: sit near the edge of the chair, and move one knee and foot out to the side while keeping them aligned, then return to the starting position without letting your foot travel outside your knee. You can also put a resistance band above your knees, keeping light tension on the band throughout the movement, and continue stepping one leg out and back in under control.
- Benefits: improves inner-thigh mobility and strengthens the muscles on the sides of your hips that support walking, balance, and stair climbing.
- Pillow squeeze: put a pillow or ball between your knees, sit tall with your knees aligned over your ankles, gently squeeze the thing (whatever you chose), and then relax without letting your legs drift apart.
- Benefits: activates and strengthens your inner-thigh muscles while helping reduce feelings of groin and inner-thigh tightness.
- Heel push-down: sit near the edge of the chair with your knees bent, and press one heel firmly into the floor, feeling your glutes and the backs of your thighs contract before relaxing. You can also press both heels into the floor at the same time to create a stronger glute contraction while remaining seated.
- Benefits: strengthens your glutes and posterior hip muscles that assist with walking, climbing stairs, and general hip support.
- Straight leg raise: sit near the edge of the chair, straighten one leg with your toes pointing upwards, tighten your thigh by pressing your knee down, then lift and lower your leg slowly. If you need to make it easier, you can do a controlled kick-out instead of a full leg raise, or slide your heel forwards along the floor for additional support.
- Benefits: strengthens the fronts of your hips, your thighs, and your core, improving support for the front of the hip joint.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Stand Up For Your Health (Or Don’t) ← our main feature on this also includes more things you can do if you must sit, to make sitting less bad!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Seated march: sit tall in a firm chair, and lift your knees (alternating one and then the other and repeat), keeping your core engaged and avoiding leaning backwards; if needed, begin by lifting only your heels—this will still activate the fronts of your hips.