Licorice, Digestion, & Hormones
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s Take A Look At Licorice…
Licorice, as a confectionary, is mostly sugar and is useless for medicinal purposes.
Licorice (Glycyrrhiza sp., most often Glycyrrhiza glabra), in the form of either the root extract (which can be taken as a supplement, or used topically) or the whole root (which can be taken as a powder/capsule, or used to make tea), is a medicinal plant with a long history of use.
How well-evidenced is it for its popular uses?
Licorice for digestion
In this case, it is more accurate to say that it combats indigestion, including acid reflux and ulcerative colitis:
Systematic Review on Herbal Preparations for Controlling Visceral Hypersensitivity in Functional Gastrointestinal Disorders ← licorice was a top-tier performer in this review
Network pharmacology mechanisms and experimental verification of licorice in the treatment of ulcerative colitis ← looking at the mechanism of action; ultimately they concluded that “licorice improves ulcerative colitis, which may be related to the activation of the Nrf2/PINK1 signaling pathway that regulates autophagy.“
Licorice vs menopause symptoms
This one, while a popular use, isn’t so clear. Here’s a study that examines the compounds in licorice (in this case, Glycyrrhiza uralensis) that interact with estrogen receptors, notes that the bioavailability is poor, and proposes, tests, and recommends a way to make it more bioavailable:
On the other hand, it is established that it will lower serum testosterone levels, which may make it beneficial for menopause and/or PCOS:
Polycystic ovaries and herbal remedies: A systematic review
Licorice for men
You may be wondering: what about for men? Well, the jury is out on whether it meaningfully reduces free testosterone levels:
Licorice consumption and serum testosterone in healthy men
See also:
And finally, it may (notwithstanding its disputed effect on testosterone itself) be useful as a safer alternative to finasteride (an antiandrogen mostly commonly used to treat benign prostatic hyperplasia, also used to as a hair loss remedy), since it (like finasteride) modulates 5α-reductase activity (this enzyme converts testosterone to the more potent dihydrogen testosterone, DHT), without lowering sperm count:
Licorice for the skin
As well as its potentially estrogenic activity, its anti-inflammatory and antioxidant powers make it comparable to hydrocortisone cream for treating eczema, psoriasis, and other such skin conditions:
New Herbal Biomedicines for the Topical Treatment of Dermatological Disorders
Is it safe?
It is “generally recognized as safe”, as the classification goes.
However, consumed in excess it can cause/worsen hypertension, and other contraindications include if you’re on blood thinners, or have kidney problems.
As ever, this is a non-exhaustive list, so do speak with your doctor/pharmacist to be sure.
Want to try some?
We don’t sell it, but here for your convenience is an example product on Amazon
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Chili Hot-Bedded Salmon

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This one can be made in less time than it takes to order and receive a Chinese take-out! The principle is simple: it’s a bed of greens giving pride of place to a salmon fillet in a deliciously spicy marinade. So healthwise, we have greens-and-beans, healthy protein and fats, and tasty polyphenols. Experientially, we have food that tastes a lot more decadent than it is!
You will need
- 4 salmon fillets (if vegan, substitute firm tofu; see also how to make this no-salmon salmon)
- 2 bok choy, washed and stems trimmed
- 7 oz green beans, trimmed
- 4 oz sugar snap peas
- 4 spring onions, sliced
- 2 tbsp chili oil*
- 1 tbsp soy sauce
- 1 tsp garlic paste
- 1 tsp ginger paste
- 1 tsp black pepper
*this can be purchased as-is, but if you want to make your own in advance, simply take extra virgin olive oil and infuse it with [finely chopped, red] chili. This is a really good thing to do for commonly-used flavored oils, by the way—chili oil and garlic oil are must-haves in this writer’s opinion; basil oil, sage oil, and rosemary oil, are all excellent things to make and have in, too. Just know, infusing is not quick, so it’s good to do these in batch and make plenty well before you need it. For now, if you don’t have any homemade already, then store-bought is fine 🙂
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 360℉/180℃/gas mark 6
2) Lay out 4 large squares of foil, and put the bok choy, green beans, and sugar snap peas in a little pile in the middle of each one. Put a salmon fillet on top of each (if it has skin, score the skin first, so that juices will be able to penetrate, and put it skin-side down), and then top with the spring onions.
3) Mix the rest of the ingredients in a small bowl, and then spoon this marinade evenly over each of the fillets (alternatively, if you have occasion to marinade the fillets in advance and let them sit in the marinade in the fridge for some hours before, do so, in which case this step will already be done now, because past-you did it. Yay for past-you!)
4) Fold up the edges of the foil, making each one an enclosed parcel, gently sealed at the top by folding it over. Put them on a baking tray and bake for about 20 minutes.
5) Serve! If you’d like some carbs with it, we recommend our tasty versatile rice recipe.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- We Are Such Stuff As Fish Are Made Of
- Farmed Fish vs Wild-Caught ← don’t underestimate the difference this makes!
- Tasty Polyphenols For Your Heart And Brain
- Brain Food? The Eyes Have It!
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Share This Post
-

What’s the difference between vegan and vegetarian?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
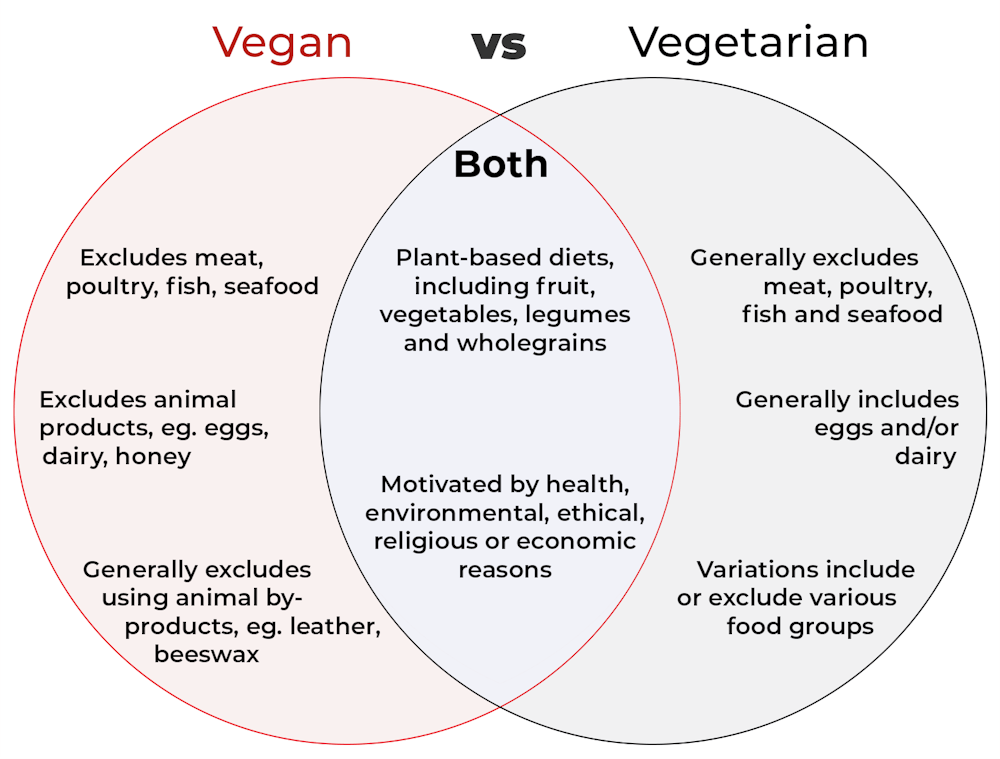
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?
Creative Cat Studio/Shutterstock What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.
More than a diet: veganism can form part of someone’s identity. Shutterstock So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Peace Is Every Step – by Thích Nhất Hạnh
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Mindfulness is one of the few practices to make its way from religion (in this case, Buddhism) into hard science. We’ve written before about its many evidence-based benefits, and many national health information outlets recommend it. So, what does this book have to add?
Thích Nhất Hạnh spent most of his 95 years devoted to the practice and teaching of mindfulness and compassion. In this book, the focus is on bringing mindfulness off the meditation mat and into general life.
After all, what if we could extend that “unflappability” into situations that pressure and antagonize us? That would be some superpower!
The author offers techniques to do just that, simple exercises to transform negative emotions, and to make us more likely to remember to do so.
After all, “in the heat of the moment” is rarely when many of us are at our best, this book gives way to allow those moments themselves to serve as immediate triggers to be our best.
The title “Peace Is Every Step” is not a random collection of words; the goal of this book is to enable to reader to indeed carry peace with us as we go.
Not just “peace is always available to us”, but if we do it right: “we have now arranged for our own peace to automatically step in and help us when we need it most”.
Bottom line: if you’d like to practice mindfulness, or practice it more consistently, this book offers some powerful tools.
Click here to check out Peace Is Every Step, and carry yours with you!
Share This Post



Related Posts
-

This Is When Your Muscles Are Strongest
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Karyn Esser is a professor in the Department of Physiology and Aging at the University of Florida, where she’s also the co-director of the University of Florida Older Americans Independence Center, and she has insights to share on when it’s best to exercise:
It’s 4–5pm
Surprise, no clickbait or burying the lede!
This goes regardless of age or sex, but as we get older, it’s common for our circadian rhythm to weaken, which may result in a tendency to fluctuate a bit more.
However, since it’s healthy to keep one’s circadian rhythm as stable as reasonably possible, this is a good reason to try to keep our main exercise focused around that time of day, as it provides a sort of “anchor point” for the rest of our day to attach to, so that our body can know what time it is relative to that.
It’s also the most useful time of day to exercise, because most exercises give benefits proportional to progressive overloading, so training at our peak efficiency time will give the most efficient results. So much for those 5am runs!
On which note: while the title says “strongest” and the thumbnail has dumbbells, this does go for all different types of exercises that have been tested.
For more details on all of the above, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The Circadian Rhythm: Far More Than Most People Know
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
You could be stress eating these holidays – or eating your way to stress. 5 tips for the table
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The holiday season can be a time of joy, celebration, and indulgence in delicious foods and meals. However, for many, it can also be an emotional and stressful period.
This stress can manifest in our eating habits, leading to what is known as emotional or stress eating.
There are certain foods we tend to eat more of when we’re stressed, and these can affect our health. What’s more, our food choices can influence our stress levels and make us feel worse. Here’s how.
Dean Clarke/Shutterstock Why we might eat more when stressed
The human stress response is a complex signalling network across the body and brain. Our nervous system then responds to physical and psychological events to maintain our health. Our stress response – which can be subtle or trigger a fight-or-flight response – is essential and part of daily life.
The stress response increases production of the hormones cortisol and insulin and the release of glucose (blood sugars) and brain chemicals to meet demand. Eating when we experience stress is a normal behaviour to meet a spike in energy needs.
But sometimes our relationship with food becomes strained in response to different types of stress. We might attach shame or guilt to overeating. And anxiety or insecurity can mean some people under-eat in stressful times.
Over time, people can start to associate eating with negative emotions – such as anger, sadness, fear or worry. This link can create behavioural cycles of emotional eating. “Emotional eaters” may go on to develop altered brain responses to the sight or smell of food.
What stress eating can do to the body
Stress eating can include binge eating, grazing, eating late at night, eating quickly or eating past the feeling of fullness. It can also involve craving or eating foods we don’t normally choose. For example, stressed people often reach for ultra-processed foods. While eating these foods is not necessarily a sign of stress, having them can activate the reward system in our brain to alleviate stress and create a pattern.
Short-term stress eating, such as across the holiday period, can lead to symptoms such as acid reflux and poor sleep – particularly when combined with drinking alcohol.
In the longer term, stress eating can lead to weight gain and obesity, increasing the risks of cancer, heart diseases and diabetes.
While stress eating may help reduce stress in the moment, long-term stress eating is linked with an increase in depressive symptoms and poor mental health.
If you do over eat at a big gathering, don’t try and compensate by eating very little the next day. Peopleimage.com – Yuri A/Shutterstock What we eat can make us more or less stressed
The foods we choose can also influence our stress levels.
Diets high in refined carbohydrates and sugar (such as sugary drinks, sweets, crackers, cakes and most chocolates) can make blood sugar levels spike and then crash.
Diets high in unhealthy saturated and trans fats (processed foods, animal fats and commercially fried foods) can increase inflammatory responses.
Rapid changes in blood sugar and inflammation can increase anxiety and can change our mood.
Meanwhile, certain foods can improve the balance of neurotransmitters in the brain that regulate stress and mood.
Omega-3 fatty acids, found in fish and flaxseeds, are known to reduce inflammation and support brain health. Magnesium, found in leafy greens and nuts, helps regulate cortisol levels and the body’s stress response.
Vitamin Bs, found in whole grains, nuts, seeds, beans and animal products (mostly B12), help maintain a healthy nervous system and energy metabolism, improving mood and cognitive performance.
5 tips for the holiday table and beyond
Food is a big part of the festive season, and treating yourself to delicious treats can be part of the fun. Here are some tips for enjoying festive foods, while avoiding stress eating:
1. slow down: be mindful about the speed of your eating. Slow down, chew food well and put down your utensils after each bite
2. watch the clock: even if you’re eating more food than you normally would, sticking to the same timing of eating can help maintain your body’s response to the food. If you normally have an eight-hour eating window (the time between your first meal and last meal of the day) then stick to this even if you’re eating more
3. continue other health behaviours: even if we are eating more food or different food during the festive season, try to keep up other healthy behaviours, such as sleep and exercise
4. stay hydrated: make sure to drink plenty of fluids, especially water. This helps our body function and can help with feelings of hunger. When our brain gets the message something has entered the stomach (what we drink) this can provide a temporary reduction in feelings of hunger
5. don’t restrict: if we have a big day of eating, it can be tempting to restrict eating in the days before or after. But it is never a good idea to overly constrain food intake. It can lead to more overeating and worsen stress.
Reaching for cookies late at night can be characteristic of stress eating. Stokkete/Shutterstock Plus 3 bonus tips to manage holiday stress
1. shift your thinking: try reframing festive stress. Instead of viewing it as “something bad”, see it as “providing the energy” to reach your goals, such as a family gathering or present shopping
2. be kind to yourself and others: practise an act of compassion for someone else or try talking to yourself as you would a friend. These actions can stimulate our brains and improve wellbeing
3. do something enjoyable: being absorbed in enjoyable activities – such as crafting, movement or even breathing exercises – can help our brains and bodies to return to a more relaxed state, feel steady and connected.
For support and more information about eating disorders, contact the Butterfly Foundation on 1800 33 4673 or Kids Helpline on 1800 551 800. If this article has raised issues for you, or if you’re concerned about someone you know, call Lifeline on 13 11 14. In an emergency, call 000.
Saman Khalesi, Senior Lecturer and Discipline Lead in Nutrition, School of Health, Medical and Applied Sciences, CQUniversity Australia; Charlotte Gupta, Senior Postdoctoral Research Fellow, Appleton Institute, HealthWise research group, CQUniversity Australia, and Talitha Best, Professor of Psychology, NeuroHealth Lab, Appleton Institute, CQUniversity Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
One More Reason To Prioritize Sleep To Fight Cognitive Decline
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve talked sometimes at 10almonds about how important sleep is for many aspects of health, including for brain health, and including in later life.
There’s a common myth that older people require less sleep; the reality is that sleeping less and not dying of it does not equate to needing less.
See also: Sleep: Yes, You Really Do Still Need It!
And: How Sleep-Deprived Are You, Really?
Quantity is not everything though; quality absolutely matters too. We’ve written about that here:
The 6 Dimensions Of Sleep (And Why They Matter) ← duration is just one dimension out of the six
We’ve even gone into some more obscure, but still very important things, such as: How Your Sleep Position Changes Dementia Risk
We’ve also talked about the role of sleep in memory (and forgetting): How Your Brain Chooses What To Remember
With that in mind…
Some more recent science
This study was about spatial memory, but what’s important (in our opinion) is that it’s about solidifying recent learning.
Researchers measured brain activity in rats for up to 20 hours of sleep following spatial learning tasks. Initially, the neuronal patterns observed during sleep mirrored those from the learning phase. However, as sleep progressed, these patterns transformed to resemble the activity seen when the rats later recalled the locations of food rewards. Interestingly, this reorganization happened during non-REM sleep, which means it wasn’t just a case of “the rats were dreaming about their day” (which is a well-established way in which memories do get encoded), but rather, the newly-learned experiences were being actively encoded in the rest of sleep.
This is critical, because in age-related cognitive decline, it’s very common for very long-term memory (VLTM) to remain intact, while LTM and short-term memory (STM) crumble. For example, someone may remember many details of their life from 20 years ago, but forget where they currently live, or what happened in the conversation two minutes ago.
In other words, the biggest problem is not the storage of memories, but rather the encoding of them in the first place.
Which sleep facilitates!
And it’s also important to note that part about it being the rest of sleep, because when the brain is sleep-deprived, it’ll tend to prioritize REM sleep, which is important, but that means cutting back on other phases of sleep, and from this study, we can see that memory & learning will be amongst the things adversely affected by such cuts.
Here’s the paper, for those interested:
Sleep stages antagonistically modulate reactivation drift
And for those who prefer lighter reading, here’s a pop-science article about the same study, which explains it in more words than we can here:
But wait, there’s more!
Sleep resets neurons for new memories the next day, study finds
So, once again… It is absolutely critical to prioritize good sleep.
Want to know more?
Check out:
Calculate (And Enjoy) The Perfect Night’s Sleep
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: