Brussels Sprouts vs Spirulina – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing Brussels sprouts to spirulina, we picked the sprouts.
Why?
Pitting these two well-known superfoods against each other, we get the following:
Looking at the macros first, spirulina has a little more protein, while sprouts have more carbs and nearly 10x the fiber. So, we call this a win for sprouts.
In terms of vitamins, sprouts have a lot more of vitamins A, B6, B9, C, E, K, and choline, while spirulina has a little more of vitamins B1, B2, and B3. An easy win for sprouts.
In the category of minerals, sprouts have more calcium, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while spirulina has more copper and iron. Another clear win for sprouts.
Adding up the sections makes the winner very clear: Brussels sprouts enjoy a well-earned victory.
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Body on Fire – by Dr. Monica Aggarwal and Dr. Jyothi Rao

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are times when you do really need a doctor, not a dietician. But there are also times when a doctor will prescribe something for the symptom, leaving the underlying issue untouched. If only there were a way to have the best of both worlds!
That’s where Drs. Rao and Aggarwal come in. They’re both medical doctors… with a keen interest in nutrition and healthy lifestyle changes to make us less sick such that we have less need to go to the doctor at all.
Best of all, they understand—while some things are true for everyone—there’s not a one-size-fits all diet or exercise regime or even sleep setup.
So instead, they take us hand-in-hand (chapter by chapter!) through the various parts of our life (including our diet) that might need tweaking. Each of these changes, if taken up, promise a net improvement that becomes synergistic with the other changes. There’s a degree of biofeedback involved, and listening to your body, to be sure of what’s really best for you, not what merely should be best for you on paper.
The writing style is accessible while science-heavy. They don’t assume prior knowledge, and/but they sure deliver a lot. The book is more text than images, but there are plenty of medical diagrams, explanations, charts, and the like. You will feed like a medical student! And it’s very much worth studying.
Bottom line: highly recommendable even if you don’t have inflammation issues, and worth its weight in gold if you do.
Share This Post
-
This is a Levantine dish, Syrian in origin (although Lebanese cuisine uses it plenty too) and popularly enjoyed all the way up to Turkey, down to Egypt, and across to Armenia. And today, perhaps rather further afield! It’s first and foremost a spicy dip/spread, though it can be lengthened into a sauce, and/or made more substantial by adding an extra protein. We’ll give you the basic recipe though, and let you see where it takes you! Healthwise, it’s very nutritionally dense, mostly thanks to the walnuts and red peppers, though spices and olive oil bring their healthy benefits too.
You will need
- ½ cup chopped walnuts (ideally: toasted)
- 3 red peppers, from a jar (jarred over fresh not only improves the consistency, but also makes it extra gut-healthy due to the fermentation bacteria present; if you must use fresh, roast them first)
- 2 tbsp extra virgin olive oil
- 1 tbsp pomegranate molasses (you can omit if you don’t like sweetness, but this is traditional)
- 1 tbsp tomato purée
- 1 tbsp Aleppo pepper flakes (less, if you don’t like heat) (substitute another hot pepper if necessary)
- ½ bulb garlic, crushed
- 2 tsp ground smoked paprika
- 1 tsp ground cumin
- ½ tsp MSG or 1 tsp low-sodium salt
- Juice of 1 lemon
- Optional: handful of pomegranate seeds
- Optional: herb garnish, e.g. cilantro or parsley
Method
(we suggest you read everything at least once before doing anything)
1) Add everything except the pomegranate seeds and herbs to a blender, and blend to a smooth consistency.
2) Add the pomegranate seeds and herbs, as a garnish.
3) Serve! Can be enjoyed as a dip (perhaps using our Homemade Healthy Flatbreads recipe), or as a spread, or used as a sauce poured over chickpeas or some other bulky protein, to make a more substantial dish.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Walnuts vs Cashews – Which is Healthier?
- Capsaicin For Weight Loss And Against Inflammation
- Red Bell Peppers vs Tomatoes – Which is Healthier?
- Bell Peppers: A Spectrum Of Specialties
- Lycopene’s Benefits For The Gut, Heart, Brain, & More
Take care!
Share This Post
-

Butter vs Margarine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Butter vs Margarine

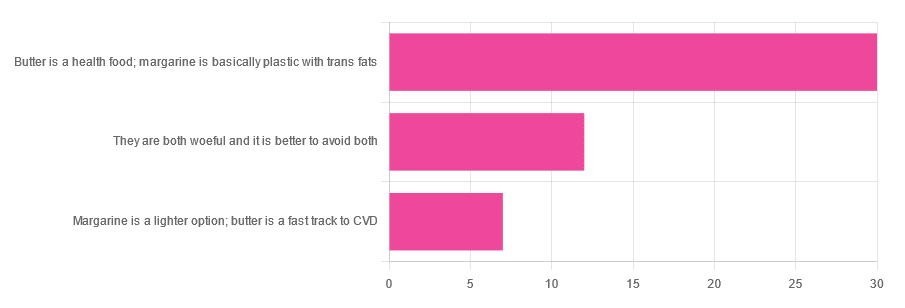
Yesterday, we asked you for your (health-related) opinion on butter vs margarine, and got the above-depicted, below-described, set of responses:
- A little over 60% said butter is a health food and margarine is basically plastic with trans fats
- A little over 20% said that both are woeful and it’s better to avoid both
- A little over 10% said that margarine is a lighter option, and butter is a fast track to cardiovascular disease.
Comments included (we will summarize/paraphrase, for space):
- “…in moderation, though”
- “I’m vegan so I use vegan butter but I know it’s not great, so I use it sparingly”
- “butter is healthy if and only if it’s grass-fed”
- “margarine has unpronounceable ingredients”
To address those quickly:
- “…in moderation” is a stipulation with which one can rarely go too far wrong
- Same! Speaking for myself (your writer here, hi) and not for the company
- Grass-fed is indeed better; alas that so little of it is grass-fed, in the US!
- Butter contains eicosatrienoic acid, linolelaidic acid, and more*. Sometimes big words don’t mean that something is worse for the health, though!
So, what does the science say?
Butter is a health food: True or False?
True or False, depending on amount! Moderation is definitely key, but we’ll return to that (and why not to have more than a small amount of butter) later. But it is a rich source of many nutrients, iff it’s grass-fed, anyway.
The nutritional profile of something isn’t a thing that’s too contentious, so rather than take too much time on it, in this case we’ll point you back up to the scientific paper we linked above, or if you prefer a pop-science rendering, here’s a nice quick rundown:
7 Reasons to Switch to Grass-Fed Butter
Margarine is basically plastic with trans fats: True or False?
False and usually False now, respectively, contingently.
On the first part: chemically, it’s simply not “basically plastic” and everything in it is digestible
On the second part: it depends on the margarine, and here’s where it pays to read labels. Historically, margarines all used to be high in trans fats (which are indeed woeful for the health). Nowadays, since trans fats have such a (well-earned) bad press, there are increasingly many margarines with low (or no) trans fats, and depending on your country, it may be that all margarines no longer have such:
❝It’s a public health success story. Consumers no longer have to worry about reading product nutritional labels to see if they contain hydrogenated oils and trans fats. They can just know that they no longer do❞
Source: Margarines now nutritionally better than butter after hydrogenated oil ban
So this is one where the science is clear (trans fats are unequivocally bad), but the consumer information is not always (it may be necessary to read labels, to know whether a margarine is conforming to the new guidelines).
Butter is a fast track to cardiovascular disease: True or False?
True or False depending on amount. In moderation, predictably it’s not a big deal.
But for example, the World Health Organization recommends that saturated fats (of which butter is a generous source) make up no more than 10% of our calorie intake:
Source: Saturated fatty acid and trans-fatty acid intake for adults and children: WHO guideline
So if you have a 2000 kcal daily intake, that would mean consuming not more than 200 kcal from butter, which is approximately two tablespoons.
If you’d like a deeper look into the complexities of saturated fats (for and against), you might like our previous main feature specifically about such:
Can Saturated Fats Be Healthy?
Enjoy!
Share This Post

Related Posts
-

What pathogen might spark the next pandemic? How scientists are preparing for ‘disease X’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Before the COVID pandemic, the World Health Organization (WHO) had made a list of priority infectious diseases. These were felt to pose a threat to international public health, but where research was still needed to improve their surveillance and diagnosis. In 2018, “disease X” was included, which signified that a pathogen previously not on our radar could cause a pandemic.
While it’s one thing to acknowledge the limits to our knowledge of the microbial soup we live in, more recent attention has focused on how we might systematically approach future pandemic risks.
Former US Secretary of Defense Donald Rumsfeld famously talked about “known knowns” (things we know we know), “known unknowns” (things we know we don’t know), and “unknown unknowns” (the things we don’t know we don’t know).
Although this may have been controversial in its original context of weapons of mass destruction, it provides a way to think about how we might approach future pandemic threats.

Anna Shvets/Pexels Influenza: a ‘known known’
Influenza is largely a known entity; we essentially have a minor pandemic every winter with small changes in the virus each year. But more major changes can also occur, resulting in spread through populations with little pre-existing immunity. We saw this most recently in 2009 with the swine flu pandemic.
However, there’s a lot we don’t understand about what drives influenza mutations, how these interact with population-level immunity, and how best to make predictions about transmission, severity and impact each year.
The current H5N1 subtype of avian influenza (“bird flu”) has spread widely around the world. It has led to the deaths of many millions of birds and spread to several mammalian species including cows in the United States and marine mammals in South America.
Human cases have been reported in people who have had close contact with infected animals, but fortunately there’s currently no sustained spread between people.
While detecting influenza in animals is a huge task in a large country such as Australia, there are systems in place to detect and respond to bird flu in wildlife and production animals.
Scientists are continually monitoring a range of pathogens with pandemic potential. Edward Jenner/Pexels It’s inevitable there will be more influenza pandemics in the future. But it isn’t always the one we are worried about.
Attention had been focused on avian influenza since 1997, when an outbreak in birds in Hong Kong caused severe disease in humans. But the subsequent pandemic in 2009 originated in pigs in central Mexico.
Coronaviruses: an ‘unknown known’
Although Rumsfeld didn’t talk about “unknown knowns”, coronaviruses would be appropriate for this category. We knew more about coronaviruses than most people might have thought before the COVID pandemic.
We’d had experience with severe acute respiratory syndrome (SARS) and Middle Eastern respiratory syndrome (MERS) causing large outbreaks. Both are caused by viruses closely related to SARS-CoV-2, the coronavirus that causes COVID. While these might have faded from public consciousness before COVID, coronaviruses were listed in the 2015 WHO list of diseases with pandemic potential.
Previous research into the earlier coronaviruses proved vital in allowing COVID vaccines to be developed rapidly. For example, the Oxford group’s initial work on a MERS vaccine was key to the development of AstraZeneca’s COVID vaccine.
Similarly, previous research into the structure of the spike protein – a protein on the surface of coronaviruses that allows it to attach to our cells – was helpful in developing mRNA vaccines for COVID.
It would seem likely there will be further coronavirus pandemics in the future. And even if they don’t occur at the scale of COVID, the impacts can be significant. For example, when MERS spread to South Korea in 2015, it only caused 186 cases over two months, but the cost of controlling it was estimated at US$8 billion (A$11.6 billion).
COVID could be regarded as an ‘unknown known’. Markus Spiske/Pexels The 25 viral families: an approach to ‘known unknowns’
Attention has now turned to the known unknowns. There are about 120 viruses from 25 families that are known to cause human disease. Members of each viral family share common properties and our immune systems respond to them in similar ways.
An example is the flavivirus family, of which the best-known members are yellow fever virus and dengue fever virus. This family also includes several other important viruses, such as Zika virus (which can cause birth defects when pregnant women are infected) and West Nile virus (which causes encephalitis, or inflammation of the brain).
The WHO’s blueprint for epidemics aims to consider threats from different classes of viruses and bacteria. It looks at individual pathogens as examples from each category to expand our understanding systematically.
The US National Institute of Allergy and Infectious Diseases has taken this a step further, preparing vaccines and therapies for a list of prototype pathogens from key virus families. The goal is to be able to adapt this knowledge to new vaccines and treatments if a pandemic were to arise from a closely related virus.
Pathogen X, the ‘unknown unknown’
There are also the unknown unknowns, or “disease X” – an unknown pathogen with the potential to trigger a severe global epidemic. To prepare for this, we need to adopt new forms of surveillance specifically looking at where new pathogens could emerge.
In recent years, there’s been an increasing recognition that we need to take a broader view of health beyond only thinking about human health, but also animals and the environment. This concept is known as “One Health” and considers issues such as climate change, intensive agricultural practices, trade in exotic animals, increased human encroachment into wildlife habitats, changing international travel, and urbanisation.
This has implications not only for where to look for new infectious diseases, but also how we can reduce the risk of “spillover” from animals to humans. This might include targeted testing of animals and people who work closely with animals. Currently, testing is mainly directed towards known viruses, but new technologies can look for as yet unknown viruses in patients with symptoms consistent with new infections.
We live in a vast world of potential microbiological threats. While influenza and coronaviruses have a track record of causing past pandemics, a longer list of new pathogens could still cause outbreaks with significant consequences.
Continued surveillance for new pathogens, improving our understanding of important virus families, and developing policies to reduce the risk of spillover will all be important for reducing the risk of future pandemics.
This article is part of a series on the next pandemic.
Allen Cheng, Professor of Infectious Diseases, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Hawthorn For The Heart (& More)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hawthorn, The Heart-Healthy Helper
Hawthorn, a berry of the genus Crataegus (there are many species, but they seem to give more or less the same benefits), has been enjoyed for hundreds of years, if not thousands, as a herbal remedy for many ailments, mostly of the cardiovascular, digestive, and/or endocrine systems:
Crataegus pinnatifida: Chemical Constituents, Pharmacology, and Potential Applications
Antioxidant & Anti-inflammatory
Like most berries, it’s full of helpful polyphenols, with antioxidant and anti-inflammatory properties. Indeed, as Dr. Nabavi et al. wrote,
❝Crataegus monogyna Jacq. (hawthorn) is one of the most important edible plants of the Rosaceae family and is also used in traditional medicine.
Growing evidence has shown that this plant has various interesting physiological and pharmacological activities due to the presence of different bioactive natural compounds.
In addition, scientific evidence suggests that the toxicity of hawthorn is negligible. ❞
Read in full: Polyphenolic Composition of Crataegus monogyna Jacq.: From Chemistry to Medical Applications
While “the toxicity of hawthorn is negligible” may be reasonably considered a baseline for recommending an edible plant, it’s still important as just that: a baseline. It’s good to know that berries are safe, after all!
More positively, about those antioxidant and anti-inflammatory properties:
This one was a mouse study, but it’s important as it about modulating liver injury after being fed a high fructose diet.
In other words: it a) helps undo the biggest cause of non-alcoholic fatty liver disease, b) logically, likely guards against diabetes also (by the same mechanism)
Anti-Diabetes Potential
Curious about that latter point, we looked for studies, and found, for example:
- Hypoglycemic effect of hawthorn in type II diabetes mellitus rat model
- Molecular Mechanisms of Hawthorn Extracts in Multiple Organs Disorders in Underlying of Diabetes: A Review
- Modulation of GPC-4 and GPLD1 serum levels by improving glycemic indices in type 2 diabetes: Resistance training and hawthorn extract intervention
Noteworthily, those studies are from the past couple of years, which is probably why we’re not seeing many human trials for this yet—everything has to be done in order, and there’s a lengthy process between each.
We did find some human trials with hawthorn in diabetes patients, for example:
…but as you see, that’s testing not its antidiabetic potential, so far demonstrated only in mice and rats (so far as we could find), but rather its blood pressure lowering effects, using diabetic patients as a sample.
Blood pressure benefits
Hawthorn has been studied specifically for its hypotensive effect, for example:
As an extra bonus, did you notice in the conclusion,
❝Furthermore, a trend towards a reduction in anxiety (p = 0.094) was also observed in those taking hawthorn compared with the other groups.
These findings warrant further study, particularly in view of the low dose of hawthorn extract used.❞
…it seems that not a lot more study has been done yet, but that is promising too!
Other blood metrics
So, it has antidiabetic and antihypertensive benefits, what of blood lipids?
Hawthorn Fruit Extract Elevates Expression of Nrf2/HO-1 and Improves Lipid Profiles
And as for arterial plaque?
here it was tested alongside another herb, and performed well (also against placebo).
In summary…
Hawthorn (Crataegus sp.) is…
- a potent berry containing many polyphenols with good antioxidant and anti-inflammatory effects
- looking promising against diabetes, but research for this is still in early stages
- found to have other cardioprotective effects (antihypertensive, improves lipid profiles), too
- considered to have negligible toxicity
Where can I get it?
As ever, we don’t sell it, but here for your convenience is an example product on Amazon
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What happens when I stop taking a drug like Ozempic or Mounjaro?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hundreds of thousands of people worldwide are taking drugs like Ozempic to lose weight. But what do we actually know about them? This month, The Conversation’s experts explore their rise, impact and potential consequences.
Drugs like Ozempic are very effective at helping most people who take them lose weight. Semaglutide (sold as Wegovy and Ozempic) and tirzepatide (sold as Zepbound and Mounjaro) are the most well known in the class of drugs that mimic hormones to reduce feelings of hunger.
But does weight come back when you stop using it?
The short answer is yes. Stopping tirzepatide and semaglutide will result in weight regain in most people.
So are these medications simply another (expensive) form of yo-yo dieting? Let’s look at what the evidence shows so far.
It’s a long-term treatment, not a short course
If you have a bacterial infection, antibiotics will help your body fight off the germs causing your illness. You take the full course of medication, and the infection is gone.
For obesity, taking tirzepatide or semaglutide can help your body get rid of fat. However it doesn’t fix the reasons you gained weight in the first place because obesity is a chronic, complex condition. When you stop the medications, the weight returns.
Perhaps a more useful comparison is with high blood pressure, also known as hypertension. Treatment for hypertension is lifelong. It’s the same with obesity. Medications work, but only while you are taking them. (Though obesity is more complicated than hypertension, as many different factors both cause and perpetuate it.)
Obesity drugs only work while you’re taking them. KK Stock/Shutterstock Therefore, several concurrent approaches are needed; taking medication can be an important part of effective management but on its own, it’s often insufficient. And in an unwanted knock-on effect, stopping medication can undermine other strategies to lose weight, like eating less.
Why do people stop?
Research trials show anywhere from 6% to 13.5% of participants stop taking these drugs, primarily because of side effects.
But these studies don’t account for those forced to stop because of cost or widespread supply issues. We don’t know how many people have needed to stop this medication over the past few years for these reasons.
Understanding what stopping does to the body is therefore important.
So what happens when you stop?
When you stop using tirzepatide or semaglutide, it takes several days (or even a couple of weeks) to move out of your system. As it does, a number of things happen:
- you start feeling hungry again, because both your brain and your gut no longer have the medication working to make you feel full
When you stop taking it, you feel hungry again. Stock-Asso/Shutterstock - blood sugars increase, because the medication is no longer acting on the pancreas to help control this. If you have diabetes as well as obesity you may need to take other medications to keep these in an acceptable range. Whether you have diabetes or not, you may need to eat foods with a low glycemic index to stabilise your blood sugars
- over the longer term, most people experience a return to their previous blood pressure and cholesterol levels, as the weight comes back
- weight regain will mostly be in the form of fat, because it will be gained faster than skeletal muscle.
While you were on the medication, you will have lost proportionally less skeletal muscle than fat, muscle loss is inevitable when you lose weight, no matter whether you use medications or not. The problem is, when you stop the medication, your body preferentially puts on fat.
Is stopping and starting the medications a problem?
People whose weight fluctuates with tirzepatide or semaglutide may experience some of the downsides of yo-yo dieting.
When you keep going on and off diets, it’s like a rollercoaster ride for your body. Each time you regain weight, your body has to deal with spikes in blood pressure, heart rate, and how your body handles sugars and fats. This can stress your heart and overall cardiovascular system, as it has to respond to greater fluctuations than usual.
Interestingly, the risk to the body from weight fluctuations is greater for people who are not obese. This should be a caution to those who are not obese but still using tirzepatide or semaglutide to try to lose unwanted weight.
How can you avoid gaining weight when you stop?
Fear of regaining weight when stopping these medications is valid, and needs to be addressed directly. As obesity has many causes and perpetuating factors, many evidence-based approaches are needed to reduce weight regain. This might include:
- getting quality sleep
- exercising in a way that builds and maintains muscle. While on the medication, you will likely have lost muscle as well as fat, although this is not inevitable, especially if you exercise regularly while taking it
Prioritise building and maintaining muscle. EvMedvedeva/Shutterstock - addressing emotional and cultural aspects of life that contribute to over-eating and/or eating unhealthy foods, and how you view your body. Stigma and shame around body shape and size is not cured by taking this medication. Even if you have a healthy relationship with food, we live in a culture that is fat-phobic and discriminates against people in larger bodies
- eating in a healthy way, hopefully continuing with habits that were formed while on the medication. Eating meals that have high nutrition and fibre, for example, and lower overall portion sizes.
Many people will stop taking tirzepatide or semaglutide at some point, given it is expensive and in short supply. When you do, it is important to understand what will happen and what you can do to help avoid the consequences. Regular reviews with your GP are also important.
Read the other articles in The Conversation’s Ozempic series here.
Natasha Yates, General Practitioner, PhD Candidate, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: