3 Secrets Behind The Healing Power Of Plants
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s well-established that whole food plant-based diets including fruits, vegetables, beans, whole grains, nuts, and seeds can reverse chronic diseases like type 2 diabetes, hypertension, high cholesterol, obesity, and more.
Dr. Laurie Marbas explains how it works:
Three ways plant-based diets heal
There’s a lot to be said for plants, from their fiber to their beneficial phytochemicals. For example:
Reversing insulin resistance: plant-based diets help reverse insulin resistance, a major factor in type 2 diabetes, heart disease, obesity, and many other maladies. Particularly high-fiber foods like beans and oats stabilize blood sugar by slowing sugar absorption and reducing insulin spikes. These diets are also naturally low in saturated fats, which are linked to insulin resistance, and include phytonutrients from colorful fruits and vegetables that improve insulin sensitivity. Studies demonstrate that plant-based diets lower HbA1C levels (glycated hemoglobin, a measure of how sugary your blood has been on average in the past 2−3 months) and can even reverse type 2 diabetes for most* people.
*Scientists are very reluctant to claim absolutes such as “all”, “every”, etc, since it cannot be proven that it will work for all people (there are over 8 billion of us after all, and any one of us could get in theory get type 2 diabetes and then try reversing it, so it’s hard to speak for all 8 billion-odd of us) but it is well-established that it usually does indeed reverse it, and for what it’s worth, the confidence interval in such studies is always at least 95% sure, usually higher, which multiplied by countless studies can indeed give us quite some confidence.
Reducing chronic inflammation: chronic inflammation, linked to diseases like arthritis, heart disease, and cancer, can also be reduced through a plant-based diet. Foods rich in antioxidants, such as berries, leafy greens, and nuts, neutralize inflammation-causing free radicals. Omega-3-rich plant foods like chia seeds, flax seeds, and walnuts further balance inflammation. Additionally, fiber fosters healthy gut bacteria, which produce vital compounds that reduce systemic inflammation (and do a lot more good things besides, but we’re limiting ourselves to talking about inflammation here). Research shows that plant-based diets can significantly lower inflammation markers within weeks (almost certainly you’ll notice the difference yourself, too).
Synergy of whole foods: perhaps the biggest power of a plant-based diet lies in the synergy of its components. Nutrients like the fiber and phytonutrients we mentioned work together to combat inflammation and remove waste products that could fuel disease. For example, magnesium, found abundantly in leafy greens (which is why most Americans are deficient in magnesium), supports over 300 enzymatic processes, including blood sugar and inflammation regulation. This holistic approach ensures the whole body receives all the tools it needs to repair, regenerate, and thrive, thus once you’re on the right track, it’s “the gift that keeps on giving” when it comes to health, as each part helps the other parts to work better, which help the other parts to work better, which… (etc)
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
What’s Your Plant Diversity Score?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Yes, you can be intolerant to fruit and veg

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For most people, eating a wide variety of fruit and vegetables is the cornerstone of a healthy diet.
But for people with hereditary fructose intolerance, even a couple of bites of juicy watermelon or some sun-dried tomatoes in a salad can cause serious health problems.
This rare condition isn’t a food allergy or sensitivity.
But it can lead to serious health problems if not identified and correctly managed.

Any Lane/Pexels What is hereditary fructose intolerance?
Hereditary fructose intolerance is a rare genetic condition that affects how the body manages the sugar fructose.
Fructose isn’t just in fruit. It’s in honey, some vegetables, sweetened drinks, and many packaged foods, such as cakes, cookies, sauces and some breads. Fructose can also be added during the processing of some meats (deli meats and sausages) and dairy products (chocolate milk).
Sucrose (table sugar) and sorbitol (a sugar substitute often in chewing gum, toothpaste and medications) also contain fructose or are converted into fructose during digestion. This means people with hereditary fructose intolerance are also intolerant to these sugars.
People with the condition don’t have the key enzyme aldolase B needed to break down fructose.
This means fructose builds up in the liver, kidneys and intestines. This excess fructose can cause serious health problems, such as seizures, coma and, in some cases, death from liver and kidney failure.
How common is it?
Hereditary fructose intolerance is passed down to a person when both their parents carry the gene. It is considered a rare condition that affects about one in 10,000 people.
It usually becomes noticeable when babies begin eating solid foods including fruit, vegetables or sweetened baby foods that contain fructose.
In adults, hereditary fructose intolerance can be missed or misdiagnosed as other conditions such as glycogen storage disease, an eating disorder or recurrent hepatitis.
Because of this overlap in symptoms, hereditary fructose intolerance in adults can remain undetected for years.
How is it different to a food allergy or sensitivity?
Hereditary fructose intolerance is markedly different to a food allergy. A food allergy involves the immune system reacting to a food – for example, cow’s milk protein – as if it’s harmful to the body. This can cause symptoms such as hives and welts, swelling of the mouth or trouble breathing.
Hereditary fructose intolerance is also different to a food sensitivity, such as lactose intolerance or non-coeliac gluten sensitivity. This doesn’t involve the immune system but can still cause discomfort such as bloating, altered bowel habits or stomach pain.
Hereditary fructose intolerance is a genetic condition that causes a food intolerance and is not immune-related.
The condition is also different to fructose malabsorption (which, confusingly has previously been referred to as “dietary fructose intolerance” informally). This is a milder digestive condition where the small intestine doesn’t absorb fructose well, and causes symptoms such as stomach pain, bloating and gas.
How do you know if you have it?
In babies and young children, symptoms may include vomiting, unusual sleepiness or irritability, food refusal and failure to gain weight.
Some children instinctively avoid sweet foods, which may mask the condition until later in childhood or adulthood.
In adults, symptoms can include chronic stomach pain, fatigue and unexplained low blood glucose (sugar) levels. Doctors may notice subtle clues such as a swollen liver, abnormal liver tests or signs of fatty liver disease.
Confirming the condition requires genetic testing or a specialised glucose (sugar) tolerance test. But for many, diagnosis only comes after years of confusion, frustration, and dietary trial and error.
How is it managed?
There’s no cure for hereditary fructose intolerance. But it can be managed by strictly avoiding fructose, sucrose and sorbitol. Reading labels becomes essential for daily life, as even sauces, medications and toothpaste can contain these sugars.
People with the condition need to watch the following:
- fruits: avoid all fruits, juices, canned fruit and other fruit products
- cereals/grains: avoid cereals with added sugars, honey, molasses, dried fruit or sweet flavourings. Pasta, rice and other plain grains such as quinoa or buckwheat are generally safe but avoid flavoured or pre-made varieties
- vegetables: most vegetables are fine, except sweeter ones such as peas, corn, beetroot, onions, pumpkin, sweet potatoes, carrots and zucchini
- breads: only those made without added sugars or sweeteners are OK.
- desserts and dairy: avoid sweetened desserts or flavoured yogurts (natural yogurts are usually fine). Be wary of plant-based milks, such as almond milks, which often have added sugars
- protein: non-sweetened or flavoured red meat, chicken, turkey, fish, beans and lentils, eggs, tofu and tempeh are usually safe. But avoid processed meats, such as sausages/deli meats, or marinated meats
- other foods: be cautious with sauces, dressings and condiments as they many contain hidden sugars or sorbitol. Choose homemade versions using safe ingredients.
Awareness matters
If someone avoids certain foods or if they unwell after eating fruit, don’t assume they’re fussy or dieting – they might have hereditary fructose intolerance.
Greater awareness of this rare condition could mean earlier diagnosis and better support for those affected.
For parents, noticing a child’s sudden or strong aversion to sweets, repeated vomiting or slow growth can be an important clue.
And for doctors, considering hereditary fructose intolerance as a possible cause of unexplained digestive problems, low blood glucose or liver changes could make a life-changing difference.
More information about hereditary fructose intolerance is available, including recipes, tips on how to read food labels, and support.
Lauren Ball, Professor of Community Health and Wellbeing, The University of Queensland; Emily Burch, Accredited Practising Dietitian and Lecturer, Southern Cross University, and Mackenzie Derry, Nutritionist, Dietitian & PhD Candidate, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

A New $16,000 Postpartum Depression Drug Is Here. How Will Insurers Handle It?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A much-awaited treatment for postpartum depression, zuranolone, hit the market in December, promising an accessible and fast-acting medication for a debilitating illness. But most private health insurers have yet to publish criteria for when they will cover it, according to a new analysis of insurance policies.
The lack of guidance could limit use of the drug, which is both novel — it targets hormone function to relieve symptoms instead of the brain’s serotonin system, as typical antidepressants do — and expensive, at $15,900 for the 14-day pill regimen.
Lawyers, advocates, and regulators are watching closely to see how insurance companies will shape policies for zuranolone because of how some handled its predecessor, an intravenous form of the same drug called brexanolone, which came on the market in 2019. Many insurers required patients to try other, cheaper medications first — known as the fail-first approach — before they could be approved for brexanolone, which was shown in early trials reviewed by the FDA to provide relief within days. Typical antidepressants take four to six weeks to take effect.
“We’ll have to see if insurers cover this drug and what fail-first requirements they put in” for zuranolone, said Meiram Bendat, a licensed psychotherapist and an attorney who represents patients.
Most health plans have yet to issue any guidelines for zuranolone, and maternal health advocates worry that the few that have are taking a restrictive approach. Some policies require that patients first try and fail a standard antidepressant before the insurer will pay for zuranolone.
In other cases, guidelines require psychiatrists to prescribe it, rather than obstetricians, potentially delaying treatment since OB-GYN practitioners are usually the first medical providers to see signs of postpartum depression.
Advocates are most worried about the lack of coverage guidance.
“If you don’t have a published policy, there is going to be more variation in decision-making that isn’t fair and is less efficient. Transparency is really important,” said Joy Burkhard, executive director of the nonprofit Policy Center for Maternal Mental Health, which commissioned the study.
With brexanolone, which was priced at $34,000 for the three-day infusion, California’s largest insurer, Kaiser Permanente, had such rigorous criteria for prescribing it that experts said the policy amounted to a blanket denial for all patients, according to an NPR investigation in 2021.
KP’s written guidelines required patients to try and fail four medications and electroconvulsive therapy before they would be eligible for brexanolone. Because the drug was approved only for up to six months postpartum, and trials of typical antidepressants take four to six weeks each, the clock would run out before a patient had time to try brexanolone.
An analysis by NPR of a dozen other health plans at the time showed Kaiser Permanente’s policy on brexanolone to be an outlier. Some did require that patients fail one or two other drugs first, but KP was the only one that recommended four.
Miriam McDonald, who developed severe postpartum depression and suicidal ideation after giving birth in late 2019, battled Kaiser Permanente for more than a year to find effective treatment. Her doctors put her on a merry-go-round of medications that didn’t work and often carried unbearable side effects, she said. Her doctors refused to prescribe brexanolone, the only FDA-approved medication specifically for postpartum depression at the time.
“No woman should suffer like I did after having a child,” McDonald said. “The policy was completely unfair. I was in purgatory.”
One month after NPR published its investigation, KP overhauled its criteria to recommend that women try just one medication before becoming eligible for brexanolone.
Then, in March 2023, after the federal Department of Labor launched an investigation into the insurer — citing NPR’s reporting — the insurer revised its brexanolone guidelines again, removing all fail-first recommendations, according to internal documents recently obtained by NPR. Patients need only decline a trial of another medication.
“Since brexanolone was first approved for use, more experience and research have added to information about its efficacy and safety,” the insurer said in a statement. “Kaiser Permanente is committed to ensuring brexanolone is available when physicians and patients determine it is an appropriate treatment.”
“Kaiser basically went from having the most restrictive policy to the most robust,” said Burkhard of the Policy Center for Maternal Mental Health. “It’s now a gold standard for the rest of the industry.”
McDonald is hopeful that her willingness to speak out and the subsequent regulatory actions and policy changes for brexanolone will lead Kaiser Permanente and other health plans to set patient-friendly policies for zuranolone.
“This will prevent other women from having to go through a year of depression to find something that works,” she said.
Clinicians were excited when the FDA approved zuranolone last August, believing the pill form, taken once a day at home over two weeks, will be more accessible to women compared with the three-day hospital stay for the IV infusion. Many perinatal psychiatrists told NPR it is imperative to treat postpartum depression as quickly as possible to avoid negative effects, including cognitive and social problems in the baby, anxiety or depression in the father or partner, or the death of the mother to suicide, which accounts for up to 20% of maternal deaths.
So far, only one of the country’s six largest private insurers, Centene, has set a policy for zuranolone. It is unclear what criteria KP will set for the new pill. California’s Medicaid program, known as Medi-Cal, has not yet established coverage criteria.
Insurers’ policies for zuranolone will be written at a time when the regulatory environment around mental health treatment is shifting. The U.S. Department of Labor is cracking down on violations of the Mental Health Parity and Addiction Equity Act of 2008, which requires insurers to cover psychiatric treatments the same as physical treatments.
Insurers must now comply with stricter reporting and auditing requirements intended to increase patient access to mental health care, which advocates hope will compel health plans to be more careful about the policies they write in the first place.
In California, insurers must also comply with an even broader state mental health parity law from 2021, which requires them to use clinically based, expert-recognized criteria and guidelines in making medical decisions. The law was designed to limit arbitrary or cost-driven denials for mental health treatments and has been hailed as a model for the rest of the country. Much-anticipated regulations for the law are expected to be released this spring and could offer further guidance for insurers in California setting policies for zuranolone.
In the meantime, Burkhard said, patients suffering from postpartum depression should not hold back from asking their doctors about zuranolone. Insurers can still grant access to the drug on a case-by-case basis before they formalize their coverage criteria.
“Providers shouldn’t be deterred from prescribing zuranolone,” Burkhard said.
This article is from a partnership that includes KQED, NPR and KFF Health News.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-
Healthy Skin At 50… With Sensitive Eyes & No Retinol
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Ruth Machin advises:
Gently does it
As she herself has a tendency to dry skin and easily irritated eyes, she recommends:
- Use a mild, moisturizing cleanser (like Emma Hardy’s Moringa Balm) morning and night; avoid scrubbing and consider water-only washing in the morning if your skin tends towards dryness.
- Skip harsh chemicals if you have sensitive or dry eyes; use gentle physical tools (she recommends Fio Luna 4) to aid skin turnover without irritation of the kind that often occurs with retinol.
- Enjoy formulas with ceramides, squalane, or hyaluronic acid; apply daily, especially after cleansing, and use separate gentle products for the eye area.
- Apply a high-SPF sunscreen that doesn’t irritate your eyes (she recommends Arven SPF 50), even on cloudy days.
- Prioritize sleep, hydration, and a nutrient-dense diet; on the flipside, do of course avoid alcohol and smoking.
For more on all of this as well as some more brand-specific recommendations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Evidence-Based Skincare That Beats Product-Specific Hype
Take care!
Share This Post




Related Posts
-
How Safe Is Botox, Really?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Botox is the brand name of a drug made from botulinum toxin type A, which is made by the bacteria Clostridium botulinum.
This is the same toxin responsible for botulism, so the fact it even has a brand name might be considered a fun sign of where we are as a species.
However! It’s certainly popular, so let’s examine the science.
Cosmetic or therapeutic?
Being as it is a paralytic agent, it’s injected into muscles, usually of the face, usually to temporarily reduce the appearance of wrinkles.
- Sometimes this is because people don’t like to have wrinkles
- Sometimes this is because people have strabismus (misaligned eyes) or blepharospasm (twitching eyes) and the same paralysing agent can fix that
The former category is the most common, by far, but the latter category is overrepresented when it comes to reported adverse effects, i.e., people who have it to treat those conditions, are more likely to report problems. There are two main ways we can interpret that, if we want to hypothesize about causality:
- people who have Botox for therapeutic rather than cosmetic reasons are more likely to experience adverse effects, perhaps because of the underlying condition being treated (actual causality)
- people who have Botox for cosmetic rather than therapeutic reasons were happier to be having it in the first place, and thus less likely to report adverse effects if experienced (reporting bias)
You can read about the stats behind this, here:
We may note that in some cases, cosmetic procedures could be considered therapeutic, if it improves someone’s mental health, but even then there is a distinction.
For cosmetic surgery, for example, satisfaction rates vary thus:
- In “type change” (e.g. rhinoplasty), more psychological adjustment is needed, but when it’s all over, the person has a new nose and, statistically speaking, is usually happy with it.
- In “restorative” (e.g. facelift), less psychological adjustment is needed (as it’s just a return to a previous state), so a person will usually be happy quickly, but ultimately it is merely “kicking the can down the road” if the underlying problem is “fear of aging”, for example. In such a case, likely talking therapy would be beneficial—whether in place of, or alongside, cosmetic surgery.
For more details, see: The Many Faces Of Cosmetic Surgery
For Botox, this is of course “restorative”, and thus (per the science, which we link above) is less likely to result in any lasting improvement in mental health.
And what are the risks?
The recorded possible side effects are quite a laundry list:
- difficulty swallowing
- drooping eyelid
- neck weakness
- nausea
- vomiting
- blurred vision
- general or marked weakness
- difficulty chewing
- hoarseness
- edema
- difficulty speaking
- heart palpitations
But, anyone who has ever read the information leaflet that comes with pretty much any medication will note that in order to cover bases, anything that got reported, even if there was no evidence of association, gets listed.
With this in mind, a large review of evidence (with a total n=42,405) found:
❝…in all enrolled facial rejuvenation studies, patients in the BTX-A group had significantly more AEs than those patients in the placebo group (RR = 1.24; 95 % CI 1.07-1.43; p = 0.003).
For crow’s feet lines injection analysis, the BTX-A group did not exhibit any significant increase in AEs compared with the control group (RR = 1.19; 95 % CI 0.96-1.48; p = 0.12), except in injection site hematoma (RR = 2.14; 95 % CI 1.13-4.07; p = 0.02) in the treatment group.
For frown wrinkle injection analysis, AEs were significantly observed in the BTX-A group (RR = 1.47; 95 % CI 1.23-1.77; p < 0.0001), particularly headaches (RR = 1.53; 95 % CI 1.15-2.03; p = 0.003), eyelid ptosis (RR = 5.56; 95 % CI 1.68-18.38; p = 0.005), and heavy eyelids (RR = 6.94; 95 % CI 1.27-37.93; p = 0.03).❞
AE = adverse event
Translating those stats from sciencese, we can summarize in broad terms* as follows:
- In total, the chance of adverse effects was 24% higher than placebo
- For crow’s feet wrinkle treatments, there was no significant increase, except in the case of injection site hematoma (2x increased risk compared to placebo), which is a little unsightly but is temporary and harmless
- For frown line wrinkle treatments, there as a 53% increased chance of headaches, and a 6x increased chance of heavy/drooping eyelids (which is really not too surprising if you inject a paralysing agent into the muscles next to the muscles that hold them up)
*we also rounded and averaged some figures for readability
In general, these risks have been considered acceptable by the medical establishment as a whole, for example:
❝Treatment with Botox is simple, safe and an effective modality for reduction of forehead wrinkles. It offers an alternative management in a cost-effective way when compared to surgical procedures.❞
Read in full: An Evaluation of Use of Botulinum Toxin Type A in the Management of Dynamic Forehead Wrinkles – A Clinical Study
Your own opinion of the acceptability of these risks may vary, of course.
But watch out!
Botox, administered skillfully by a professional, has a very different risk profile to fake Botox and/or administered incorrectly:
CDC | Harmful Reactions Linked to Counterfeit “Botox” or Mishandled Botulinum Toxin Injections
So, take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Dried Apricots vs Dried Prunes – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing dried apricots to prunes, we picked the apricots.
Why?
First, let’s talk hydration. We’ve described both of these as “dried”, but prunes are by default dried plums, usually partially rehydrated. So, for fairness, on the other side of things we’re also looking at dried apricots, partially rehydrated. Otherwise, it would look (mass for mass or volume for volume) like one is seriously outstripping the other even if some metric were actually equal, just because of water-weight in one and not the other.
Illustrative example: consider, for example, that the sugar in a big bunch of grapes or a small handful of raisins can be the same, not because they magically got more sugar by some mysterious force of transmutation, but because the water was dried out, so per mass and per volume, there’s more sugar, proportionally.
Back to dried apricots and dried prunes…
You’ll often see these two next to each other in the heath food store, which is why we’re comparing them here.
Of course, if it is practical, please by all means enjoy fresh apricots and fresh plums. But we know that life is not always convenient, fruits are not in season growing in abundance in our gardens all year round, and sometimes we’re stood in the aisle of a grocery store, weighing up the dried fruit options.
So, let’s get to it…
In terms of macros, the dried apricots have a touch more fiber while the prunes have a tiny bit more carbs, but it’s so close that most reasonably this round should be considered a tie.
In the category of vitamins, dried apricots have more of vitamins A, B3, B5, B7, B9, C, and E, while prunes have more of vitamins B1, B2, B6, and K; a clear win for apricots by strength of numbers, though it’s worth noting that the vitamin K difference is considerable (19x more vitamin K).
Looking at minerals, dried apricots have more calcium, copper, iron, potassium, and selenium, while prunes have more magnesium, manganese and zinc, yielding a 5:3 win to apricots here.
Adding up the sections makes for a clear overall win for apricots, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like:
Which Sugars Are Healthier, And Which Are Just The Same?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cannabis Myths vs Reality
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cannabis Myths vs Reality

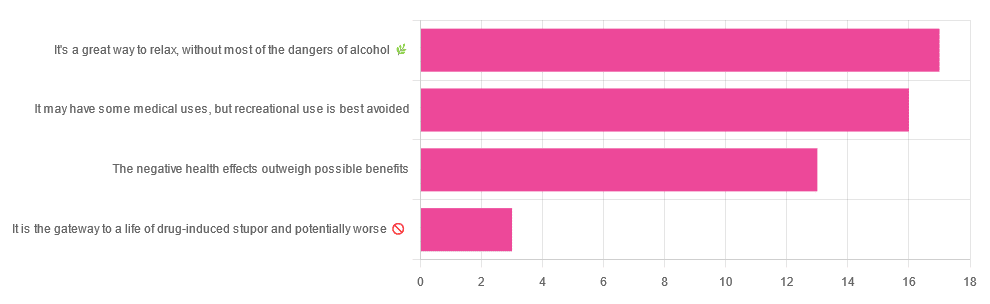
We asked you for your (health-related) opinion on cannabis use—specifically, the kind with psychoactive THC, not just CBD. We got the above-pictured, below-described, spread of responses:
- A little over a third of you voted for “It’s a great way to relax, without most of the dangers of alcohol”.
- A little under a third of you voted for “It may have some medical uses, but recreational use is best avoided”.
- About a quarter of you voted for “The negative health effects outweigh the possible benefits”
- Three of you voted for “It is the gateway to a life of drug-induced stupor and potentially worse”
So, what does the science say?
A quick legal note first: we’re a health science publication, and are writing from that perspective. We do not know your location, much less your local laws and regulations, and so cannot comment on such. Please check your own local laws and regulations in that regard.
Cannabis use can cause serious health problems: True or False?
True. Whether the risks outweigh the benefits is a personal and subjective matter (for example, a person using it to mitigate the pain of late stage cancer is probably unconcerned with many other potential risks), but what’s objectively true is that it can cause serious health problems.
One subscriber who voted for “The negative health effects outweigh the possible benefits” wrote:
❝At a bare minimum, you are ingesting SMOKE into your lungs!! Everyone SEEMS TO BE against smoking cigarettes, but cannabis smoking is OK?? Lung cancer comes in many forms.❞
Of course, that is assuming smoking cannabis, and not consuming it as an edible. But, what does the science say on smoking it, and lung cancer?
There’s a lot less research about this when it comes to cannabis, compared to tobacco. But, there is some:
❝Results from our pooled analyses provide little evidence for an increased risk of lung cancer among habitual or long-term cannabis smokers, although the possibility of potential adverse effect for heavy consumption cannot be excluded.❞
Read: Cannabis smoking and lung cancer risk: Pooled analysis in the International Lung Cancer Consortium
Another study agreed there appears to be no association with lung cancer, but that there are other lung diseases to consider, such as bronchitis and COPD:
❝Smoking cannabis is associated with symptoms of chronic bronchitis, and there may be a modest association with the development of chronic obstructive pulmonary disease. Current evidence does not suggest an association with lung cancer.❞
Read: Cannabis Use, Lung Cancer, and Related Issues
Cannabis edibles are much safer than smoking cannabis: True or False?
Broadly True, with an important caveat.
One subscriber who selected “It may have some medical uses, but recreational use is best avoided”, wrote:
❝I’ve been taking cannabis gummies for fibromyalgia. I don’t know if they’re helping but they’re not doing any harm. You cannot overdose you don’t become addicted.❞
Firstly, of course consuming edibles (rather than inhaling cannabis) eliminates the smoke-related risk factors we discussed above. However, other risks remain, including the much greater ease of accidentally overdosing.
❝Visits attributable to inhaled cannabis are more frequent than those attributable to edible cannabis, although the latter is associated with more acute psychiatric visits and more ED visits than expected.❞
Note: that “more frequent” for inhaled cannabis, is because more people inhale it than eat it. If we adjust the numbers to control for how much less often people eat it, suddenly we see that the numbers of hospital admissions are disproportionately high for edibles, compared to inhaled cannabis.
Or, as the study author put it:
❝There are more adverse drug events associated on a milligram per milligram basis of THC when it comes in form of edibles versus an inhaled cannabis. If 1,000 people smoked pot and 1,000 people at the same dose in an edible, then more people would have more adverse drug events from edible cannabis.❞
See the numbers: Acute Illness Associated With Cannabis Use, by Route of Exposure
Why does this happen?
- It’s often because edibles take longer to take effect, so someone thinks “this isn’t very strong” and has more.
- It’s also sometimes because someone errantly eats someone else’s edibles, not realising what they are.
- It’s sometimes a combination of the above problems: a person who is now high, may simply forget and/or make a bad decision when it comes to eating more.
On the other hand, that doesn’t mean inhaling it is necessarily safer. As well as the pulmonary issues we discussed previously, inhaling cannabis has a higher risk of cannabinoid hyperemesis syndrome (and the resultant cyclic vomiting that’s difficult to treat).
You can read about this fascinating condition that’s sometimes informally called “scromiting”, a portmanteau of screaming and vomiting:
Cannabinoid Hyperemesis Syndrome
You can’t get addicted to cannabis: True or False?
False. However, it is fair to say that the likelihood of developing a substance abuse disorder is lower than for alcohol, and much lower than for nicotine.
See: Prevalence of Marijuana Use Disorders in the United States Between 2001–2002 and 2012–2013
If you prefer just the stats without the science, here’s the CDC’s rendering of that:
Addiction (Marijuana or Cannabis Use Disorder)
However, there is an interesting complicating factor, which is age. One is 4–7 times more likely to develop a substance abuse disorder, if one starts use as an adolescent, rather than later as an adult:
Cannabis is the gateway to use of more dangerous drugs: True or False?
False, generally speaking. Of course, for any population there will be some outliers, but there appears to be no meaningful causal relation between cannabis use and other substance use:
Interestingly, the strongest association (where any existed at all) was between cannabis use and opioid use. However, rather than this being a matter of cannabis use being a gateway to opioid use, it seems more likely that this is a matter of people looking to both for the same purpose: pain relief.
As a result, growing accessibility of cannabis may actually reduce opioid problems:
- Cannabis as a Gateway Drug for Opioid Use Disorder
- Association between medical cannabis laws and opioid overdose mortality has reversed over time
Some final words…
Cannabis is a complex drug with complex mechanisms and complex health considerations, and research is mostly quite young, due to its historic illegality seriously cramping science by reducing sample sizes to negligible. Simply put, there’s a lot we still don’t know.
Also, we covered some important topics today, but there were others we didn’t have time to cover, such as the other potential psychological benefits—and risks. Likely we’ll revisit those another day.
Lastly, while we’ve covered a bunch of risks today, those of you who said it has fewer and lesser risks than alcohol are quite right—the only reason we couldn’t focus on that more, is because to talk about all the risks of alcohol would make this feature many times longer!
Meanwhile, whether you partake or not, stay safe and stay well.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: