Celery vs Rhubarb – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing celery to rhubarb, we picked the rhubarb.
Why?
In terms of macros, rhubarb has more carbs and fiber, the ratio of which give it the lower glycemic index, though both are low glycemic index foods. This means we’re calling this category a very marginal win for rhubarb, but a first-round win nevertheless!
In the category of vitamins, celery has more of vitamins A, B5, B6, and B9, while rhubarb has more vitamin C. A win for celery, this time.
Looking at minerals next, celery has more copper and phosphorus, while rhubarb has more calcium, iron, magnesium, manganese, potassium, and selenium. This one’s a clear win for rhubarb.
In other considerations, rhubarb has more polyphenols in not only in terms of overall quantity, but also in terms of “more useful to humans” too, being rich in an assortment of flavanols while celery must make do with some furanocoumarins (not in dangerous quantities, though).
Adding up the sections make for a clear overall win for rhubarb, but by all means do enjoy either or both, as diversity is best!
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Rapamycin Can Slow Aging By 20% (But Watch Out)

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Rapamycin’s Pros & Cons
Rapamycin is generally heralded as a wonderdrug that (according to best evidence so far) can slow down aging, potentially adding decades to human lifespan—and yes, healthspan.
It comes from a kind of soil bacteria, which in turn comes from the island of Rapa Nui (a Chilean territory best known for its monumental moai statues), hence the name rapamycin.
Does it work?
Yes! Probably! With catches!
Like most drugs that are tested for longevity-inducing properties, research in humans is very slow. Of course for drugs in general, they must go through in vitro and in vivo animal testing first before they can progress to human randomized clinical trials, but for longevity-inducing drugs, it’s tricky to even test in humans, without waiting entire human lifetimes for the results.
Nevertheless, mouse studies are promising:
Rapamycin: An InhibiTOR of Aging Emerges From the Soil of Easter Island
(“Easter Island” is another name given to the island of Rapa Nui)
That’s not a keysmash in the middle there, it’s a reference to rapamycin’s inhibitory effect on the kinase mechanistic target of rapamycin, sometimes called the mammalian target of rapamycin, and either way generally abbreviated to “mTOR”—also known as “FK506-binding protein 12-rapamycin-associated protein 1” or “FRAP1“ to its friends, but we’re going to stick with “mTOR”.
What’s relevant about this is that mTOR regulates cell growth, cell proliferation, cell motility, cell survival, protein synthesis, autophagy, and transcription.
Don’t those words usually get associated with cancer?
They do indeed! Rapamycin and its analogs have well-demonstrated anti-cancer potential:
❝Rapamycin, the naturally occurring inhibitor of mTOR, along with a number of recently developed rapamycin analogs (rapalogs) consisting of synthetically derived compounds containing minor chemical modifications to the parent structure, inhibit the growth of cell lines derived from multiple tumor types in vitro, and tumor models in vivo.
Results from clinical trials indicate that the rapalogs may be useful for the treatment of subsets of certain types of cancer.❞
…and as such, gets used sometimes as an anticancer drug—especially against renal cancer. See also:
Research perspective: Cancer prevention with rapamycin
What’s the catch?
Aside from the fact that its longevity-inducing effects are not yet proven in humans, the mouse models find its longevity effects to be sex-specific, extending the life of male mice but not female ones:
Rapamycin‐mediated mouse lifespan extension: Late‐life dosage regimes with sex‐specific effects
One hypothesis about this is that it may have at least partially to do with rapamycin’s immunomodulatory effect, bearing in mind that estrogen is immune-enhancing and testosterone is immunosuppressant.
And rapamycin? That’s another catch: it is an immunosuppressant.
This goes in rapamycin’s favor for its use to avoiding rejection when it comes to some transplants (most notably including for kidneys), though the very same immunosuppressant effect is a reason it is contraindicated for certain other transplants (such as in liver or lung transplants), where it can lead to an unacceptable increase in risk of lymphoma and other malignancies:
Prescribing Information: Rapamune, Sirolimus Solution / Sirolimus Tablet
(Sirolimus is another name for rapamycin, and Rapamune is a brand name)
What does this mean for the future?
Researchers think that rapamycin may be able to extend human lifespan to a more comfortable 120–125 years, but acknowledge there’s quite a jump to get there from the current mouse studies, and given the current drawbacks of sex-specificity and immunosuppression:
Advances in anti-aging: Rapamycin shows potential to extend lifespan and improve health
Noteworthily, rapamycin has also shown promise in simultaneously staving off certain diseases associated most strongly with aging, including Alzheimer’s and cardiac disease—or even, starting earlier, to delay menopause, in turn kicking back everything else that has an uptick in risk peri- or post-menopause:
Effect of Rapamycin in Ovarian Aging (Rapamycin)
👆 an upcoming study whose results are thus not yet published, but this is to give an idea of where research is currently at. See also:
Pilot Study Evaluates Weekly Pill to Slow Ovarian Aging, Delay Menopause
Where can I try it?
Not from Amazon, that’s for sure!
It’s still tightly regulated, but you can speak with your physician, especially if you are at risk of cancer, especially if kidney cancer, about potentially being prescribed it as a preventative—they will be able to advise about safety and applicability in your personal case.
Alternatively, you can try getting your name on the list for upcoming studies, like the one above. ClinicalTrials.gov is a great place to watch out for those.
Meanwhile, take care!
Share This Post
-

Half of Australians in aged care have depression. Psychological therapy could help
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
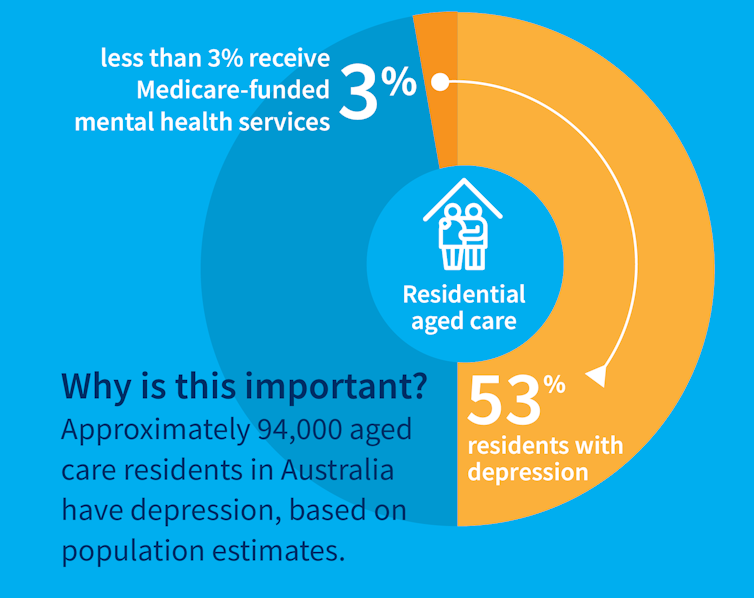
While many people maintain positive emotional wellbeing as they age, around half of older Australians living in residential aged care have significant levels of depression. Symptoms such as low mood, lack of interest or pleasure in life and difficulty sleeping are common.
Rates of depression in aged care appear to be increasing, and without adequate treatment, symptoms can be enduring and significantly impair older adults’ quality of life.
But only a minority of aged care residents with depression receive services specific to the condition. Less than 3% of Australian aged care residents access Medicare-subsidised mental health services, such as consultations with a psychologist or psychiatrist, each year.

Cochrane AustraliaInstead, residents are typically prescribed a medication by their GP to manage their mental health, which they often take for several months or years. A recent study found six in ten Australian aged care residents take antidepressants.
While antidepressant medications may help many people, we lack robust evidence on whether they work for aged care residents with depression. Researchers have described “serious limitations of the current standard of care” in reference to the widespread use of antidepressants to treat frail older people with depression.
Given this, we wanted to find out whether psychological therapies can help manage depression in this group. These treatments address factors contributing to people’s distress and provide them with skills to manage their symptoms and improve their day-to-day lives. But to date researchers, care providers and policy makers haven’t had clear information about their effectiveness for treating depression among older people in residential aged care.
The good news is the evidence we published today suggests psychological therapies may be an effective approach for people living in aged care.
We reviewed the evidence
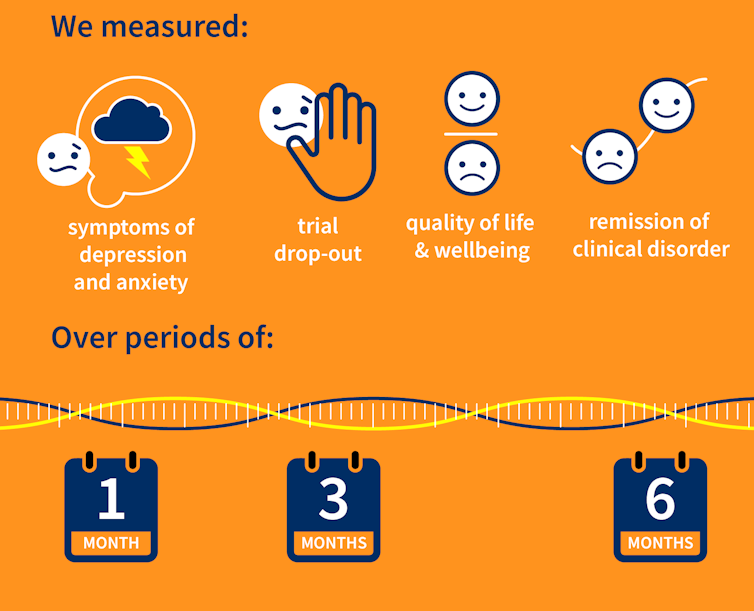
Our research team searched for randomised controlled trials published over the past 40 years that were designed to test the effectiveness of psychological therapies for depression among aged care residents 65 and over. We identified 19 trials from seven countries, including Australia, involving a total of 873 aged care residents with significant symptoms of depression.
The studies tested several different kinds of psychological therapies, which we classified as cognitive behavioural therapy (CBT), behaviour therapy or reminiscence therapy.
CBT involves teaching practical skills to help people re-frame negative thoughts and beliefs, while behaviour therapy aims to modify behaviour patterns by encouraging people with depression to engage in pleasurable and rewarding activities. Reminiscence therapy supports older people to reflect on positive or shared memories, and helps them find meaning in their life history.
The therapies were delivered by a range of professionals, including psychologists, social workers, occupational therapists and trainee therapists.
Cochrane AustraliaIn these studies, psychological therapies were compared to a control group where the older people did not receive psychological therapy. In most studies, this was “usual care” – the care typically provided to aged care residents, which may include access to antidepressants, scheduled activities and help with day-to-day tasks.
In some studies psychological therapy was compared to a situation where the older people received extra social contact, such as visits from a volunteer or joining in a discussion group.
What we found
Our results showed psychological therapies may be effective in reducing symptoms of depression for older people in residential aged care, compared with usual care, with effects lasting up to six months. While we didn’t see the same effect beyond six months, only two of the studies in our review followed people for this length of time, so the data was limited.
Our findings suggest these therapies may also improve quality of life and psychological wellbeing.
Psychological therapies mostly included between two and ten sessions, so the interventions were relatively brief. This is positive in terms of the potential feasibility of delivering psychological therapies at scale. The three different therapy types all appeared to be effective, compared to usual care.
However, we found psychological therapy may not be more effective than extra social contact in reducing symptoms of depression. Older people commonly feel bored, lonely and socially isolated in aged care. The activities on offer are often inadequate to meet their needs for stimulation and interest. So identifying ways to increase meaningful engagement day-to-day could improve the mental health and wellbeing of older people in aged care.
Some limitations
Many of the studies we found were of relatively poor quality, because of small sample sizes and potential risk of bias, for example. So we need more high-quality research to increase our confidence in the findings.
Many of the studies we reviewed were also old, and important gaps remain. For example, we are yet to understand the effectiveness of psychological therapies for people from diverse cultural or linguistic backgrounds.
Separately, we need better research to evaluate the effectiveness of antidepressants among aged care residents.
What needs to happen now?
Depression should not be considered a “normal” experience at this (or any other) stage of life, and those experiencing symptoms should have equal access to a range of effective treatments. The royal commission into aged care highlighted that Australians living in aged care don’t receive enough mental health support and called for this issue to be addressed.
While there have been some efforts to provide psychological services in residential aged care, the unmet need remains very high, and much more must be done.
The focus now needs to shift to how to implement psychological therapies in aged care, by increasing the competencies of the aged care workforce, training the next generation of psychologists to work in this setting, and funding these programs in a cost-effective way.

Tanya Davison, Adjunct professor, Health & Ageing Research Group, Swinburne University of Technology and Sunil Bhar, Professor of Clinical Psychology, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Widen the Window – by Dr. Elizabeth Stanley
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Firstly, about the title… That “window” that the author bids us “widen” is not a flowery metaphor, but rather, is referring to the window of exhibited resilience to stress/trauma; the “window” in question looks like an “inverted U” bell-curve on the graph.
In other words: Dr. Stanley’s main premise here is that we respond best to moderate stress (i.e: in that window, the area under the curve!), but if there is too little or too much, we don’t do so well. The key, she argues, is widening that middle part (expanding the area under the curve) in which we perform optimally. That way, we can still function in a motivated fashion without extrinsic threats, and we also don’t collapse under the weight of overwhelm, either.
The main strength of this book, however, lies in its practical exercises to accomplish that—and more.
“And more”, because the subtitle also promised recovery from trauma, and the author delivers in that regard too. In this case, it’s about widening that same window, but this time to allow one’s parasympathetic nervous system to recognize that the traumatic event is behind us, and no longer a threat; we are safe now.
Bottom line: if you would like to respond better to stress, and/or recover from trauma, this book is a very good tool.
Share This Post

Related Posts
-
What Causes Yeast Infections, & How To Get Rid Of Them?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Liesbeth Demuyser explains:
The fungus among us
The vaginal microbiome is host to countless microorganisms, with Lactobacilli being especially prevalent, which is good because they produce acid that lowers pH and prevents infections.
Candida yeasts (so, fungus) are normally present in small quantities, and/but kept in check by the immune system and competing microbes like the aforementioned Lactobacilli.
If the vaginal microbiome is disrupted, then C. albicans (the most commonly bothersome form of Candida) will shift into disease-causing forms, multiply, form hyphae, secrete enzymes that damage epithelial tissue, and trigger immune responses that cause itching, burning, swelling, redness, and thicker white discharge.
Things that can cause/promote this: antibiotics reduce protective Lactobacilli, lowered immunity allows overgrowth, hormonal changes and diet alter balance, semen raises pH, tight/wet clothing retains moisture, and soaps damage the protective mucus and physically wash out bacteria that should be there (while leaving the Candida relatively unbothered).
Avoiding problems: when it comes to hygiene down there, generally speaking “less is more”. Let the vagina do its thing without interference, and wash the vulva gently without special chemicals (including: without greenwashed chemicals that the “special cleansing crystals” or something, but in fact throw the pH way out (because they are salts, and bases) and kill a lot of bacteria that should be there (while, once again, leaving the Candida relatively unbothered).
Treating problems: most infections are mild, clear by themselves within two weeks if left alone, and/or respond well to antifungal medications; probiotics can help but are very hit-and-miss.
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Vaginal Probiotics: What Does The Science Say?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Using the”Task Zero” approach
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Jonathan Frakes Asks You Things” Voice:
- Do you ever find yourself in a room and wonder what you’re doing there?
- Or set about a to-do list, but get quickly distracted by side-quests?
- Finally get through to a person in a call center, they ask how they can help, and your mind goes blank?
- Go to the supermarket and come out with six things, none of which were the one you came for?
This is a “working memory” thing and you’re not alone. There’s a trick that can help keep you on track more often than not:
Don’t try to overburden your working memory. It is very limited (this goes for everyone to a greater or lesser degree). Instead, hold only two tasks at once:
- Task zero (what you are doing right now)
- Task one (your next task)
When you’ve completed task zero, task one becomes the new task zero, and you can populate a new task one from your to-do list.
This way, you will always know what you’re doing right now, and what you’re doing next, and your focus will be so intent on task zero, that you will not get sidetracked by task seventeen!
Happy focusing
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
“Skinny Fat” Explained (& How To Fix It)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Skinny fat” is a term you may have seen floating around social media. It describes people who have a low body weight but a high body fat percentage, often resulting in flabby appearance despite being within a weight range considered healthy. Many try dieting and exercising, only to find that neither work.
This video explains what’s going wrong, and how to fix it:
Diet & exercise won’t work if it’s not right
This problem occurs because common weight-loss approaches, such as restrictive dieting and excessive cardio, fail to improve body composition:
- Restrictive dieting reduces both fat and lean mass, keeping the body fat percentage unchanged
- Cardio burns some calories but the underlying metabolic issue hasn’t meaningfully changed, so any loss will be temporary (and most of any immediate loss will be water weight, anyway)
The key to overcoming skinny fat is resistance training. Lifting weights or doing bodyweight exercises helps build muscle, which not only lowers body fat percentage (by simple mathematics; add more muscle and the percentages of other things must go down even if the total amount is the same) and improves overall definition, which is something most people consider nice. However, the real value here is that it actually addresses the underlying metabolic issue—because muscle costs calories to maintain, one’s basal metabolic rate will now be faster, even when you’re sleeping.
This then becomes… Not quite a self-sustaining system, because you do have to still eat well and continue to do resistance training, but your body will be doing most of the work for you, and you’ll find it’s a lot easier to maintain a healthy body composition than to get one in the first place, for exactly the metabolic reason we described.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Visceral Belly Fat & How To Lose It ← this is a different, but adjacent issue (and very important for avoiding metabolic disease risks)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: