Is There A Limit To How Much You Can Improve Your Brain?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There’s a popular myth that our brains finish developing at 25 (not remotely true) and from then on, stays pretty much the same with no new growth (also not true), and in terms of cognitive performance, the only way is down (have a guess whether this is true).
If you guessed “no”, you guessed correctly!
The first two myths we’ve previous covered here: Building Your Brain At Every Age
And for more about the terribly misrepresented study that inadvertently launched the “brain finishes developing at 25” myth, see: The Brain As A Work-In-Progress
So, what about cognitive performance?
Limitless?
Researchers (Dr. Lori Cook et al.) set about this question, by means of a large (n=3,966) and exciting 3-year longitudinal study with adults of all ages (well, 19–94), using the BrainHealth Index (BHI), a first-of-its-kind multidimensional metric that measures holistic brain fitness.
They gave these participants a comprehensive set of brain-healthy practices to do, and then measured to see if there would be improvements, and if so, how much and for whom and what factors affected it.
In few words, they found:
- No ceiling on improvement: significant gains in brain health were observed across the board. Even top-tier performers continued to improve over 1,000 days, suggesting there is no known limit to brain optimization.
- Advantage for “low-starters”: participants who entered the study with the lowest baseline scores demonstrated the most significant rates of improvement, demonstrating that poor brain health is not a life sentence.
- Small habit changes; big difference: gains were directly correlated with consistency of utilization. Participants who engaged the most in 5 to 15 minutes of daily micro-training and adopted brain-healthy habits in their everyday lives achieved the highest brain health scores.
- Age was not an issue: young and old participants alike enjoyed similar brain gains!
…which is really quite groundbreaking! And as one of the researchers put it:
❝For too long, we’ve operated under the outdated notion that we need to wait until something bad happens to our brain before we do anything for it. This study reminds us that our brain is not defined by age, it is defined by possibility. Humans have already expanded how long we live. Now, we are expanding how long the brain can continue to improve, disrupting the trajectory of decline that often begins in our early 30s. Because the true promise of longer life is a brain that allows us to thrive year by year.❞
~ Dr. Sandra Chapman, whose work we featured in our article: How (And Why) To Train Your Pre-Frontal Cortex
…and who was also a co-author on the study we’ve been talking about today, which study you can read in full here: Measuring and increasing the brain health span across adulthood: a public health imperative ← you will need to click on the PDF option to read it in full, otherwise it’s just the abstract on the page
Want to learn more?
As for how to do it for yourself, consider:
- Do Try This At Home: The 12-Week Brain Fitness Program
- Synergistic Brain-Training
- The Physical Exercises That Build Your Brain
- Sharper Minder & Body In 3 Weeks With 1 Supplement
- Seven Exercises To Strengthen Your Brain
- Ways To Boost Brain-Derived Neurotrophic Factor (BDNF)
- Reading As A Cognitive Exercise ← there are specific tips here for ensuring your reading is (and remains) cognitively beneficial
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Hospitals worldwide are short of saline. We can’t just switch to other IV fluids – here’s why

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Last week, the Australian Therapeutic Goods Administration added intravenous (IV) fluids to the growing list of medicines in short supply. The shortage is due to higher-than-expected demand and manufacturing issues.
Two particular IV fluids are affected: saline and compound sodium lactate (also called Hartmann’s solution). Both fluids are made with salts.
There are IV fluids that use other components, such as sugar, rather than salt. But instead of switching patients to those fluids, the government has chosen to approve salt-based solutions by other overseas brands.
So why do IV fluids contain different chemicals? And why can’t they just be interchanged when one runs low?

Pavel Kosolapov/Shutterstock We can’t just inject water into a vein
Drugs are always injected into veins in a water-based solution. But we can’t do this with pure water, we need to add other chemicals. That’s because of a scientific principle called osmosis.
Osmosis occurs when water moves rapidly in and out of the cells in the blood stream, in response to changes to the concentration of chemicals dissolved in the blood plasma. Think salts, sugars, nutrients, drugs and proteins.
Too high a concentration of chemicals and protein in your blood stream leads it to being in a “hypertonic” state, which causes your blood cells to shrink. Not enough chemicals and proteins in your blood stream causes your blood cells to expand. Just the right amount is called “isotonic”.
Mixing the drug with the right amount of chemicals, via an injection or infusion, ensures the concentration inside the syringe or IV bag remains close to isotonic.
Australia is currently short on two salt-based IV fluids. sirnength88/Shutterstock What are the different types of IV fluids?
There are a range of IV fluids available to administer drugs. The two most popular are:
- 0.9% saline, which is an isotonic solution of table salt. This is one of the IV fluids in short supply
- a 5% solution of the sugar glucose/dextrose. This fluid is not in short supply.
There are also IV fluids that combine both saline and glucose, and IV fluids that have other salts:
- Ringer’s solution is an IV fluid which has sodium, potassium and calcium salts
- Plasma-Lyte has different sodium salts, as well as magnesium
- Hartmann’s solution (compound sodium lactate) contains a range of different salts. It is generally used to treat a condition called metabolic acidosis, where patients have increased acid in their blood stream. This is in short supply.
What if you use the wrong solution?
Some drugs are only stable in specific IV fluids, for instance, only in salt-based IV fluids or only in glucose.
Putting a drug into the wrong IV fluid can potentially cause the drug to “crash out” of the solution, meaning patients won’t get the full dose.
Or it could cause the drug to decompose: not only will it not work, but it could also cause serious side effects.
An example of where a drug can be transformed into something toxic is the cancer chemotherapy drug cisplatin. When administered in saline it is safe, but administration in pure glucose can cause life-threatening damage to a patients’ kidneys.
What can hospitals use instead?
The IV fluids in short supply are saline and Hartmann’s solution. They are provided by three approved Australian suppliers: Baxter Healthcare, B.Braun and Fresenius Kabi.
The government’s solution to this is to approve multiple overseas-registered alternative saline brands, which they are allowed to do under current legislation without it going through the normal Australian quality checks and approval process. They will have received approval in their country of manufacture.
The government is taking this approach because it may not be effective or safe to formulate medicines that are meant to be in saline into different IV fluids. And we don’t have sufficient capacity to manufacture saline IV fluids here in Australia.
The Australian Society of Hospital Pharmacists provides guidance to other health staff about what drugs have to go with which IV fluids in their Australian Injectable Drugs Handbook. If there is a shortage of saline or Hartmann’s solution, and shipments of other overseas brands have not arrived, this guidance can be used to select another appropriate IV fluid.
Why don’t we make it locally?
The current shortage of IV fluids is just another example of the problems Australia faces when it is almost completely reliant on its critical medicines from overseas manufacturers.
Fortunately, we have workarounds to address the current shortage. But Australia is likely to face ongoing shortages, not only for IV fluids but for any medicines that we rely on overseas manufacturers to produce. Shortages like this put Australian lives at risk.
In the past both myself, and others, have called for the federal government to develop or back the development of medicines manufacturing in Australia. This could involve manufacturing off-patent medicines with an emphasis on those medicines most used in Australia.
Not only would this create stable, high technology jobs in Australia, it would also contribute to our economy and make us less susceptible to future global drug supply problems.
Nial Wheate, Professor and Director Academic Excellence, Macquarie University and Shoohb Alassadi, Casual academic, pharmaceutical sciences, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

What’s the difference between freckles, sunspots and moles?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You’ve got a new brown spot on your face, but is it a freckle or a sunspot? Or perhaps you’ve found a spot on your back that looks like a mole but is flatter than your other ones – is it a mole or a dark freckle?
Here’s how to tell the difference between freckles, sunspots and moles – and when you need to get a spot checked to see if it’s skin cancer.
Cottonbro Studio/Pexels Freckles
Freckles, known as ephelides, are small, flat, light brown spots that appear on people with fair skin, or red or light-coloured hair.
These people are more likely to have the MC1R gene, which leads to freckles forming.
Freckles are caused by sun exposure and are more noticeable in summer. When sunlight hits the skin, cells called melanocytes produce melanin, the pigment that gives skin its colour.
In people prone to freckles, the melanin doesn’t spread evenly. Instead, it clumps together, creating freckles.
Melanin doesn’t spread evenly in people prone to freckles. Chermiti Mohamed/Unsplash Freckles generally appear in childhood and may fade with age, especially if sun exposure reduces. As we age we produce less melanin, or it can break down or disperse, resulting in lighter or fewer freckles.
Using sunscreen and wearing protective clothing can help prevent new freckles from developing, especially on the face and arms.
While freckles are completely harmless, they are a sign that someone is genetically at higher risk of developing skin cancer.
Sunspots
Sunspots are also called age spots or solar lentigos (or liver spots, but they have nothing to do with the liver). They are larger than freckles: sometimes the size of a small coin, and appear as flat brown spots.
Sunspots develop over time due to long-term sun exposure, which leads to excessive melanin production. They tend to appear on skin with greater sun exposure, such as the face, hands, shoulders and arms.
Sunspots develop after years of sun exposure. Zay Nyi Nyi/Shutterstock Unlike freckles, which tend to get lighter with less sun exposure, sunspots will not fade with time, and may further darken with continued sun exposure.
However, some people try to remove their sunspots for cosmetic reasons using either a laser, chemical peel or a prescription topical cream.
While sunspots are not dangerous, they do increase your risk of other skin cancers in that area.
It’s also important to monitor them, as slow-growing melanomas may initially look like sunspots. If you see the spot changes in size, shape or colour, see your doctor to rule out skin cancer.
Moles
Moles are often dark, raised or flat skin growths that can appear anywhere on your body.
Although moles can exist from birth, they typically grow during childhood, adolescence and early adulthood (including during pregnancy, when hormones are changing), until around the age of around 40. Moles can increase in size, and new ones can also appear.
Most adults have between ten and 40 moles on their body. A person with a high mole count has 50 or more, while someone with a very high mole count has 100 or more.
Some moles are raised while others are flat. Pixel-Shot/Shutterstock Moles form when melanocytes grow in clusters instead of spreading evenly throughout the skin.
Moles can either be raised or flat, depending upon their type, depth and age.
Raised moles, referred to as compound nevi, have both flat and raised portions and typically have pigment that is deeper in the skin.
Dermal nevi are skin-coloured or light brown moles that are also raised.
Most moles are harmless. Some may have hair growing from them and some may disappear, whereas other moles may darken or alter with age or hormonal changes.
However, some moles can develop into melanoma, a dangerous form of skin cancer.
When to see your doctor
While freckles and sunspots are completely harmless, moles do require more attention, especially if they change in size, shape, colour or texture.
If a mole shows any of the following warning signs, see your doctor, who will use the ABCDE rule to detect if a lesion is a skin cancer:
- asymmetry: if one half of the mole looks different from the other half
- border: if your mole is shaped irregularly, jagged or has poorly defined edges
- colour: varied shades or sudden changes in colour of the mole
- diameter: if it is larger than 6 millimeters (about the size of a pencil eraser)
- evolving: if your mole has any changes in its size, shape, colour, or sensation such as itching or bleeding for more than a few weeks.
Our research shows only 21.7% of people can correctly identify melanoma on their own, so professional checks are essential.
How to prevent skin damage
Since freckles, sunspots and some moles are influenced by exposure to the sun, you can protect your skin by:
- avoiding the sun when ultraviolet rays are strongest
- wearing sunscreen with SPF 50 every day, even when it’s cloudy. Apply it 20 minutes before going outside and reapply every two hours
- wearing protective clothing, including a wide-brimmed hat to cover your face, neck and ears, and long-sleeved shirts and pants to protect your arms and legs.
Correction: this article originally referred to sun sports as actinic keratoses rather than solar lentigos.
Mike Climstein, Associate Professor, Faculty of Health, Southern Cross University; Jeremy Hudson, Adjunct Associate Professor, Faculty of Health, Southern Cross University; Michael Stapelberg, Adjunct Associate Professor, Faculty of Health, Southern Cross University, and Nedeljka Rosic, Senior Lecturer, Faculty of Health, Southern Cross University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Montana Eyes $30M Revamp of Mental Health, Developmental Disability Facilities
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
HELENA, Mont. — As part of a proposed revamping of the state’s behavioral health system, Republican Gov. Greg Gianforte’s administration is looking into moving a facility for people with developmental disabilities, beefing up renovations at the Montana State Hospital, and creating a Helena unit of that psychiatric hospital.
The changes, backers say, would fill gaps in services and help people better prepare for life outside of the locked, secure setting of the two state facilities before they reenter their own communities.
“I think part of the theme is responsibly moving people in and out of the state facilities so that we create capacity and have people in the appropriate places,” state Sen. Dave Fern (D-Whitefish) said of the proposed capital projects during a recent interview.
Fern served on the Behavioral Health System for Future Generations Commission, a panel created by a 2023 law to suggest how to spend $300 million to revamp the system. The law set aside the $300 million for improving state services for people with mental illness, substance abuse disorders, and developmental disabilities.
Gianforte’s proposed budget for the next two years would spend about $100 million of that fund on 10 other recommendations from the commission. The capital projects are separate ideas for using up to $32.5 million of the $75 million earmarked within the $300 million pool of funds for building new infrastructure or remodeling existing buildings.
The state Department of Public Health and Human Services and consultants for the behavioral health commission presented commission members with areas for capital investments in October. In December, the commission authorized state health department director Charlie Brereton to recommend the following projects to Gianforte:
- Move the 12-bed Intensive Behavior Center for people with developmental disabilities out of Boulder, possibly to either Helena or Butte, at an estimated cost of up to $13.3 million.
- Establish a “step-down” facility of about 16 beds, possibly on the campus of Shodair Children’s Hospital in Helena, to serve adults who have been committed to the Montana State Hospital but no longer need the hospital’s intensive psychiatric services.
- Invest $19.2 million to upgrade the Montana State Hospital’s infrastructure and buildings at Warm Springs, on top of nearly $16 million appropriated in 2023 for renovations already underway there in an effort to regain federal certification of the facility.
The state Architecture & Engineering Division is reviewing the health department’s cost estimates and developing a timeline for the projects so the information can be sent to the governor. Gianforte ultimately must approve the projects.
Health department officials have said they plan to take the proposals to legislative committees as needed. “With Commission recommendation and approval from the governor, the Department believes that it has the authority to proceed with capital project expenditures but must secure additional authority from the Legislature to fund operations into future biennia,” said department spokesperson Jon Ebelt.
The department outlined its facility plans to the legislature’s health and human services budget subcommittee on Jan. 22 as part of a larger presentation on the commission’s work and the 10 noncapital proposals in the governor’s budget. Time limits prevented in-depth discussion and public comment on the facility-related ideas.
One change the commission didn’t consider: moving the Montana State Hospital to a more populated area from its rural and relatively remote location near Anaconda, in southwestern Montana, in an attempt to alleviate staffing shortages.
“The administration is committed to continuing to invest in MSH as it exists today,” Brereton told the commission in October, referring to the Montana State Hospital.
The hospital provides treatment to people with mental illness who have been committed to the state’s custody through a civil or criminal proceeding. It’s been beset by problems, including the loss of federal Medicaid and Medicare funding due to decertification by the federal government in April 2022, staffing issues that have led to high use of expensive traveling health care providers, and turnover in leadership.
State Sen. Chris Pope (D-Bozeman) was vice chair of a separate committee that met between the 2023 and 2025 legislative sessions and monitored progress toward a 2023 legislative mandate to transition patients with dementia out of the state hospital. He agreed in a recent interview that improving — not moving — MSH is a top priority for the system right now.
“Right now, we have an institution that is failing and needs to be brought back into the modern age, where it is located right now,” he said after ticking off a list of challenges facing the hospital.
State Sen. John Esp (R-Big Timber) also noted at the October commission meeting that moving the hospital was likely to run into resistance in any community considered for a new facility.
Fern, the Whitefish senator, questioned in October whether similar concerns might exist for moving the Intensive Behavior Center out of Boulder. For more than 130 years, the town 30 miles south of Helena has been home, in one form or another, to a state facility for people with developmental disabilities. But Brereton said he believes relocation could succeed with community and stakeholder involvement.
The 12-bed center in Boulder serves people who have been committed by a court because their behaviors pose an immediate risk of serious harm to themselves or others. It’s the last residential building for people with developmental disabilities on the campus of the former Montana Developmental Center, which the legislature voted in 2015 to close.
Drew Smith, a consultant with the firm Alvarez & Marsal, told the commission in October that moving the facility from the town of 1,300 to a bigger city such as Helena or Butte would provide access to a larger labor pool, possibly allow a more homelike setting for residents, and open more opportunities for residents to interact with the community and develop skills for returning to their own communities.
Ideally, Brereton said, the center would be colocated with a new facility included in the governor’s proposed budget, for crisis stabilization services to people with developmental disabilities who are experiencing significant behavioral health issues.
Meanwhile, the proposed subacute facility with up to 16 beds for state hospital patients would provide a still secure but less structured setting for people who no longer need intensive treatment at Warm Springs but aren’t yet ready to be discharged from the hospital’s care. Brereton told the commission in October the facility would essentially serve as a less restrictive “extension” of the state hospital. He also said the agency would like to contract with a company to staff the subacute facility.
Health department officials don’t expect the new facility to involve any construction costs. Brereton has said the agency believes an existing building on the Shodair campus would be a good spot for it.
The state began leasing the building Nov. 1 for use by about 20 state hospital patients displaced by the current remodeling at Warm Springs — a different purpose than the proposed subacute facility.
Shodair CEO Craig Aasved said Shodair hasn’t committed to having the state permanently use the building as the step-down facility envisioned by the agency and the commission.
But Brereton said the option is attractive to the health department now that the building has been set up and licensed to serve adults.
“It seems like a natural place to start,” he told the commission in December, “and we don’t mind that it’s in our backyard here in Helena.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post







Related Posts
-

Zuranolone: What to know about the pill for postpartum depression
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In the year after giving birth, about one in eight people who give birth in the U.S. experience the debilitating symptoms of postpartum depression (PPD), including lack of energy and feeling sad, anxious, hopeless, and overwhelmed.
Postpartum depression is a serious, potentially life-threatening condition that can affect a person’s bond with their baby. Although it’s frequently confused with the so-called “baby blues,” it’s not the same.
The baby blues include similar, temporary symptoms that affect up to 80 percent of people who have recently given birth and usually go away within the first few weeks. PPD usually begins within the first month after giving birth and can last for months and interfere with a person’s daily life if left untreated. Thankfully, PPD is treatable and there is help available.
On August 4, the FDA approved zuranolone, branded as Zurzuvae, the first-ever oral medication to treat PPD. Until now, besides other common antidepressants, the only medication available to treat PPD specifically was the IV injection brexanolone, which is difficult to access and expensive and can only be administered in a hospital or health care setting.
Read on to find out more about zuranolone: what it is, how it works, how much it costs, and more.
What is zuranolone?
Zurzuvae is the brand name for zuranolone, an oral medication to treat postpartum depression. Developed by Sage Therapeutics in partnership with Biogen, it’s now available in the U.S. Zurzuvae is typically prescribed as two 25 mg capsules a day for 14 days. In clinical trials, the medication showed to be fast-acting, improving PPD symptoms in just three days.
How does zuranolone work?
Zuranolone is a neuroactive steroid, a type of medication that helps the neurotransmitter GABA’s receptors, which affect how the body reacts to anxiety, stress, and fear, function better.
“Zuranolone can be thought of as a synthetic version of [the neuroactive steroid] allopregnanolone,” says Dr. Katrina Furey, a reproductive psychiatrist, clinical instructor at Yale University, and co-host of the Analyze Scripts podcast. “Women with PPD have lower levels of allopregnenolone compared to women without PPD.”
How is it different from other antidepressants?
“What differentiates zuranolone from other previously available oral antidepressants is that it has a much more rapid response and a shorter course of treatment,” says Dr. Asima Ahmad, an OB-GYN, reproductive endocrinologist, and founder of Carrot Fertility.
“It can take effect as early as on day three of treatment, versus other oral antidepressants that can take up to six to 12 weeks to take full effect.”
What are Zurzuvae’s side effects?
According to the FDA, the most common side effects of Zurzuvae include dizziness, drowsiness, diarrhea, fatigue, the common cold, and urinary tract infection. Similar to other antidepressants, the medication may increase the risk of suicidal thoughts and actions in people 24 and younger. However, NPR noted that this type of labeling is required for all antidepressants, and researchers didn’t see any reports of suicidal thoughts in their trials.
“Drug trials also noted that the side effects for zuranolone were not as severe,” says Ahmad. “[There was] no sudden loss of consciousness as seen with brexanolone or weight gain and sexual dysfunction, which can be seen with other oral antidepressants.”
She adds: “Given the lower incidence of side effects and more rapid-acting onset, zuranolone could be a viable option for many,” including those looking for a treatment that offers faster symptom relief.
Can someone breastfeed while taking zuranolone?
It’s complicated. In clinical trials, participants were asked to stop breastfeeding (which, according to Furey, is common in early clinical trials).
A small study of people who were nursing while taking zuranolone found that 0.3 percent of the medication dose was passed on to breast milk, which, Furey says, is a pretty low amount of exposure for the baby. Ahmad says that “though some data suggests that the risk of harm to the baby may be low, there is still overall limited data.”
Overall, people should talk to their health care provider about the risks and benefits of breastfeeding while on the medication.
“A lot of factors will need to be weighed, such as overall health of the infant, age of the infant, etc., when making this decision,” Furey says.
How much does Zurzuvae cost?
Zurzuvae’s price before insurance coverage is $15,900 for the 14-day treatment. However, the Policy Center for Maternal Mental Health says insurance companies and Medicaid are expected to cover it because it’s the only drug of its kind.
Less than 1 percent of U.S. insurers have issued coverage guidelines so far, so it’s still unknown how much it will cost patients after insurance. Some insurers require patients to try another antidepressant first (like the more common SSRIs) before covering Zurzuvae. For uninsured and underinsured people, Sage Therapeutics said it will offer copay assistance.
The hefty price tag and potential issues with coverage may widen existing health disparities, says Ahmad. “We need to ensure that we are seeking out solutions to enable wide-scale access to all PPD treatments so that people have access to whatever treatment may work best for them.”
If you or anyone you know is considering suicide or self-harm or is anxious, depressed, upset, or needs to talk, call the Suicide & Crisis Lifeline at 988 or text the Crisis Text Line at 741-741. For international resources, here is a good place to begin.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Ozempic’s cousin drug liraglutide is about to get cheaper. But how does it stack up?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
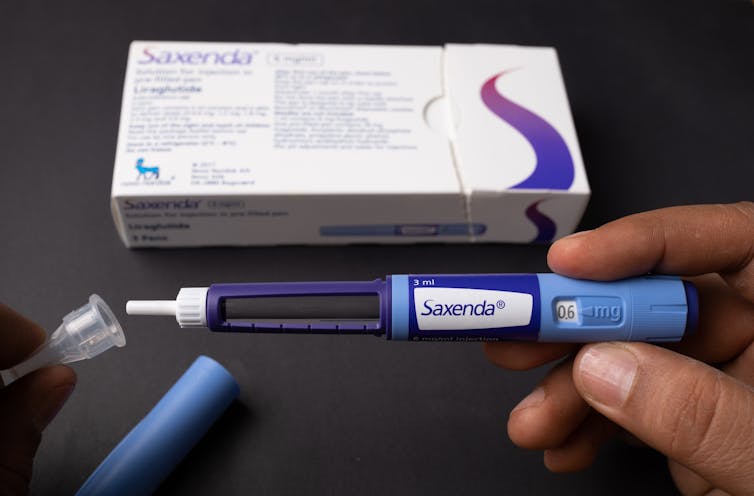
Fourteen years ago, the older drug cousin of semaglutide (Ozempic and Wegovy) came onto the market. The drug, liraglutide, is sold under the brand names Victoza and Saxenda.
Patents for Victoza and Saxenda have now expried. So other drug companies are working to develop “generic” versions. These are likely be a fraction of current cost, which is around A$400 a month.
So how does liraglutide compare with semaglutide?
Halfpoint/Shutterstock How do these drugs work?
Liraglutide was not originally developed as a weight-loss treatment. Like semaglutide (Ozempic), it originally treated type 2 diabetes.
The class of drugs liraglutide and semaglutide belong to are known as GLP-1 mimetics, meaning they mimic the natural hormone GLP-1. This hormone is released from your small intestines in response to food and acts in several ways to improve the way your body handles glucose (sugar).
How do they stop hunger?
Liraglutide acts in several regions of the unconscious part of your brain, specifically the hypothalamus, which controls metabolism, and parts of the brain stem responsible for communicating your body’s nutrient status to the hypothalamus.
Its actions here appear to reduce hunger in two different ways. First, it helps you to feel full earlier, making smaller meals more satisfying. Second, it alters your “motivational salience” towards food, meaning it reduces the amount of food you seek out.
Liraglutide’s original formulation, designed to treat type 2 diabetes, was marketed as Victoza. Its ability to cause weight loss was evident soon after it entered the market.
Shortly after, a stronger formulation, called Saxenda, was released, which was intended for weight loss in people with obesity.
How much weight can you lose with liraglutide?
People respond differently and will lose different amounts of weight. But here, we’ll note the average weight loss users can expect. Some will lose more (sometimes much more), others will lose less, and a small proportion won’t respond.
The first GLP-1 mimicking drug was exenatide (Bayetta). It’s still available for treating type 2 diabetes, but there are currently no generics. Exenatide does provide some weight loss, but this is quite modest, typically around 3-5% of body weight.
For liraglutide, those using the drug to treat obesity will use the stronger one (Saxenda), which typically gives about 10% weight loss.
Semaglutide, with the stronger formulation called Wegovy, typically results in 15% weight loss.
The newest GLP-1 mimicking drug on the market, tirzepatide (Mounjaro for type 2 diabetes and Zepbound for weight loss), results in weight loss of around 25% of body weight.
What happens when you stop taking them?
Despite the effectiveness of these medications in helping with weight loss, they do not appear to change people’s weight set-point.
So in many cases, when people stop taking them, they experience a rebound toward their original weight.
People often regain weight when when they stop taking the drug. Mohammed_Al_Ali/Shutterstock What is the dose and how often do you need to take it?
Liraglutide (Victoza) for type 2 diabetes is exactly the same drug as Saxenda for weight loss, but Saxenda is a higher dose.
Although the target for each formulation is the same (the GLP-1 receptor), for glucose control in type 2 diabetes, liraglutide has to (mainly) reach the pancreas.
But to achieve weight loss, it has to reach parts of the brain. This means crossing the blood-brain barrier – and not all of it makes it, meaning more has to be taken.
All the current formulations of GLP-1 mimicking drug are injectables. This won’t change when liraglutide generics hit the market.
However, they differ in how frequently they need to be injected. Liraglutide is a once-daily injection, whereas semaglutide and tirzepatide are once-weekly. (That makes semaglutide and tirzepatide much more attractive, but we won’t see semaglutide as a generic until 2033.)
What are the side effects?
Because all these medicines have the same target in the body, they mostly have the same side effects.
The most common are a range of gastrointestinal upsets including nausea, vomiting, bloating, constipation and diarrhoea. These occur, in part, because these medications slow the movement of food out of the stomach, but are generally managed by increasing the dose slowly.
Recent clinical data suggests the slowing in emptying of the stomach can be problematic for some people, and may increase the risk of of food entering the lungs during operations, so it is important to let your doctor know if you are taking any of these drugs.
Because these are injectables, they can also lead to injection-site reactions.
Gastrointestinal side effects are most common. Halfpoint/Shutterstock During clinical trials, there were some reports of thyroid disease and pancreatitis (inflammation of the pancreas). However, it is not clear that these can be attributed to GLP-1 mimicking drugs.
In animals, GLP-1 mimicking drugs drugs have been found to negatively alter the growth of the embryo. There is currently no controlled clinical trial data on their use during pregnancy, but based on animal data, these medicines should not be used during pregnancy.
Who can use them?
The GLP-1 mimicking drugs for weight loss (Wegovy, Saxenda, Zepbound/Mounjaro) are approved for use by people with obesity and are meant to only be used in conjunction with diet and exercise.
These drugs must be prescribed by a doctor and for obesity are not covered by the Pharmaceutical Benefits Scheme, which is one of the reasons why they are expensive. But in time, generic versions of liraglutide are likely to be more affordable.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Tartar Removal At Home & How To Prevent Tartar
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Three things to bear in mind:
- Tartar is hardened plaque.
- Plaque is an infected biofilm that expands the natural thin film on teeth.
- Healthy biofilm resists plaque and tartar formation.
Therefore, the recommended approach is a multistep program:
The Complete Mouth Care System
Dr. Phillips recommends to use these five products in this order twice daily:
- Zellie’s Mints & Gum: having 6–10 grams of xylitol daily will help to loosen plaque on teeth so that the following program is more effective. Xylitol protects from mouth acidity and help to remineralize teeth.
- CloSYS Prerinse: CloSYS will prepare your teeth for brushing. This pH neutral rinse ensures that brushing teeth does not occur in an acidic mouth and therefore easily damage teeth.
- Crest Cavity Protection Regular Paste: has an active ingredient of sodium fluoride at optimal concentration (not stannous fluoride). This paste has the proper abrasion and no glycerine.
- Listerine: is an effective rinse that targets the bacteria that cause plaque build up and gingivitis with three active ingredients: eucalyptus essential oil, menthol essential oil, and thymol essential oil. As such, unlike many mouthwashes, listerine does not harm the mouth’s diversity of good bacteria or the mouth’s production of nitric oxide.
- ACT Anticavity Rinse: ACT is a very dilute but extremely effective sodium fluoride solution. It helps prevent and reverse cavities, strengthen teeth, reduce sensitivity, and leaves your breath fresh.
She advises us that by doing this twice-daily over 6 months, we can expect significant tartar reduction, and indeed, that dental appointments may reveal minimal or no need for tartar removal.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read our own three-part series:
- Toothpastes & Mouthwashes: Which Help And Which Harm?
- Flossing Without Flossing?
- Less Common Oral Hygiene Options ← we recommend the miswak! Not only does it clean the teeth as well as or better than traditional brushing, but also it changes the composition of saliva to improve the oral microbiome, effectively turning your saliva into a biological mouthwash that kills unwanted microbes and is comfortable for the ones that should be there.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: