Do Try This At Home: The 12-Week Brain Fitness Program
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
12 Weeks To Measurably Boost Your Brain
This is Dr. Majid Fotuhi. From humble beginnings (being smuggled out of Iran in 1980 to avoid death in the war), he went on (after teaching himself English, French, and German, hedging his bets as he didn’t know for sure where life would lead him) to get his MD from Harvard Medical School and his PhD in neuroscience from Johns Hopkins University. Since then, he’s had a decades-long illustrious career in neurology and neurophysiology.
What does he want us to know?
The Brain Fitness Program
This is not, by the way, something he’s selling. Rather, it was a landmark 12-week study in which 127 people aged 60–80, of which 63% female, all with a diagnosis of mild cognitive impairment, underwent an interventional trial—in other words, a 12-week brain fitness course.
After it, 84% of the participants showed statistically significant improvements in cognitive function.
Not only that, but of those who underwent MRI testing before and after (not possible for everyone due to practical limitations), 71% showed either no further deterioration of the hippocampus, or actual growth above the baseline volume of the hippocampus (that’s good, and it means functionally the memory center of the brain has been rejuvenated).
You can read a little more about the study here:
As for what the program consisted of, and what Dr. Fotuhi thus recommends for everyone…
Cognitive stimulation
This is critical, so we’re going to spend most time on this one—the others we can give just a quick note and a pointer.
In the study this came in several forms and had the benefit of neurofeedback technology, but he says we can replicate most of the effects by simply doing something cognitively stimulating. Whatever challenges your brain is good, but for maximum effect, it should involve the language faculties of the brain, since these are what tend to get hit most by age-related cognitive decline, and are also what tends to have the biggest impact on life when lost.
If you lose your keys, that’s an inconvenience, but if you can’t communicate what is distressing you, or understand what someone is explaining to you, that’s many times worse—and that kind of thing is a common reality for many people with dementia.
To keep the lights brightly lit in that part of the brain: language-learning is good, at whatever level suits you personally. In other words: there’s a difference between entry-level Duolingo Spanish, and critically analysing Rumi’s poetry in the original Persian, so go with whatever is challenging and/but accessible for you—just like you wouldn’t go to the gym for the first time and try to deadlift 500lbs, but you also probably wouldn’t do curls with the same 1lb weights every day for 10 years.
In other words: progressive overloading is key, for the brain as well as for muscles. Start easy, but if you’re breezing through everything, it’s time to step it up.
If for some reason you’re really set against the idea of learning another language, though, check out:
Reading As A Cognitive Exercise ← there are specific tips here for ensuring your reading is (and remains) cognitively beneficial
Mediterranean diet
Shocking nobody, this is once again recommended. You might like to check out the brain-healthy “MIND” tweak to it, here:
Four Ways To Upgrade The Mediterranean Diet ← it’s the fourth one
Omega-3 supplementation
Nothing complicated here. The brain needs a healthy balance of these fatty acids to function properly, and most people have an incorrect balance (too little omega-3 for the omega-6 present):
What Omega-3 Fatty Acids Really Do For Us ← scroll to “against cognitive decline”
Increasing fitness
There’s a good rule of thumb: what’s healthy for your heart, is healthy for your brain. This is because, like every other organ in your body, the brain does not function well without good circulation bringing plenty of oxygen and nutrients, which means good cardiovascular health is necessary. The brain is extra sensitive to this because it’s a demanding organ in terms of how much stuff it needs delivering via blood, and also because of the (necessary; we’d die quickly and horribly without it) impediment of the blood-brain barrier, and the possibility of beta-amyloid plaques and similar woes (they will build up if circulation isn’t good).
How To Reduce Your Alzheimer’s Risk ← number two on the list here
Practising mindfulness medication
This is also straightforward, but not to be underestimated or skipped over:
No-Frills, Evidence-Based Mindfulness
Want to step it up? Check out:
Meditation Games That You’ll Actually Enjoy
Lastly…
Dr. Fotuhi wants us to consider looking after our brain the same way we look after our teeth. No, he doesn’t want us to brush our brain, but he does want us to take small measurable actions multiple times per day, every day.
You can’t just spend the day doing nothing but brushing your teeth for the entirety of January the 1st and then expect them to be healthy for the rest of the year; it doesn’t work like that—and it doesn’t work like that for the brain, either.
So, make the habits, and keep them going
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fitness Walking and Bodyweight Exercises – by Frank S. Ring

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A lot of exercise manuals assume that the reader has a “basic” body (nothing Olympian, but nothing damaged either). As we get older, increasingly few of us fall into the “but nothing damaged either” category!
Here’s where Ring brings to bear his decades of experience as a coach and educator, and also his personal recovery from a serious back injury.
The book covers direct, actionable exercise advice (with all manner of detail), and also offers mental health tips he’s learned along the way.
Ring, like us, is a big fan of keeping things simple, so he focusses on “the core four” of bodyweight exercises:
- Pushups
- Squats
- Lunges
- Planks
These four exercises get a whole chapter devoted to them, though! Because there are ways to make each exercise easier or harder, or have different benefits. For example, adjustments include:
- Body angle
- Points of contact
- Speed
- Pausing
- Range of motion
This, in effect, makes a few square meters of floor (and perhaps a chair or bench) your fully-equipped gym.
As for walking? Ring enjoys and extols the health benefits, and/but also uses his walks a lot for assorted mental exercises, and recommends we try them too.
A fine book for anyone who wants to gain and/or maintain good health, but doesn’t pressingly want to join a gym or start pumping iron!
Share This Post
-

Is Chiropractic All It’s Cracked Up To Be?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Is Chiropractic All It’s Cracked Up To Be?

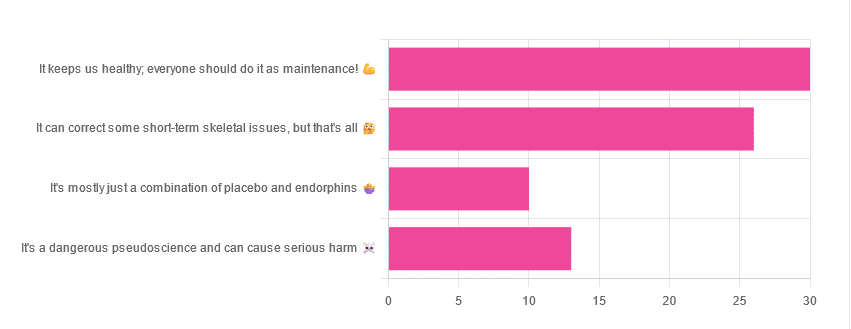
Yesterday, we asked you for your opinions on chiropractic medicine, and got the above-depicted, below-described set of results:
- 38% of respondents said it keeps us healthy, and everyone should do it as maintenance
- 33% of respondents said it can correct some short-term skeletal issues, but that’s all
- 16% of respondents said that it’s a dangerous pseudoscience and can cause serious harm
- 13% of respondents said that it’s mostly just a combination of placebo and endorphins
Respondents also shared personal horror stories of harm done, personal success stories of things cured, and personal “it didn’t seem to do anything for me” stories.
What does the science say?
It’s a dangerous pseudoscience and can cause harm: True or False?
Mixed and True, respectively.
That is to say, chiropractic in its simplest form that makes the fewest claims, is not a pseudoscience. If somebody physically moves your bones around, your bones will be physically moved. If your bones were indeed misaligned, and the chiropractor is knowledgeable and competent, this will be for the better.
However, like any form of medicine, it can also cause harm; in chiropractic’s case, because it more often than not involves manipulation of the spine, this can be very serious:
❝Twenty six fatalities were published in the medical literature and many more might have remained unpublished.
The reported pathology was usually vascular accidents involving the dissection of a vertebral artery.
Conclusion: Numerous deaths have occurred after chiropractic manipulations. The risks of this treatment by far outweigh its benefit.❞
Source: Deaths after chiropractic: a review of published cases
From this, we might note two things:
- The abstract doesn’t note the initial sample size; we would rather have seen this information expressed as a percentage. Unfortunately, the full paper is not accessible, and nor are many of the papers it cites.
- Having a vertebral artery fatally dissected is nevertheless not an inviting prospect, and is certainly a very reasonable cause for concern.
It’s mostly just a combination of placebo and endorphins: True or False?
True or False, depending on what you went in for:
- If you went in for a regular maintenance clunk-and-click, then yes, you will get your clunk-and-click and feel better for it because you had a ritualized* experience and endorphins were released.
- If you went in for something that was actually wrong with your skeletal alignment, to get it corrected, and this correction was within your chiropractor’s competence, then yes, you will feel better because a genuine fault was corrected.
*this is not implying any mysticism, necessarily, though that can certainly also be a component for many, and indeed, chiropractic was originally founded as a new religious movement. Outside of the context of spirituality, however, it means simply that placebo effect is strongest when there is a ritual associated with it. In this case it means going to the place, sitting in a pleasant waiting room, being called in, removing your shoes and perhaps some other clothes, getting the full attention of a confident and assured person for a while, this sort of thing.
With regard to its use to combat specifically spinal pain (i.e., perhaps the most obvious thing to treat by chiropractic spinal manipulation), evidence is slightly in favor, but remains unclear:
❝Due to the low quality of evidence, the efficacy of chiropractic spinal manipulation compared with a placebo or no treatment remains uncertain. ❞
Source: Clinical Effectiveness and Efficacy of Chiropractic Spinal Manipulation for Spine Pain
It can correct some short-term skeletal issues, but that’s all: True or False?
Probably True.
Why “probably”? The effectiveness of chiropractic treatment for things other than short-term skeletal issues has barely been studied. From this, we may wish to keep an open mind, while also noting that it can hardly claim to be evidence-based—and it’s had hundreds of years to accumulate evidence. In all likelihood, publication bias has meant that studies that were conducted and found inconclusive or negative results were simply not published—but that’s just a hypothesis on our part.
In the case of using chiropractic to treat migraines, a very-related-but-not-skeletal issue, researchers found:
❝Pre-specified feasibility criteria were not met, but deficits were remediable. Preliminary data support a definitive trial of MCC+ for migraine.❞
Translating this: “it didn’t score as well as we hoped, but we can do better. We got some positive results, and would like to do another, bigger, better trial; please fund it”
Source: Multimodal chiropractic care for migraine: A pilot randomized controlled trial
Meanwhile, chiropractors’ claims for very unrelated things have been harshly criticized by the scientific community, for example:
Misinformation, chiropractic, and the COVID-19 pandemic
About that “short-term” aspect, one of our subscribers put it quite succinctly:
❝Often a skeletal correction is required for initial alignment but the surrounding fascia and muscles also need to be treated to mobilize the joint and release deep tissue damage surrounding the area. In combination with other therapies chiropractic support is beneficial.❞
This is, by the way, very consistent with what was said in the very clinically-dense book we reviewed yesterday, which has a chapter on the short-term benefits and limitations of chiropractic.
A truism that holds for many musculoskeletal healthcare matters, holds true here too:
❝In a battle between muscle and bone, muscle will always win❞
In other words…
Chiropractic can definitely help put misaligned bones back where they should be. However, once they’re there, if the cause of their misalignment is not treated, they will just re-misalign themselves shortly after you walking out of your session.
This is great for chiropractors, if it keeps you coming back for endless appointments, but it does little for your body beyond give you a brief respite.
So, by all means go to a chiropractor if you feel so inclined (and you do not fear accidental arterial dissection etc), but please also consider going to a physiotherapist, and potentially other medical professions depending on what seems to be wrong, to see about addressing the underlying cause.
Take care!
Share This Post
-

The Diabetes Code – by Dr. Jason Fung
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cure this serious disease with diet!” is often a bold-claim that overreaches scientific rigor, but in this case, it’s well-established as scientifically valid.
Caveat up-front: the only known circumstance in which this won’t work is if you have comorbidities that prevent you from following the advice.
You may be wondering: is this just the Mediterranean diet again? The answer is that the Mediterreanean diet (or similar) is part of it. But there’s a lot more to this book than that.
Dr. Fung explains to us a lot of the physiology of type 2 diabetes; how insulin resistance occurs, how it becomes a vicious cycle that we get locked into, and how to escape it.
- We learn about the role of fructose, and why fruit is very healthful whereas high-fructose corn syrup and similars are very much not.
- We learn about the role of the liver in glycogen metabolism, and how to un-fatty a fatty liver. Good news: the liver has famously strong self-regenerative abilities, if we give it a break to allow it to do so!
- We learn why portion control doesn’t work, and why intermittent fasting does (here be science).
Dr. Fung’s very readable explanations are free from needless jargon while not dumbing down. The writing style is clear and direct: “this happens this way”, “do this, not that”, etc.
Bottom line: if you have type 2 diabetes and would like to not have that (or if you are pre-diabetic and would like to avoid diabetes) this is a book for you. If you are in great metabolic health and would like to stay that way as you get older, then this is a book for you too.
Click here to check out The Diabetes Code, and get/keep your metabolic health in order!
Share This Post
Related Posts
-

Elderberries vs Strawberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing elderberries to strawberries, we picked the elderberries.
Why?
It’s hard to go wrong with (non-poisonous) berries, but…
In terms of macros, elderberries have more than 3x the fiber, 2x the carbs, and (for what it’s worth, which is not a lot because it’s very little) the same amount of protein. An easy win for elderberries.
In the category of vitamins, elderberries have (a lot) more of vitamins A, B1, B2, B3, B5, and B6, while strawberries have more of vitamins B9 and C. Another win for elderberries.
When it comes to minerals, elderberries have more calcium, copper, iron, manganese, phosphorus, potassium, and selenium, while strawberries have more magnesium and zinc. One more win for elderberries.
Looking at phytochemicals, both are good but elderberries have more polyphenols, plus some additional beneficial properties (see the link below). A fourth win for elderberries!
Adding up the sections makes for a clear overall win for elderberries, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Herbs For Evidence-Based Health & Healing ← elderberry significantly hastens recovery from upper respiratory viral infections 😎
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Banana vs Pear – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing banana to pear, we picked the banana.
Why?
In terms of macros, bananas have slightly carbs and protein, while they are equal on fiber. So, which wins this round depends on how we prioritize those macros; for simplicity, we’ll call this one a tie.
In the category of vitamins, bananas have more of vitamins A, B1, B2, B3, B5, B6, B7, B9, C, and choline, while pear has more of vitamins E and K, so, a clear win for bananas this time.
Looking at minerals, bananas have more iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while pears have more calcium. Another easy win for bananas.
Adding up the sections makes for a clear overall win for bananas, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
The Real Magic Number For Daily Fruit/Veg
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Plant Power Doctor
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A Prescription For GLOVES

This is Dr. Gemma Newman. She’s a GP (General Practitioner, British equivalent to what is called a family doctor in America), and she realized that she was treating a lot of patients while nobody was actually getting better.
So, she set out to help people actually get better… But how?
The biggest thing
The single biggest thing she recommends is a whole foods plant-based diet, as that’s a starting point for a lot of other things.
Click here for an assortment of short videos by her and other health professionals on this topic!
Specifically, she advocates to “love foods that love you back”, and make critical choices when deciding between ingredients.
Click here to see her recipes and tips (this writer is going to try out some of these!)
What’s this about GLOVES?
We recently reviewed her book “Get Well, Stay Well: The Six Healing Health Habits You Need To Know”, and now we’re going to talk about those six things in more words than we had room for previously.
They are six things that she says we should all try to get every day. It’s a lot simpler than a lot of checklists, and very worthwhile:
Gratitude
May seem like a wishy-washy one to start with, but there’s a lot of evidence for this making a big difference to health, largely on account of how it lowers stress and anxiety. See also:
How To Get Your Brain On A More Positive Track (Without Toxic Positivity)
Love
This is about social connections, mostly. We are evolved to be a social species, and while some of us want/need more or less social interaction than others, generally speaking we thrive best in a community, with all the social support that comes with that. See also:
How To Beat Loneliness & Isolation
Outside
This is about fresh air and it’s about moving and it’s about seeing some green plants (and if available, blue sky), marvelling at the wonder of nature and benefiting in many ways. See also:
Vegetables
We spoke earlier about the whole foods plant-based diet for which she advocates, so this is that. While reducing/skipping meat etc is absolutely a thing, the focus here is on diversity of vegetables; it is best to make a game of seeing how many different ones you can include in a week (not just the same three!). See also:
Three Critical Kitchen Prescriptions
Exercise
At least 150 minutes moderate exercise per week, and some kind of resistance work. It can be calisthenics or something; it doesn’t have to be lifting weights if that’s not your thing! See also:
Resistance Is Useful! (Especially As We Get Older)
Sleep
Quality and quantity. Yes, 7–9 hours, yes, regardless of age. Unless you’re a child or a bodybuilder, in which case make it nearer 12. But for most of us, 7–9. See also:
Why You Probably Need More Sleep
Want to know more?
As well as the book we mentioned earlier, you might also like:
The Plant Power Doctor – by Dr. Gemma Newman
While the other book we mentioned is available for pre-order for Americans (it’s already released for the rest of the world), this one is available to all right now, so that’s a bonus too.
If books aren’t your thing (or even if they are), you might like her award-winning podcast:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: