Half of Australians in aged care have depression. Psychological therapy could help
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
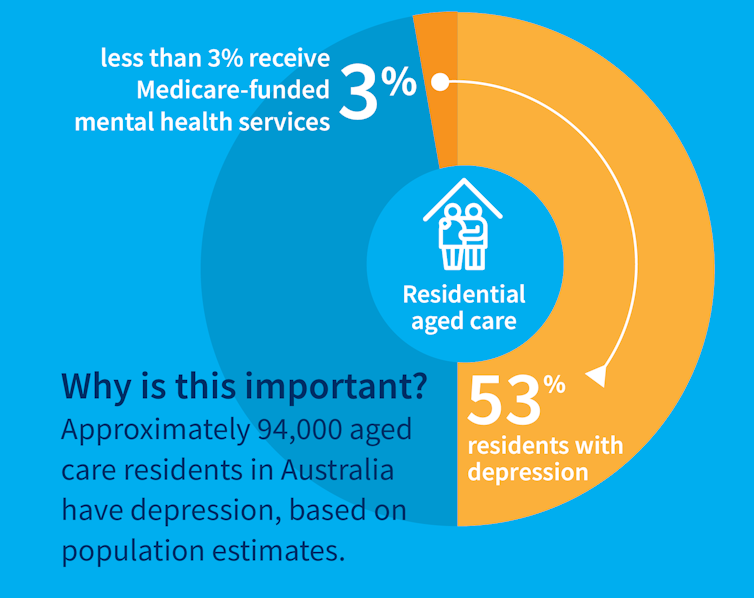
While many people maintain positive emotional wellbeing as they age, around half of older Australians living in residential aged care have significant levels of depression. Symptoms such as low mood, lack of interest or pleasure in life and difficulty sleeping are common.
Rates of depression in aged care appear to be increasing, and without adequate treatment, symptoms can be enduring and significantly impair older adults’ quality of life.
But only a minority of aged care residents with depression receive services specific to the condition. Less than 3% of Australian aged care residents access Medicare-subsidised mental health services, such as consultations with a psychologist or psychiatrist, each year.
Cochrane Australia
Instead, residents are typically prescribed a medication by their GP to manage their mental health, which they often take for several months or years. A recent study found six in ten Australian aged care residents take antidepressants.
While antidepressant medications may help many people, we lack robust evidence on whether they work for aged care residents with depression. Researchers have described “serious limitations of the current standard of care” in reference to the widespread use of antidepressants to treat frail older people with depression.
Given this, we wanted to find out whether psychological therapies can help manage depression in this group. These treatments address factors contributing to people’s distress and provide them with skills to manage their symptoms and improve their day-to-day lives. But to date researchers, care providers and policy makers haven’t had clear information about their effectiveness for treating depression among older people in residential aged care.
The good news is the evidence we published today suggests psychological therapies may be an effective approach for people living in aged care.
We reviewed the evidence
Our research team searched for randomised controlled trials published over the past 40 years that were designed to test the effectiveness of psychological therapies for depression among aged care residents 65 and over. We identified 19 trials from seven countries, including Australia, involving a total of 873 aged care residents with significant symptoms of depression.
The studies tested several different kinds of psychological therapies, which we classified as cognitive behavioural therapy (CBT), behaviour therapy or reminiscence therapy.
CBT involves teaching practical skills to help people re-frame negative thoughts and beliefs, while behaviour therapy aims to modify behaviour patterns by encouraging people with depression to engage in pleasurable and rewarding activities. Reminiscence therapy supports older people to reflect on positive or shared memories, and helps them find meaning in their life history.
The therapies were delivered by a range of professionals, including psychologists, social workers, occupational therapists and trainee therapists.
Cochrane Australia
In these studies, psychological therapies were compared to a control group where the older people did not receive psychological therapy. In most studies, this was “usual care” – the care typically provided to aged care residents, which may include access to antidepressants, scheduled activities and help with day-to-day tasks.
In some studies psychological therapy was compared to a situation where the older people received extra social contact, such as visits from a volunteer or joining in a discussion group.
What we found
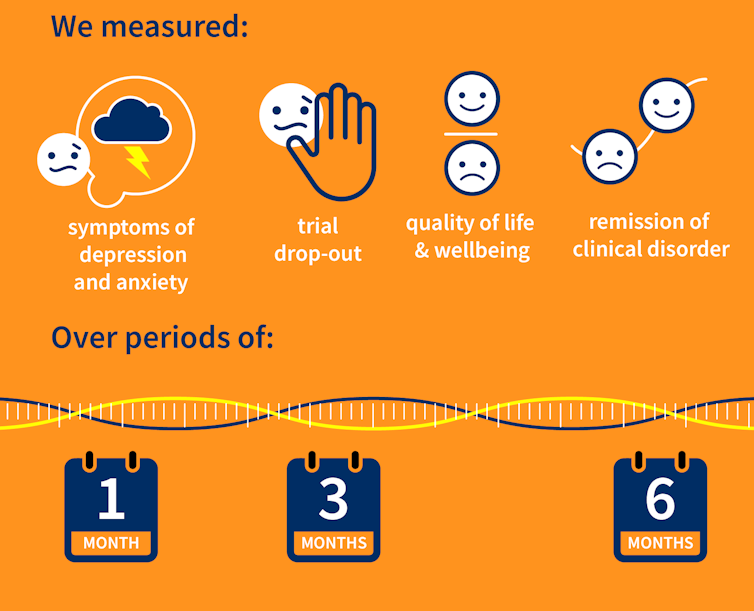
Our results showed psychological therapies may be effective in reducing symptoms of depression for older people in residential aged care, compared with usual care, with effects lasting up to six months. While we didn’t see the same effect beyond six months, only two of the studies in our review followed people for this length of time, so the data was limited.
Our findings suggest these therapies may also improve quality of life and psychological wellbeing.
Psychological therapies mostly included between two and ten sessions, so the interventions were relatively brief. This is positive in terms of the potential feasibility of delivering psychological therapies at scale. The three different therapy types all appeared to be effective, compared to usual care.
However, we found psychological therapy may not be more effective than extra social contact in reducing symptoms of depression. Older people commonly feel bored, lonely and socially isolated in aged care. The activities on offer are often inadequate to meet their needs for stimulation and interest. So identifying ways to increase meaningful engagement day-to-day could improve the mental health and wellbeing of older people in aged care.
Some limitations
Many of the studies we found were of relatively poor quality, because of small sample sizes and potential risk of bias, for example. So we need more high-quality research to increase our confidence in the findings.
Many of the studies we reviewed were also old, and important gaps remain. For example, we are yet to understand the effectiveness of psychological therapies for people from diverse cultural or linguistic backgrounds.
Separately, we need better research to evaluate the effectiveness of antidepressants among aged care residents.
What needs to happen now?
Depression should not be considered a “normal” experience at this (or any other) stage of life, and those experiencing symptoms should have equal access to a range of effective treatments. The royal commission into aged care highlighted that Australians living in aged care don’t receive enough mental health support and called for this issue to be addressed.
While there have been some efforts to provide psychological services in residential aged care, the unmet need remains very high, and much more must be done.
The focus now needs to shift to how to implement psychological therapies in aged care, by increasing the competencies of the aged care workforce, training the next generation of psychologists to work in this setting, and funding these programs in a cost-effective way. ![]()
Tanya Davison, Adjunct professor, Health & Ageing Research Group, Swinburne University of Technology and Sunil Bhar, Professor of Clinical Psychology, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Eye Drops That Instantly Correct Myopia With Just One Drop

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
These days, there are increasingly many ways to give our eyes medical attention. Laser surgery opened a lot of doors (not to mention cutting into the window to your soul and all that), and even that may be becoming obsolete as science marches on. That said, some methods still seem a little too exciting for complete comfort, such as: Laser Eye Surgery Without The Laser Or The Surgery! ← uses electrochemical corneal refraction to reshape it!
But what about eye drops? Taking them is not most people’s favorite hobby, but they can help with minor conditions; dry eyes being the most obvious. Yet even these being gradually sidelined as other technologies step forwards, for example: A New Free App Offers Relief For Dry Eyes (Yes, Really)
But they can do more complex things too, as we’ve written about before, such as: New Eye Drops vs Age-Related Macular Degeneration
So, what’s this about treating myopia with eye drops?
Let’s take a close-up look at the evidence
Researchers (Dr. Lisa Ostrin & Dr. Barsha Lal) investigated this, and found that a single low-dose atropine eye drop (0.01%–0.1%) caused significant improvements to pupil size and focusing ability that lasted at least 24 hours, while not changing eye length, retinal thickness, or choroidal thickness over that period (that’s good).
How they tested it: it was a small (n=20) randomized controlled trial (RCT), in which healthy adults (average age 25.5) received placebo or one of four atropine concentrations in one eye across five randomized, double-masked sessions, with measurements taken at baseline, 1 hour, and 24 hours.
The results, in numbers:
❝The superficial vascular plexus perfusion density in the 1.0–2.5 mm annulus showed significant decrease (P = 0.02) with time after atropine instillation, but not with concentration (P > 0.05); post hoc analysis showed significant decrease from baseline at 1 h (P = 0.03) compared to 24 h (P = 0.28)❞
In other words: it helps significantly, and quickly. However, the results are temporary, and meaning that while one drop per eye is sufficient to gain these changes for a day, it’d be necessary to take it again later to get the same effect again. On the other hand, the temporary nature of the effects does suggest a good safety profile.
Or as Dr. Ostrin herself put it:
❝Characterizing these short-term effects is important for a better understanding of the physiological responses to atropine in clinical and research settings.
By linking objective ocular responses with subjective visual experience, this work advances our understanding of how atropine works and supports more precise, evidence-based, and individualized approaches to myopia management❞
~ Dr. Lisa Ostrin, Professor of Optometry
You can read the paper in full, here: Short-term effects of atropine on the retina and choroid in young adults
Note: yes, “young adults” per the average age of 25.5 that we mentioned above, though there’s no reason to assume this won’t work similarly for older adults; that’s just the science that’s been done so far, and scientists like to claim only what they can be confident their study actually shows.
Not a fan of eye drops?
Well, first you might want to check out: Tips For Putting In Eye Drops (3 Techniques That Work!) ← this writer uses technique #3; how about you?
But if you want a no-med, entirely DIY approach to better eyesight, then do consider this highly recommendable book we reviewed a while back:
Vision for Life, Revised Edition: Ten Steps to Natural Eyesight Improvement – by Dr. Meir Schneider
Take care!
Share This Post
-
Menopause, & When Not To Let Your Guard Down
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Dr. Jessica Shepherd, a physician Fellow of the American College of Obstetricians & Gynecologists, CEO at Sanctum Medical & Wellness, and CMO at Hers.
She’s most well-known for her expertise in the field of the menopause. So, what does she want us to know?
Untreated menopause is more serious than most people think
Beyond the famous hot flashes, there’s also the increased osteoporosis risk, which is more well-known at least amongst the health-conscious, but oft-neglected is the increased cardiovascular disease risk:
What Menopause Does To The Heart
…and, which a lot of Dr. Shepherd’s work focuses on, it also increases dementia risk; she cites that 60–80% of dementia cases are women, and it’s also established that it progresses more quickly in women than men too, and this is associated with lower estrogen levels (not a problem for men, because testosterone does it for them) which had previously been a protective factor, but in untreated menopause, was no longer there to help:
Alzheimer’s Sex Differences May Not Be What They Appear
Treated menopause is safer than many people think
The Women’s Health Initiative (WHI) study, conducted in the 90s and published in 2002, linked HRT to breast cancer, causing fear, but it turned out that this was quite bad science in several ways and the reporting was even worse (even the flawed data did not really support the conclusion, much less the headlines); it was since broadly refuted (and in fact, it can be a protective factor, depending on the HRT regimen), but fearmongering headlines made it to mainstream news, whereas “oopsies, never mind, we take that back” didn’t.
The short version of the current state of the science is: breast cancer risk varies depending on age, HRT type, and dosage; some kinds of HRT can increase the risk marginally in those older than 60, but absolute risk is low compared to placebo, and taking estrogen alone can reduce risk at any age in the event of not having a uterus (almost always because of having had a hysterectomy; as a quirk, it is possible to be born without, though).
It’s worth noting that even in the cases where HRT marginally increased the risk of breast cancer, it significantly decreased the risk of cancers in total, as well fractures and all-cause-mortality compared to the placebo group.
In other words, it might be worth having a 0.12% risk of breast cancer, to avoid the >30% risk of osteoporosis, which can ultimately be just as fatal (without even looking at the other things the HRT is protective against).
However! In the case of those who already have (or have had) breast cancer, increasing estrogen levels can indeed make that worse/return, and it becomes more complicated in cases where you haven’t had it, but there is a family history of it, or you otherwise know you have the gene for it.
You can read more about HRT and breast cancer risk (increases and decreases) here:
…and about the same with regard to HMT, here:
The Hormone Therapy That Reduces Breast Cancer Risk & More
Lifestyle matters, and continues to matter
Menopause often receives the following attention from people:
- Perimenopause: “Is this menopause?”
- Menopause: “Ok, choices to make about HRT or not, plus I should watch out for osteoporosis”
- Postmenopause: “Yay, that’s behind me now, back to the new normal”
The reality, Dr. Shepherd advises, is that “postmenopause” is a misnomer because if it’s not being treated, then the changes are continuing to occur in your body.
This is a simple factor of physiology; your body is always rebuilding itself, will never stop until you die, and in untreated menopause+postmenopause, it’s now doing it without much estrogen.
So, you can’t let your guard down!
Thus, she recommends: focus on maintaining muscle mass, bone health, and cardiovascular health. If you focus on those things, the rest (including your brain, which is highly dependent on cardiovascular health) will mostly take care of itself.
Because falls and fractures, particularly hip fractures, drastically reduce quality and length of life in older adults, it is vital to avoid those, and try to be sufficiently robust so that if you do go A over T, you won’t injure yourself too badly, because your bones are strong. As a bonus, the same things (especially that muscle mass we talked about) will help you avoid falling in the first place, by improving stability.
See also: Resistance Is Useful! (Especially As We Get Older)
And about falls specifically: Fall Special: Be Robust, Mobile, & Balanced!
Want to know more from Dr. Shepherd?
You might like this book of hers that we reviewed not long back:
Generation M – by Dr. Jessica Shepherd
Take care!
Share This Post
-
5 Vaginal Estrogen Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Jennifer Roelands, gynecologist, explains:
Let’s get down to business
Here are the 5 myths busted:
- Vaginal estrogen causes cancer: vaginal estrogen does not increase cancer risk, including breast cancer; it doesn’t raise systemic hormone levels so your breasts won’t even know you’re taking it; even people with a history of breast cancer or blood clots can usually use it safely.
- Vaginal estrogen is only for older women: it’s useful for a wide range of people—including those who are postpartum, perimenopausal, those on certain medications, or with autoimmune or vulvar conditions—not just those in menopause.
- Vaginal estrogen is dangerous for your heart: vaginal estrogen doesn’t raise the risk of blood clots, stroke, or heart attack because it has minimal systemic absorption.
- Vaginal estrogen is hard to use: it comes in various user-friendly forms (e.g. cream, suppositories, ring, etc), and many can be applied easily without mess or complicated devices.
- You have to stop vaginal estrogen at a certain age: there’s no age limit; it can be safely used indefinitely to maintain vaginal and urinary health, including preventing infections and dryness.
Note: in some of these cases, Dr. Roelands compares the effects of topical vaginal estrogen with those of systemic HRT, mentioning multiple times that it’s safer because it’s not systemic. Now, that is true, but it’s worth noting that systemic HRT also does not increase cancer risk in most people, and it reduces (not increases) the risk of heart attack. Nothing is perfect though, and we will concede that it does increase thrombosis risk.
You can enjoy the video here:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
- HRT: A Tale Of Two Approaches ← explains how the “HRT causes cancer” myth came from a single methodologically flawed, since-refuted study that, as an extra consideration against it, didn’t even use modern bioidentical HRT that is even safer than ye olde Premarin and similar animal-derived estrogens.
- HRT & Your Heart ← explains how estrogen is, on balance, cardioprotective (including by improved lipids and vascular function), while still increasing thrombosis risk
- How Old Is Too Old For HRT? ← includes a simple test you can do to know whether it is too late for you or not
Take care!
Share This Post




-
How Regularity Of Sleep Can Be Even More Important Than Duration
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A recent, large (n=72,269) 8-year prospective* observational study of adults aged 40-79 has found an association between irregular sleep and major cardiovascular events.
*this means they started the study at a given point, and measured what happened for the next eight years—as opposed to a retrospective study, which would look at what had happened during the previous 8 years.
As to what qualifies as major cardiovascular events, they counted:
- Heart attack
- Cardiac arrest
- Stroke
- Cardiovascular death (any)
Irregular sleep, meanwhile, was defined per a bell curve of participants. Based on a sleep regularity index (SRI) score, those with a score of 87 or more were on the “regular” side of the curve, and those with a score of 72 or lower were on the “irregular” side of the curve.
What they found is that irregular sleep is associated with major cardiovascular events, regardless of the actual amount of sleep that people got. So in other words, you could be sleeping 9 hours per day, but if it’s a different 9 hours each day, your cardiovascular risk will still be higher.
How much higher?
- For those in the middle of the curve (so, moderate irregularity), it was 8% higher than those on the “regular” side.
- For those on the “irregular” side of the curve, it was 26% higher than those on the “regular” side.
All of the above is after taking into account confounding variables such as age, physical activity levels, discretionary screen time, fruit, vegetable, and coffee intake, alcohol consumption, smoking, mental health issues, medication use, and shift work. Which is quite something, given that shift work is a very common reason for irregular sleep schedules in a lot of people.
Limitations
While, as noted above, they did their best to account for a lot of things, this was an observational study, not an interventional study or a randomized controlled trial, and as such, it cannot truly establish cause and effect.
For example, an observational study in the 90s found that the sport most strongly associated with longevity was polo. For any unfamiliar, it’s a game played on horseback with mallets and balls. Why was this game so much better than, say, swimming? And the answer is most likely that polo is played almost entirely by very rich people. It wasn’t the sport that enhanced longevity—it was the wealth.
So similarly here, it could be for example that people who are predisposed to heart conditions, are prone to having irregular schedules. We won’t know for sure until we have interventional studies (and we probably can’t get RCTs for this, for practical reasons).
Still, it seems likely that the association is indeed causal, in which case, having a regular sleep schedule if at all possible seems like a very good way to look after one’s health.
You can read more about the study here:
Irregular sleep may elevate risk of major cardiovascular events
Practical take-away
This study strongly suggests that sleep regularity is even more important than sleep duration.
This means that there is extra reason to not sleep in past one’s normal getting-up time, even if one had a less restful night.
That’s the end of sleep that’s the most important in practical terms, too, because we can control our getting-up time, whereas we can’t really control our going-to-sleep time, because it’s perfectly possible to just lie there awake.
So, controlling the getting-up time is really the key to the whole thing. See also:
Calculate (And Enjoy) The Perfect Night’s Sleep
And for scope, you might enjoy reading:
Morning Larks vs Night Owls: How Much Can We Control Our Sleep Schedule?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Metabolism Reset Diet – by Alan Christianson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The liver is an incredible organ that does a very important job, but what’s not generally talked about is how we can help it… Beyond the obvious “try to not poison it too much with alcohol, tobacco, etc”. But what can we do that’s actually positive for it?
That’s what Alan Christianson offers in this book.
Now, usually when someone speaks of a “four week cleanse” as this book advertises on its front cover, it’s a lot of bunk. The liver cleanses itself, and the liver and kidneys between them (along with some other organs and processes) detoxify your body for you. No amount of celery juice will do that. However, this book does better than that:
What it’s about, is not really about trying to do a “detox” at all, so much as supporting your liver function by:
- Giving your liver what it needs to regenerate (mostly: protein)
- Not over-taxing your liver while it does so
The liver is a self-regenerating organ (the mythological story of Prometheus aside, here in real life it can regenerate up to 80% of itself, given the opportunity), so whatever the current state of your liver, it’s probably not too late to fix it.
Maybe you’ve been drinking a little too much, or maybe you’ve been taking some meds that have hobbled it a bit (some medications strain the liver rather), or maybe your diet hasn’t been great. Christianson invites you to draw a line under that, and move forwards:
The book gives an overview of the science involved, and explains about the liver’s role in metabolism (hence the promised weight loss benefits) and our dietary habits’ impact on liver function. This is about what we eat, and also about when we eat it, and how and when our body metabolizes that.
Christianson also provides meal ideas and recipes. If we’re honest (and we always are), the science/principles part of the book are worth a lot more than the meal-plan part of the book, though.
In short: a great book for understanding how the liver works and how we can help it do its job effectively.
Click here to check out “The Metabolism Reset Diet” on Amazon today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Yes, adults can develop food allergies. Here are 4 types you need to know about
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you didn’t have food allergies as a child, is it possible to develop them as an adult? The short answer is yes. But the reasons why are much more complicated.
Preschoolers are about four times more likely to have a food allergy than adults and are more likely to grow out of it as they get older.
It’s hard to get accurate figures on adult food allergy prevalence. The Australian National Allergy Council reports one in 50 adults have food allergies. But a US survey suggested as many as one in ten adults were allergic to at least one food, with some developing allergies in adulthood.
What is a food allergy
Food allergies are immune reactions involving immunoglobulin E (IgE) – an antibody that’s central to triggering allergic responses. These are known as “IgE-mediated food allergies”.
Food allergy symptoms that are not mediated by IgE are usually delayed reactions and called food intolerances or hypersensitivity.
Food allergy symptoms can include hives, swelling, difficulty swallowing, vomiting, throat or chest tightening, trouble breathing, chest pain, rapid heart rate, dizziness, low blood pressure or anaphylaxis.

Symptoms include hives. wisely/Shutterstock IgE-mediated food allergies can be life threatening, so all adults need an action management plan developed in consultation with their medical team.
Here are four IgE-mediated food allergies that can occur in adults – from relatively common ones to rare allergies you’ve probably never heard of.
1. Single food allergies
The most common IgE-mediated food allergies in adults in a US survey were to:
- shellfish (2.9%)
- cow’s milk (1.9%)
- peanut (1.8%)
- tree nuts (1.2%)
- fin fish (0.9%) like barramundi, snapper, salmon, cod and perch.
In these adults, about 45% reported reacting to multiple foods.
This compares to most common childhood food allergies: cow’s milk, egg, peanut and soy.
Overall, adult food allergy prevalence appears to be increasing. Compared to older surveys published in 2003 and 2004, peanut allergy prevalence has increased about three-fold (from 0.6%), while tree nuts and fin fish roughly doubled (from 0.5% each), with shellfish similar (2.5%).
While new adult-onset food allergies are increasing, childhood-onset food allergies are also more likely to be retained into adulthood. Possible reasons for both include low vitamin D status, lack of immune system challenges due to being overly “clean”, heightened sensitisation due to allergen avoidance, and more frequent antibiotic use.
Some adults develop allergies to cow’s milk, while others retain their allergy from childhood. Sarah Swinton/Unsplash 2. Tick-meat allergy
Tick-meat allergy, also called α-Gal syndrome or mammalian meat allergy, is an allergic reaction to galactose-alpha-1,3-galactose, or α-Gal for short.
Australian immunologists first reported links between α-Gal syndrome and tick bites in 2009, with cases also reported in the United States, Japan, Europe and South Africa. The US Centers for Disease Control estimates about 450,000 Americans could be affected.
The α-Gal contains a carbohydrate molecule that is bound to a protein molecule in mammals.
The IgE-mediated allergy is triggered after repeated bites from ticks or chigger mites that have bitten those mammals. When tick saliva crosses into your body through the bite, antibodies to α-Gal are produced.
When you subsequently eat foods that contain α-Gal, the allergy is triggered. These triggering foods include meat (lamb, beef, pork, rabbit, kangaroo), dairy products (yoghurt, cheese, ice-cream, cream), animal-origin gelatin added to gummy foods (jelly, lollies, marshmallow), prescription medications and over-the counter supplements containing gelatin (some antibiotics, vitamins and other supplements).
Tick-meat allergy reactions can be hard to recognise because they’re usually delayed, and they can be severe and include anaphylaxis. Allergy organisations produce management guidelines, so always discuss management with your doctor.
3. Fruit-pollen allergy
Fruit-pollen allergy, called pollen food allergy syndrome, is an IgE-mediated allergic reaction.
In susceptible adults, pollen in the air provokes the production of IgE antibodies to antigens in the pollen, but these antigens are similar to ones found in some fruits, vegetables and herbs. The problem is that eating those plants triggers an allergic reaction.
The most allergenic tree pollens are from birch, cypress, Japanese cedar, latex, grass, and ragweed. Their pollen can cross-react with fruit and vegetables, including kiwi, banana, mango, avocado, grapes, celery, carrot and potato, and some herbs such as caraway, coriander, fennel, pepper and paprika.
Fruit-pollen allergy is not common. Prevalence estimates are between 0.03% and 8% depending on the country, but it can be life-threatening. Reactions range from itching or tingling of lips, mouth, tongue and throat, called oral allergy syndrome, to mild hives, to anaphylaxis.
4. Food-dependent, exercise-induced food allergy
During heavy exercise, the stomach produces less acid than usual and gut permeability increases, meaning that small molecules in your gut are more likely to escape across the membrane into your blood. These include food molecules that trigger an IgE reaction.
If the person already has IgE antibodies to the foods eaten before exercise, then the risk of triggering food allergy reactions is increased. This allergy is called food-dependent exercise-induced allergy, with symptoms ranging from hives and swelling, to difficulty breathing and anaphylaxis.
This type of allergy is extremely rare. Ben O’Sullivan/Unsplash Common trigger foods include wheat, seafood, meat, poultry, egg, milk, nuts, grapes, celery and other foods, which could have been eaten many hours before exercising.
To complicate things even further, allergic reactions can occur at lower levels of trigger-food exposure, and be more severe if the person is simultaneously taking non-steroidal inflammatory medications like aspirin, drinking alcohol or is sleep-deprived.
Food-dependent exercise-induced allergy is extremely rare. Surveys have estimated prevalence as between one to 17 cases per 1,000 people worldwide with the highest prevalence between the teenage years to age 35. Those affected often have other allergic conditions such as hay fever, asthma, allergic conjunctivitis and dermatitis.
Allergies are a growing burden
The burden on physical health, psychological health and health costs due to food allergy is increasing. In the US, this financial burden was estimated as $24 billion per year.
Adult food allergy needs to be taken seriously and those with severe symptoms should wear a medical information bracelet or chain and carry an adrenaline auto-injector pen. Concerningly, surveys suggest only about one in four adults with food allergy have an adrenaline pen.
If you have an IgE-mediated food allergy, discuss your management plan with your doctor. You can also find more information at Allergy and Anaphylaxis Australia.
Clare Collins, Laureate Professor in Nutrition and Dietetics, University of Newcastle
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: