Antidepressants: Personalization Is Key!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Antidepressants: Personalization Is Key!
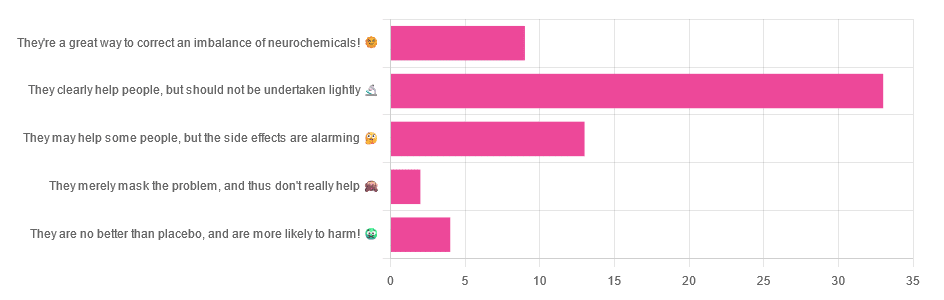
Yesterday, we asked you for your opinions on antidepressants, and got the above-depicted, below-described, set of responses:
- Just over half of respondents said “They clearly help people, but should not be undertaken lightly”
- Just over a fifth of respondents said “They may help some people, but the side effects are alarming”
- Just under a sixth of respondents said “They’re a great way to correct an imbalance of neurochemicals”
- Four respondents said “They are no better than placebo, and are more likely to harm”
- Two respondents said “They merely mask the problem, and thus don’t really help”
So what does the science say?
❝They are no better than placebo, and are more likely to harm? True or False?❞
True or False depending on who you are and what you’re taking. Different antidepressants can work on many different systems with different mechanisms of action. This means if and only if you’re not taking the “right” antidepressant for you, then yes, you will get only placebo benefits:
- Placebo Effect in the Treatment of Depression and Anxiety ← randomly assigned antidepressants are, shockingly, luck of the draw in usefulness
- Antidepressants versus placebo in major depression: an overview ← “wow this science is messy”
- Comparative efficacy and acceptability of 21 antidepressant drugs: a systematic review and network meta-analysis ← “oh look, it makes a difference which antidepressant we give to people”
Rather than dismissing antidepressants as worthless, therefore, it is a good idea to find out (by examination or trial and error) what kind of antidepressant you need, if you indeed do need such.
Otherwise it is like getting a flu shot and being surprised when you still catch a cold!
❝They merely mask the problem, and thus don’t really help: True or False?❞
False, categorically.
The problem in depressed people is the depressed mood. This may be influenced by other factors, and antidepressants indeed won’t help directly with those, but they can enable the person to better tackle them (more on this later).
❝They may help some people, but the side-effects are alarming: True or False?❞
True or False depending on more factors than we can cover here.
Side-effects vary from drug to drug and person to person, of course. As does tolerability and acceptability, since to some extent these things are subjective.
One person’s dealbreaker may be another person’s shrugworthy minor inconvenience at most.
❝They’re a great way to correct an imbalance of neurochemicals: True or False?❞
True! Contingently.
That is to say: they’re a great way to correct an imbalance of neurochemicals if and only if your problem is (at least partly) an imbalance of neurochemicals. If it’s not, then your brain can have all the neurotransmitters it needs, and you will still be depressed, because (for example) the other factors* influencing your depression have not changed.
*common examples include low self-esteem, poor physical health, socioeconomic adversity, and ostensibly bleak prospects for the future.
For those for whom the problem is/was partly a neurochemical imbalance and partly other factors, the greatest help the antidepressants give is getting the brain into sufficient working order to be able to tackle those other factors.
Want to know more about the different kinds?
Here’s a helpful side-by-side comparison of common antidepressants, what type they are, and other considerations:
Mind | Comparing Antidepressants
Want a drug-free approach?
You might like our previous main feature:
The Mental Health First-Aid That You’ll Hopefully Never Need
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Milk Thistle For The Brain, Bones, & More

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Thistle Do Nicely”
Milk thistle is a popular supplement; it comes from the milk thistle plant (Silybum marianum), commonly just called thistles. There are other kinds of thistle too, but these are one of the most common.
So, what does it do?
Liver health
Milk thistle enjoys popular use to support liver health; the liver is a remarkably self-regenerative organ if given the chance, but sometimes it can use a helping hand.
See for example: How To Undo Liver Damage
As for milk thistle’s beneficence, it is very well established:
- Milk thistle in liver diseases: past, present, future
- Hepatoprotective effect of silymarin
- Silybum Marianum and Chronic Liver Disease: A Marriage of Many Years
Brain health
For this one the science is less well-established, as studies so far have been on non-human animals, or have been in vitro studies.
Nevertheless, the results so far are promising, and the mechanism of action seems to be a combination of reducing oxidative stress and neuroinflammation, as well as suppressing amyloid β-protein (Aβ) fibril formation, in other words, reducing amyloid plaques.
General overview: A Mini Review on the Chemistry and Neuroprotective Effects of Silymarin
All about the plaques, but these are non-human animal studies:
- Mouse model: Silymarin attenuated the amyloid β plaque burden and improved behavioral abnormalities in an Alzheimer’s disease mouse model
- Rat model: Silymarin effect on amyloid-β plaque accumulation and gene expression of APP in an Alzheimer’s disease rat model
Against diabetes
Milk thistle improves insulin sensitivity, and reduces fasting blood sugar levels and HbA1c levels. The research so far is mostly in type 2 diabetes, however (at least, so far as we could find). For example:
Studies we could find for T1D were very far from translatable to human usefulness, for example, “we poisoned these rats with streptozotocin then gave them megadoses of silymarin (10–15 times the dose usually recommended for humans) and found very small benefits to the lenses of their eyes” (source).
Against osteoporosis
In this case, milk thistle’s estrogenic effects may be of merit to those at risk of menopause-induced osteoporosis:
If you’d like a quick primer about such things as what antiosteoclastic activity is, here’s a quick recap:
Which Osteoporosis Medication, If Any, Is Right For You?
Is it safe?
It is “Generally Recognized As Safe”, and even when taken at high doses for long periods, side effects are very rare.
Contraindications include if you’re pregnant, nursing, or allergic.
Potential reasons for caution (but not necessarily contraindication) include if you’re diabetic (its blood-sugar lowering effects will decrease the risk of hyperglycemia while increasing the risk of hypoglycemia), or have a condition that could be exacerbated by its estrogenic effects—including if you are on HRT, because it’s an estrogen receptor agonist in some ways (for example those bone benefits we mentioned before) but an estrogen antagonist in others (for example, in the uterus, if you have one, or in nearby flat muscles, if you don’t).
As ever, speak with your doctor/pharmacist to be sure.
Want to try it?
We don’t sell it, but here for your convenience is an example product on Amazon
Enjoy!
Share This Post
-

Better Sex = Longer Life (Here’s How)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Dr. Candice Hargons. She’s a professor of psychology, and has served on the Kentucky Psychological Association Board, the Society of Counseling Psychology Executive Board, and the American Psychological Association (APA)’s Council of Representatives. She also served on the APA Board of Directors, after receiving the APA’s Presidential Citation award for her research and leadership.
She leads the Study of Mental And Sexual Health Equity in Relationships (SMASHER Lab), with a predominant focus on promoting good sex, sexual wellness, and liberation among couples and communities.
In her own words:
❝Sex is one of the most common and normal human behaviors, and yet it remains relatively taboo as a topic. Many people worry about being judged, either for being perceived as too sexual or not sexual enough, and a major focus of my work is to normalize talking and learning about sex to improve sexual functioning across the adult lifespan.❞
~ Dr. Candice Hargons
So, let’s do that!
What does good sex do for health?
We’ve written previously about the health aspects of orgasms specifically:
“Early To Bed…” (Mythbusting Orgasms) ← including resources pertaining to anorgasmia, the inability to orgasm
…but orgasms are not the be-all-and-end-all of sex; see for example:
A Urologist Explains Edging: What, Why, & Is It Safe? ← when the journey is genuinely more of a focus than the destination
And certainly, good sex is simply a very good way to relax and de-stress, which is important, given how important stress management is to general health in very many ways (affecting things ranging from inflammation to heart health and more).
Plus, while the level of athleticism deployed may vary, sex is a physical activity, and physical activity is, as a rule, good.
There’s more to it than that though! It also can help us bind closely to our loved ones, in a positive way, which—critically—has a very positive impact on healthy longevity:
Only One Kind Of Relationship Promotes Longevity This Much! ← this is about the seriousness of the relationship, not the sex, but for most people, a strong and fulfilling relationship will include having good sex.
The scientific relationship between sex and longevity also got a whole chapter in this excellent book that we reviewed all so recently:
Age Proof: The New Science of Living a Longer and Healthier Life – by Dr. Rose Anne Kenny
What makes it “good”?
Dr. Hargons considers (and her opinion is backed by extensive research in the SMASHER Lab, if you’ll pardon the mental image that that might conjure) that first and foremost… It has to feel good to all parties involved.
In contrast, oftentimes, one partner’s pleasure is prioritized over another’s, and that becomes a problem.*
*assuming that’s not part of an established kink dynamic with enthusiastic affirmative consent, such as if the partner whose pleasure is being deprioritized is enthusiastically requesting to be denied orgasms, for example. Yes, that’s a real kink and even a popular one, but it’s not what’s happening in most sexually uneven relationships.
This kind of unplanned disparity often goes undiscussed by the couple in question—especially in heterosexual couples if the man is getting what he wants/needs and the woman isn’t, because there’s a rather lop-sided societal expectation in that regard. And even a loving, well-intentioned man can simply not know how to do better and be afraid to ask. And for that matter, it’s also entirely possible for his partner to not know either.
Dr. Hargons lists the four main keys as:
- Communication
- Intimacy
- Passion
- Pleasure
And communication indeed comes first, so to speak. For example, she advises:
❝Begin by identifying what you like and don’t like sexually. An easy way to do this is to create a “Yes, No, Maybe So” list. You can use paper or a Notes app on your phone.
Create three columns: one for Yes, No, and Maybe So sections. In the Yes section, write all the things you enjoy and want to keep doing sexually, as well as things you have not tried yet that you want to try. In the No section, write all the things you don’t enjoy and do not want to do anymore. It can also include things you haven’t tried that you’re uninterested in trying. Finally, in your Maybe So list, write all the things you’re curious about and/or are only willing to try in specific settings or circumstances.
You can share this list with your partner, but even if you are not ready to do that, you will already have enhanced your sexual self-awareness and be better positioned to talk with your sexual partner about what you want.❞
This represents an important shift from “whatever” to taking an active role in your sex life at your own pace.
And from there, it’s just a matter of exploring, together, and learning as you go. Could anything be more exciting than that?
“What if I’m single?”
We talked about this a little previously, more relationally than sexually specifically, though:
Now, a single person can of course still have an active sex life if you so choose, in which case, the above advice still applies, just, it’ll be conversations with your partner-of-the-moment rather than with a life partner. And that’s important too! Just because something is casual, doesn’t mean it need not be entered into mindfully and with a sense of what you want out of it, and communicating that effectively (while encouraging the same from others, and of course actually listening to, and caring about, what they say too).
And if you are, perchance, single and decided on a life of celibacy now, you can and (if you are sexual at all) should still figure out what you like and don’t like sexually, because even if it’s going to be you-on-you action, it will be good for you to love yourself enough to do it right.
Seriously, treat yourself at least as well as you would any other lover.
On which note, corded wand-style vibrators like the famous “Magic Wand” kind are much more powerful than the battery kind, and you will feel the difference, in a good way.
And if you really want to invest in your sexual wellness and you like the idea, saddle-style vibrators like this one will rock your socks off in ways handheld vibrators couldn’t dream of.
Want to know more?
You might want to check out Dr. Hargons’ book:
Good Sex: Stories, Science, and Strategies for Sexual Liberation – by Dr. Candice Hargons ← this covers so many important areas, more than we have room to here. Just check out the table of contents, and you’ll see what we mean.
…which we haven’t reviewed yet, but here are some excellent related books that we have:
- Come Together: The Science (and Art) of Creating Lasting Sexual Connections – by Dr. Emily Nagoski
- Better Sex Through Mindfulness: How Women Can Cultivate Desire – by Dr. Lori Brotto
Enjoy!
Share This Post
-
8 Signs On Your Breast You Shouldn’t Ignore
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Can you name the 8 signs that may indicate breast cancer? This video discusses them, and also shows what they look like on various different skintones:
Stay abreast:
Dr Simi Adedeji bids us watch out for:
- Inverted nipple: a newly inverted nipple (pointing inward or folded) should be checked by a doctor, especially if it’s a recent change.
- Flaky rash: a flaky, itchy, or red rash around the nipple or areola could indicate an underlying issue and should not be dismissed as just a skin condition.
- Tethering: skin pulling or denting, noticeable when raising your arms, may signal a deeper problem.
- Dimpling: skin resembling an orange peel (po orang sign) with dips and accentuated pores could indicate swelling or thickening and requires medical evaluation.
- Redness or heat: unusual warmth, redness, or tenderness in the breast, particularly if not breastfeeding, should be investigated.
- Nipple discharge: any unusual fluid from the nipple (be it yellow, green, milky, clear, or blood-stained) warrants attention, especially if spontaneous or only from one side.
- Change in size: sudden changes in the size or shape of one breast should not be ignored.
- Breast lump: a firm, irregular, or persistent lump in the breast, armpit, or collarbone area should be checked promptly, even if it’s not always harmful.
The above signs may indicate cancer or something else, but none of them are things that should be ignored (even if you get just one sign).
For more on each of these, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The Hormone Therapy That Reduces Breast Cancer Risk & More
Take care!
Share This Post


Related Posts
-

Regular Nail Polish vs Gel Nail Polish – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing regular nail polish to gel nail polish, we picked the regular.
Why?
This one’s less about what’s in the bottle, and more about what gets done to your hands:
- Regular nail polish application involves carefully brushing it on.
- Regular nail polish removal involves wiping with acetone.
…whereas:
- Gel nail polish application involves deliberately damaging (roughing up) the nail to allow the color coat to adhere, then when the top coat is applied, holding the nails (and thus, the attached fingers) under a UV light to set it. That UV lamp exposure is very bad for the skin.
- Gel nail polish removal involves soaking in acetone, which is definitely worse than wiping with acetone. Failure to adequately soak it will result in further damage to the nail while trying to get the base coat off the nail that you already deliberately damaged when first applying it.
All in all, regular nail polish isn’t amazing for nail health (healthiest is for nails to be free and naked), but for those of us who like a little bit of color there, regular is a lot better than gel.
Gel nail polish damages the nail itself by necessity, and presents a cumulative skin cancer risk and accelerated aging of the skin, by way of the UV lamp use.
For your interest, here are the specific products that we compared, but the above goes for any of this kind:
Regular nail polish | Gel nail polish
If you’d like to read more about nail health, you might enjoy reading:
The Counterintuitive Dos and Don’ts of Nail Health
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Brown Rice vs Russet Potatoes – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing brown rice to russet potatoes, we picked the rice.
Why?
First we’ll note: for brevity and to avoid undue repetitiveness, we’re henceforth going to just say “rice” and “potato”, respectively, but values and conclusions are still for brown rice and russet potatoes. Also, we are including the flesh and skin into the metrics for the potato (without the skin, many nutrients are no longer present).
In terms of macros, the rice has more fiber, carbs, and protein. It’s difficult to compare glycemic indices in this case, because they both need cooking before eating, and how one cooks them (and whether one cools them) along with other preparatory methods will change the GI considerably. Thus, we’ll simply go with the more nutritionally dense option, and that’s the rice.
In the category of vitamins, the rice has much more of vitamins B1, B2, B3, B5, B6, B7, B9, E, and choline, while the potato has more of vitamins C and K. A clear win for rice (and by the way, that’s 60x the vitamin E, but as potatoes don’t have much vitamin E, in practical terms, it’s actually the B-vitamins where rice’s strengths really show, as potatoes aren’t a bad source but rice is amazing).
When it comes to minerals, rice has a lot more copper, iron, magnesium, manganese, phosphorus, selenium, and zinc, while potato has more calcium and potassium. Another easy win for rice.
You may be wondering about phytic acid: brown rice contains this by default, and it is something of an antinutrient (i.e., if left as-is, it reduces the bioavailability of other nutrients), and/but the phytic acid content is reduced to negligible by two things: soaking and heating (especially if those two things are combined) ← doing this the way described results in bioavailability of nutrients that’s even better than if there were just no phytic acid, albeit it requires you having the time to soak, and do so at temperature.
All in all, adding up the sections makes for an overall win for brown rice, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Carb-Strong or Carb-Wrong? Should You Go Light Or Heavy On Carbs?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Gut-Healthy Tacos
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Full of prebiotics and probiotics, healthy fats, colorful salad boasting vitamins and minerals aplenty, and of course satisfying protein too, these tacos are also boasting generous flavors to keep you coming back for more…
You will need
- 24 sardines—canned is fine (if vegetarian/vegan, substitute tempeh and season generously; marinade if you have time)
- 12 small wholewheat tortillas
- 1 14oz/400g can black beans, drained
- 1 ripe avocado, stoned and cut into small chunks
- 1 red onion, thinly sliced
- 1 little gem lettuce, shredded
- 12 cherry tomatoes, halved
- 1 bulb garlic, crushed
- 1 lemon, sliced
- 4 tbsp plain unsweetened yogurt (your choice what kind, but something with a live culture is best)
- 3oz pickled jalapeños, roughly chopped
- 1oz cilantro (or substitute parsley if you have the cilantro-tastes-like-soap gene), finely chopped
- 1 tbsp extra virgin olive oil
- 2 tsp black pepper
- 1 tsp smoked paprika
- Juice of 1 lime
- Optional: Tabasco sauce, or similar hot sauce
Method
(we suggest you read everything at least once before doing anything)
1) Preheat your oven to a low temperature; 200℉ or just under 100℃ is fine
2) Place the lemon slices on top of the sardines on top of foil on a baking tray; you want the foil to be twice as much as you’d expect to need, because now you’re going to fold it over and make a sort of sealed envelope. You could use a dish with a lid yes, but this way is better because there’s going to be less air inside. Upturn the edges of the envelope slightly so that juices won’t run out, and make sure the foil is imperfectly sealed so a little steam can escape but not much at a time. This will ensure it doesn’t dry out, while also ensuring your house doesn’t smell of fish. Put all this into the oven on a middle shelf.
3) Mix the lime juice with the onion in a bowl, and add the avocado and tomatoes, mixing gently. Add half the cilantro, and set aside.
4) Put the black beans in a sieve and pour boiling water over them to refresh and slightly warm them. Tip them into a bowl and add the olive oil, black pepper, and paprika. Mix thoroughly with a fork, and no need to be gentle this time; in fact, deliberately break the beans a little in this case.
5) Mix the yogurt, jalapeños, garlic, and remaining cilantro in a small bowl.
6) Get the warmed sardines from the oven; discard the lemon slices.
7) Assemble! We recommend the order: tortilla, lettuce, fish (2 per taco), black bean mixture, salad mixture, garlic jalapeño yogurt mixture. You can also add a splash of the hot sauce per your preference, or if catering for more people, let people add their own.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- We Are Such Stuff As Fish Are Made Of
- Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
- Making Friends With Your Gut (You Can Thank Us Later)
- Our Top 5 Spices: How Much Is Enough For Benefits?
- Enjoy Pungent Polyphenols For Your Heart & Brain
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: