The Five Pillars Of Longevity
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Five Pillars Of Longevity

This is Dr. Mark Hyman. He’s a medical doctor, and he’s the board president of clinical affairs of the Institute for Functional Medicine. He’s also the founder and medical director of the UltraWellness Center!
What he’d like you to know about is what he calls the “Five Pillars of Longevity”.
Now, here at 10almonds, we often talk about certain things that science finds to be good for almost any health condition, and have made a habit of referencing what we call “The Usual Five Things™” (not really a trademark, by the way—just a figure of speech), which are:
- Have a good diet
- Get good exercise
- Get good sleep
- Reduce (or eliminate) alcohol consumption
- Don’t smoke
…and when we’re talking about a specific health consideration, we usually provide sources as to why each of them are particularly relevant, and pointers as to the what/how associated with them (ie what diet is good, how to get good sleep, etc).
Dr. Hyman’s “Five Pillars of Longevity” are based on observations from the world’s “Blue Zones”, the popular name for areas with an unusually high concentration of supercentenarians—Sardinia and Okinawa being famous examples, with a particular village in each being especially exemplary.
These Five Pillars of Longevity partially overlap with ours for three out of five, and they are:
- Good nutrition
- Optimized workouts
- Reduce stress
- Get quality sleep
- Find (and live) your purpose
We won’t argue against those! But what does he have to say, for each of them?
Good nutrition
Dr. Hyman advocates for a diet he calls “pegan”, which he considers to combine the paleo and vegan diets. Here at 10almonds, we generally advocate for the Mediterranean Diet because of the mountains of evidence for it, but his approach may be similar in some ways, since it looks to consume a majority plant diet, with some unprocessed meats/fish, limited dairy, and no grains.
By the science, honestly, we stand by the Mediterranean (which includes whole grains), but if for example your body may have issues of some kind with grains, his approach may be a worthy consideration.
Optimized workouts
For Dr. Hyman, this means getting in three kinds of exercise regularly:
- Aerobic/cardio, to look after your heart health
- Resistance training (e.g. weights or bodyweight strength-training) to look after your skeletal and muscular health
- Yoga or similar suppleness training, to look after your joint health
Can’t argue with that, and it can be all too easy to fall into the trap of thinking “I’m healthy because I do x” while forgetting y and/or z! Thus, a three-pronged approach definitely has its merits.
Reduce stress
Acute stress (say, a cold shower) is can confer some health benefits, but chronic stress is ruinous to our health and it ages us. So, reducing this is critical. Dr. Hyman advocates for the practice of mindfulness and meditation, as well as journaling.
Get quality sleep
Quality here, not just quantity. As well as the usual “sleep hygiene” advices, he has some more unorthodox methods, such as the use of binaural beats to increase theta-wave activity in the brain (and thus induce more restful sleep), and the practice of turning off Wi-Fi, on the grounds that Wi-Fi signals interfere with our sleep.
We were curious about these recommendations, so we checked out what the science had to say! Here’s what we found:
- Minimal Effects of Binaural Auditory Beats for Subclinical Insomnia: A Randomized Double-Blind Controlled Study
- Spending the night next to a router – Results from the first human experimental study investigating the impact of Wi-Fi exposure on sleep
In short: probably not too much to worry about in those regards. On the other hand, worrying less, unlike those two things, is a well-established way improve sleep!
(Surprised we disagreed with our featured expert on a piece of advice? Please know: you can always rely on us to stand by what the science says; we pride ourselves on being as reliable as possible!)
Find (and live!) your purpose
This one’s an ikigai thing, to borrow a word from Japanese, or finding one’s raison d’être, as we say in English using French, because English is like that. It’s about having purpose.
Dr. Hyman’s advice here is consistent with what many write on the subject, and it’d be an interesting to have more science on, but meanwhile, it definitely seems consistent with commonalities in the Blue Zone longevity hotspots, where people foster community, have a sense of belonging, know what they are doing for others and keep doing it because they want to, and trying to make the world—or even just their little part of it—better for those who will follow.
Being bitter, resentful, and self-absorbed is not, it seems a path to longevity. But a life of purpose, or even just random acts of kindness, may well be.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cure – by Dr. Jo Marchant

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The subtitle here, “a journey into the science of mind over body”, prompts an immediate question: is this book actually about science?
And yes, yes it is. It’s not about “positive energy” or “tapping into your divine essence” or anysuch. It’s about science, and scientific studies.
The author’s PhD is in genetics and medical microbiology, not metaphysics or something.
For those of us who read a lot of clinical studies about a lot of things (hi, regular researcher/writer here), we’re very used to placebo being used as a control in medical science.
“This drug performed no better than placebo” is generally considered a disappointing statement… But what if the placebo was already having a profound effect? Shouldn’t that be worthy of note too?
Dr. Marchant looks at more than just drugs, though, and also looks into the science (complete with EEGs and such) of hypnosis and virtual reality.
The writing style here is very accessible without skimping on science. This is to be expected; Dr. Marchant also has an MSc in science communication, and spent a time as senior editor of New Scientist magazine.
This isn’t a how-to book, but there are some practical takeaways too, specific things we can do to augment (or avoid sabotaging) any medications we take, for example.
Bottom line: placebo effect (and its evil twin, the nocebo effect) has a profound impact on all of us whether we want it or not, so we might as well learn about how it works and how to leverage it. This book gives a very good, hard science grounding.
Click here to check out “Cure” and get the most out of whatever you take (or do) for your health!
Share This Post
-

Eyes for Alzheimer’s Diagnosis: New?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Time!
This is the bit whereby each week, we respond to subscriber questions/requests/etc
Have something you’d like to ask us, or ask us to look into? Hit reply to any of our emails, or use the feedback widget at the bottom, and a Real Human™ will be glad to read it!
Q: As I am a retired nurse, I am always interested in new medical technology and new ways of diagnosing. I have recently heard of using the eyes to diagnose Alzheimer’s. When I did some research I didn’t find too much. I am thinking the information may be too new or I wasn’t on the right sites.
(this is in response to last week’s piece on lutein, eyes, and brain health)
We’d readily bet that the diagnostic criteria has to do with recording low levels of lutein in the eye (discernible by a visual examination of macular pigment optical density), and relying on the correlation between this and incidence of Alzheimer’s, but we’ve not seen it as a hard diagnostic tool as yet either—we’ll do some digging and let you know what we find! In the meantime, we note that the Journal of Alzheimer’s Disease (which may be of interest to you, if you’re not already subscribed) is onto this:
See also:
- Journal of Alzheimer’s Disease (mixture of free and paid content)
- Journal of Alzheimer’s Disease Reports (open access—all content is free)
Share This Post
-

How often should you really weigh yourself?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Few topics are more debated in health than the value of the humble bathroom scale. Some experts advocate daily self-weigh-ins to promote accountability for weight management, particularly when we’re following a diet and exercise program to lose weight.
Others suggest ditching self-weigh-ins altogether, arguing they can trigger negative psychological responses and unhealthy behaviours when we don’t like, or understand, the number we see on the scale.
Many, like me, recommend using scales to weigh yourself weekly, even when we’re not trying to lose weight. Here’s why.

Diva Plavalaguna/Pexels 1. Weighing weekly helps you manage your weight
Research confirms regular self-weighing is an effective weight loss and management strategy, primarily because it helps increase awareness of our current weight and any changes.
A systematic review of 12 studies found participants who weighed themselves weekly or daily over several months lost 1–3 BMI (body mass index) units more and regained less weight than participants who didn’t weight themselves frequently. The weight-loss benefit was evident with weekly weighing; there was no added benefit with daily weighing.
Weighing regularly means we know when our weight changes. Andres Ayrton/Pexels Self-weigh-ins are an essential tool for weight management as we age. Adults tend to gain weight progressively through middle age. While the average weight gain is typically between 0.5–1kg per year, this modest accumulation of weight can lead to obesity over time. Weekly weighing and keeping track of the results helps avoid unnecessary weight gain.
Tracking our weight can also help identify medical issues early. Dramatic changes in weight can be an early sign of some conditions, including problems with our thyroid, digestion and diabetes.
2. Weekly weighing accounts for normal fluctuations
Our body weight can fluctuate within a single day and across the days of the week. Studies show body weight fluctuates by 0.35% within the week and it’s typically higher after the weekend.
Daily and day-to-day body weight fluctuations have several causes, many linked to our body’s water content. The more common causes include:
The type of food we’ve consumed
When we’ve eaten a dinner higher in carbohydrates, we’ll weigh more the next day. This change is a result of our bodies temporarily carrying more water. We retain 3–4 grams of water per gram of carbohydrate consumed to store the energy we take from carbs.
Our water content also increases when we consume foods higher in salt. Our bodies try to maintain a balance of sodium and water. When the concentration of salt in our bloodstream increases, a mechanism is triggered to restore balance by retaining water to dilute the excess salt.
The morning after a big pasta dinner, we’ll carry more water weight. Dana Tentis/Pexels Our food intake
Whether it’s 30 grams of nuts or 65 grams of lean meat, everything we eat and drink has weight, which increases our body weight temporarily while we digest and metabolise what we’ve consumed.
Our weight also tends to be lower first thing in the morning after our food intake has been restricted overnight and higher in the evening after our daily intake of food and drinks.
Exercise
If we weigh ourselves at the gym after a workout, there’s a good chance we’ll weigh less due to sweat-induced fluid loss. The amount of water lost varies depending on things like our workout intensity and duration, the temperature and humidity, along with our sweat rate and hydration level. On average, we lose 1 litre of sweat during an hour of moderate-intensity exercise.
Hormonal changes
Fluctuations in hormones within your menstrual cycle can also affect fluid balance. Women may experience fluid retention and temporarily gain 0.5–2kg of weight at this time. Specifically, the luteal phase, which represents the second half of a woman’s cycle, results in a shift of fluid from your blood plasma to your cells, and bloating.
Most of our weight fluctuations are water-related. Engin Akyurt/Unsplash Bowel movements
Going to the bathroom can lead to small but immediate weight loss as waste is eliminated from the body. While the amount lost will vary, we generally eliminate around 100 grams of weight through our daily bowel movements.
All of these fluctuations are normal, and they’re not indicative of significant changes in our body fat or muscle mass. However, seeing these fluctuations can lead to unnecessary stress and a fixation with our weight.
3. Weekly weighing avoids scale obsession and weight-loss sabotage
Weighing too frequently can create an obsession with the number on the scales and do more harm than good.
Often, our reaction when we see this number not moving in the direction we want or expect is to further restrict our food intake or embark on fad dieting. Along with not being enjoyable or sustainable, fad diets also ultimately increase our weight gain rather than reversing it.
This was confirmed in a long-term study comparing intentional weight loss among more than 4,000 twins. The researchers found the likelihood of becoming overweight by the age of 25 was significantly greater for a twin who dieted to lose 5kg or more. This suggests frequent dieting makes us more susceptible to weight gain and prone to future weight gain.
So what should you do?
Weighing ourselves weekly gives a more accurate measure of our weight trends over time.
Aim to weigh yourself on the same day, at the same time and in the same environment each week – for example, first thing every Friday morning when you’re getting ready to take a shower, after you’ve gone to the bathroom, but before you’ve drunk or eaten anything.
Weigh yourself at the same time on the same day of the week. Alexanderstock23/Shutterstock Use the best quality scales you can afford. Change the batteries regularly and check their accuracy by using a “known” weight – for example, a 10kg weight plate. Place the “known” weight on the scale and check the measurement aligns with the “known” weight.
Remember, the number on the scale is just one part of health and weight management. Focusing solely on it can overshadow other indicators, such as how your clothes fit. It’s also essential to pay equal attention to how we’re feeling, physically and emotionally.
Stop weighing yourself – at any time interval – if it’s triggering anxiety or stress, and get in touch with a health-care professional to discuss this.
At the Boden Group, Charles Perkins Centre, we are studying the science of obesity and running clinical trials for weight loss. You can register here to express your interest.
Nick Fuller, Charles Perkins Centre Research Program Leader, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post





Related Posts
-

Reduce Your Stroke Risk
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
❝Each year in the U.S., over half a million people have a first stroke; however, up to 80% of strokes may be preventable.❞
~ American Stroke Association
Source: New guideline: Preventing a first stroke may be possible with screening, lifestyle changes
So, what should we do?
Some of the risk factors are unavoidable or not usefully avoidable, like genetic predispositions and old age, respectively (i.e. it is possible to avoid old age—by dying young, which is not a good approach).
Some of the risk factors are avoidable. Let’s look at the most obvious first:
You cannot drink to your good health
While overall, the World Health Organization has declared that “the only safe amount of alcohol is zero”, when it comes to stroke risk specifically, it seems that low consumption is not associated with stroke, while moderate to high consumption is associated with a commensurately increased risk of stroke:
Alcohol Intake as a Risk Factor for Acute Stroke
Note: there are some studies out there that say that a low to moderate consumption may decrease the risk compared to zero consumption. However, any such study that this writer has seen has had the methodological flaw of not addressing why those who do not drink alcohol, do not drink it. In many cases, someone who drinks no alcohol at all does so because either a) it would cause problems with some medication(s) they are taking, or b) they used to drink heavily, and quit. In either case, their reasons for not drinking alcohol may themselves be reasons for an increased stroke risk—not the lack of alcohol itself.
Smoke now = stroke later
This one is straightforward; smoking is bad for pretty much everything, and that includes stroke risk, as it’s bad for your heart and brain both, increasing stroke risk by 200–400%:
Smoking and stroke: the more you smoke the more you stroke
So, the advice here of course is: don’t smoke
Diet matters
The American Stroke Association’s guidelines recommend, just for a change, the Mediterranean Diet. This does not mean just whatever is eaten in the Mediterranean region though, and there are specifically foods that are included and excluded, and the ratios matter, so here’s a run-down of what the Mediterranean Diet does and doesn’t include:
The Mediterranean Diet: What Is It Good For? ← what isn’t it good for?!
You can outrun stroke
Or out-walk it; that’s fine too. Most important here is frequency of exercise, more than intensity. So basically, getting those 150 minutes moderate exercise per week as a minimum.
See also: The Doctor Who Wants Us To Exercise Less & Move More
Which is good, because it means we can get a lot of exercise in that doesn’t feel like “having to do” exercise, for example:
Do You Love To Go To The Gym? No? Enjoy These “No-Exercise Exercises”!
Your brain needs downtime too
Your brain (and your heart) both need you to get good regular sleep:
Sleep Disorders in Stroke: An Update on Management
We sometimes say that “what’s good for your heart is good for your brain” (because the heart feeds the brain, and also ultimately clears away detritus), and that’s true here too, so we might also want to prioritize sleep regularity over other factors, even over duration:
How Regularity Of Sleep Can Be Even More Important Than Duration ← this is about adverse cardiovascular events, including ischemic stroke
Keep on top of your blood pressure
High blood pressure is a very modifiable risk factor for stroke. Taking care of the above things will generally take care of this, especially the DASH variation of the Mediterranean diet:
Hypertension: Factors Far More Relevant Than Salt
However, it’s still important to actually check your blood pressure regularly, because sometimes an unexpected extra factor can pop up for no obvious reason. As a bonus, you can do this improved version of the usual blood pressure test, still using just a blood pressure cuff:
Try This At Home: ABI Test For Clogged Arteries
Consider GLP-1 receptor agonists (or…)
GLP-1 receptor agonists (like Ozempic et al.) seem to have cardioprotective and neuroprotective (thus: anti-stroke) activity independent of their weight loss benefits:
Of course, GLP-1 RAs aren’t everyone’s cup of tea, and they do have their downsides (including availability, cost, and the fact benefits reverse themselves if you stop taking them), so if you want a similar effect from a natural approach, there are some foods that work on the body’s incretin responses in the same way as GLP-1 RAs do:
5 Foods That Naturally Mimic The “Ozempic Effect”
Better to know sooner rather than too late
Rather than waiting until one half of our face is drooping to know that there was a stroke risk, here are things to watch out for to know about it before it’s too late:
6 Signs Of Stroke (One Month In Advance)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Bitter Truth About Coffee (or is it?)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Bitter Truth About Coffee (or is it?)

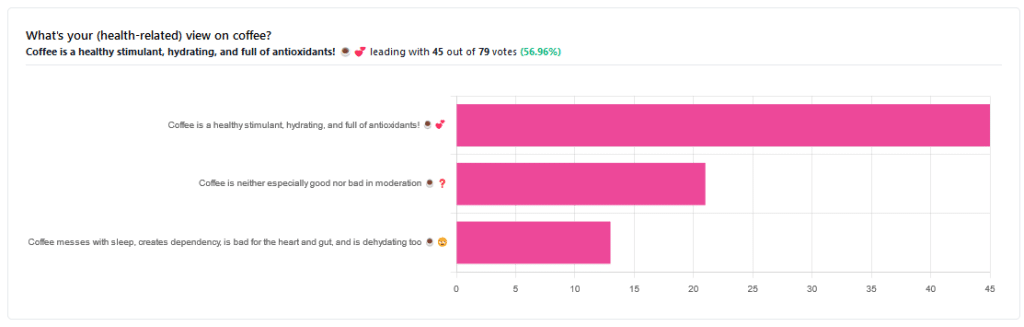
Yesterday, we asked you for your (health-related) views on coffee. The results were clear: if we assume the responses to be representative, we’re a large group of coffee-enthusiasts!
One subscriber who voted for “Coffee is a healthy stimulant, hydrating, and full of antioxidants” wrote:
❝Not so sure about how hydrating it is! Like most food and drink, moderation is key. More than 2 or 3 cups make me buzz! Just too much.❞
And that fine point brings us to our first potential myth:
Coffee is dehydrating: True or False?
False. With caveats…
Coffee, in whatever form we drink it, is wet. This may not come as a startling revelation, but it’s an important starting point. It’s mostly water. Water itself is not dehydrating.
Caffeine, however, is a diuretic—meaning you will tend to pee more. It achieves its diuretic effect by increasing blood flow to your kidneys, which prompts them to release more water through urination.
See: Effect of caffeine on bladder function in patients with overactive bladder symptoms
How much caffeine is required to have a diuretic effect? About 4.5 mg/kg.
What this means in practical terms: if you weigh 70kg (a little over 150lbs), 4.5×70 gives us 315.
315mg is about how much caffeine might be in six shots of espresso. We say “might” because while dosage calculations are an exact science, the actual amount in your shot of espresso can vary depending on many factors, including:
- The kind of coffee bean
- How and when it was roasted
- How and when it was ground
- The water used to make the espresso
- The pressure and temperature of the water
…and that’s all without looking at the most obvious factor: “is the coffee decaffeinated?”
If it doesn’t contain caffeine, it’s not diuretic. Decaffeinated coffee does usually contain tiny amounts of caffeine still, but with nearer 3mg than 300mg, it’s orders of magnitude away from having a diuretic effect.
If it does contain caffeine, then the next question becomes: “and how much water?”
For example, an Americano (espresso, with hot water added to make it a long drink) will be more hydrating than a ristretto (espresso, stopped halfway through pushing, meaning it is shorter and stronger than a normal espresso).
A subscriber who voted for “Coffee messes with sleep, creates dependency, is bad for the heart and gut, and is dehydrating too” wrote:
❝Coffee causes tachycardia for me so staying away is best. People with colon cancer are urged to stay away from coffee completely.❞
These are great points! It brings us to our next potential myth:
Coffee is bad for the heart: True or False?
False… For most people.
Some people, like our subscriber above, have an adverse reaction to caffeine, such as tachycardia. An important reason (beyond basic decency) for anyone providing coffee to honor requests for decaff.
For most people, caffeine is “heart neutral”. It doesn’t provide direct benefits or cause direct harm, provided it is enjoyed in moderation.
See also: Can you overdose on caffeine?
Some quick extra notes…
That’s all we have time for in myth-busting, but it’s worth noting before we close that coffee has a lot of health benefits; we didn’t cover them today because they’re not contentious, but they are interesting nevertheless:
- Coffee is the world’s biggest source of antioxidants
- 65% reduced risk of Alzheimer’s for coffee-drinkers
- 67% reduced risk of type 2 diabetes for coffee-drinkers
- 43% reduced risk of liver cancer for coffee-drinkers
- 53% reduced suicide risk for coffee-drinkers
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

At The Heart Of Women’s Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A woman’s heart is a particular thing
For the longest time (and still to a large degree now), “women’s health” is assumed to refer to the health of organs found under a bikini. But there’s a lot more to it than that. We are whole people, with such things as brains and hearts and more.
Today (Valentine’s Day!) we’re focusing on the heart.
A quick recap:
We’ve talked previously about some of these sex differences when it comes to the heart, for example:
Heart Attack: His & Hers (Be Prepared!)
…but that’s fairly common knowledge at least amongst those who are attentive to such things, whereas…
…is much less common knowledge, especially with the ways statins are more likely to make things worse for a lot of women (not all though; see the article for some nuance about that).
We also talked about:
What Menopause Does To The Heart
…which is well worth reading too!
A question:
Why are women twice as likely to die from a heart attack as their age-equivalent male peers? Women develop heart disease later, but die from it sooner. Why is that?
That’s been a question scientists have been asking (and tentatively answering, as scientists do—hypotheses, theories, conclusions even sometimes) for 20 years now. Likely contributing factors include:
- A lack of public knowledge of the different symptoms
- A lack of confidence of bystanders to perform CPR on a woman
- A lack of public knowledge (including amongst prescribers) about the sex-related differences for statins
- A lack of women in cardiology, comparatively.
- A lack of attention to it, simply. Men get heart disease earlier, so it’s thought of as a “man thing”, by health providers as much as by individuals. Men get more regular cardiovascular check-ups, women get a mammogram and go.
Statistically, women are much more likely to die from heart disease than breast cancer:
- Breast cancer kills around 0.02% of us.
- Heart disease kills one in three.
And yet…
❝In a nationwide survey, only 22% of primary care doctors and 42% of cardiologists said they feel extremely well prepared to assess cardiovascular risks in women.
We are lagging in implementing risk prevention guidelines for women.
A lot of women are being told to just watch their cholesterol levels and see their doctor in a year. That’s a year of delayed care.❞
Source: The slowly evolving truth about heart disease and women
(there’s a lot more in that article than we have room for in ours, so do check it out!)
Some good news:
The “bystanders less likely to feel confident performing CPR on a woman” aspect may be helped by the deployment of new automatic external defibrillator, that works from four sides instead of one.
It’s called “double sequential external defibrillation”, and you can learn about it here:
A new emergency procedure for cardiac arrests aims to save more lives—here’s how it works
(it’s in use already in Canada and Aotearoa)
Gentlemen-readers, thank you for your attention to this one even if it was mostly not about you! Maybe someone you love will benefit from being aware of this
On a lighter note…
Since it’s Valentine’s Day, a little more on affairs of the heart…
Is chocolate good for the heart? And is it really an aphrodisiac?
We answered these questions and more in our previous main feature:
Chocolate & Health: Fact or Fiction?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: