Cranberries vs Goji Berries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing cranberries to goji berries, we picked the cranberries.
Why?
Both are great! And your priorities may differ. Here’s how they stack up:
In terms of macros, goji berries have more protein, carbs, and fiber. This is consistent with them generally being eaten very dried, whereas cranberries are more often eaten fresh or from frozen, or partially rehydrated. In any case, goji berries are the “more food per food” option, so it wins this category. The glycemic indices are both low, by the way, though goji berries are the lower.
When it comes to vitamins, cranberries have more of vitamins B1, B2, B3, B5, B6, B9, E, K, and choline, while goji berries have more of vitamins A and C. Admittedly it’s a lot more, but still, on strength of overall vitamin coverage, the clear winner here is cranberries.
We see a similar story when it comes to minerals: cranberries have more copper, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while goji berries have (a lot) more calcium and iron. Again, by strength of overall mineral coverage, the clear winner here is cranberries.
Cranberries do also have some extra phytochemical benefits, including their prevention/cure status when it comes to UTIs—see our link below for more on that.
At any rate, enjoy either or both, but those are the strengths and weaknesses of these two berries!
Want to learn more?
You might like to read:
- Health Benefits Of Cranberries (But: You’d Better Watch Out)
- Goji Berries: Which Benefits Do They Really Have?
- The Sugary Food That Lowers Blood Sugars ← this is also about goji berries
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Samosa Spiced Surprise

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You know what’s best about samosas? It’s not actually the fried pastry; that’s just what holds it together. If you were to try eating sheets of pastry alone, it would not be much fun. But, the spiced vegetable filling? Now we’re talking! So, this recipe takes what’s best about samosas, and makes them into healthy snack-sized patties.
You will need
- Extra virgin olive oil, or coconut oil (per your preference) for cooking
- 4 medium potatoes, boiled, peeled, and mashed
- 1 medium onion, diced
- 1 cup peas
- 1 carrot, finely chopped
- ½ cup garbanzo bean flour (chickpea flour, gram flour, whatever your supermarket calls it)
- ¼ cup fresh cilantro, chopped (substitute parsley if you have the soap gene)
- ¼ bulb garlic, minced
- 1 jalapeño pepper, chopped
- 1 tbsp ground cumin
- 2 tsp garam masala
- 1 tsp ground coriander
- 1 tsp ground turmeric
- 1 tsp ground black pepper
Method
(we suggest you read everything at least once before doing anything)
1) Fry the onion until it is becoming soft and translucent (3–5 minutes).
2) Add the spices (the garlic, both kinds of pepper, cumin, coriander, turmeric, and the garam masala), stirring in well
3) Add the carrot and peas, stirring and cooking until just becoming soft (probably another 3–5 minutes, depending on the heat, how small you chopped the carrot, and whether the peas were frozen or fresh). Take it off the heat.
4) Mix the potato, chickpea flour, and cilantro in a bowl, and carefully add everything from the pan, mixing that in thoroughly too.
5) Shape into patties, and fry them on each side until browned and crispy.
6) Serve as part of a buffet, or perhaps as an appetizer—raita is a fine accompaniment option.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
Take care!
Share This Post
-

Scheduling Tips for Overrunning Tasks
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Your Questions, Our Answers!
Q: Often I schedule time for things, but the task takes longer than I think, or multiplies while I’m doing it, and then my schedule gets thrown out. Any ideas?
A: A relatable struggle! Happily, there are remedies:
- Does the task really absolutely need to be finished today? If not, just continue it in scheduled timeslots until it’s completed.
- Some tasks do indeed need to be finished today (hi, writer of a daily newsletter here!), so it can be useful to have an idea of how long things really take, in advance. While new tasks can catch us unawares, recurring or similar-to-previous tasks can be estimated based on how long they took previously. For this reason, we recommend doing a time audit every now and again, to see how you really use your time.
- A great resource that you should include in your schedule is a “spare” timeslot, ideally at least one per day. Call it a “buffer” or a “backup” or whatever (in my schedule it’s labelled “discretionary”), but the basic idea is that it’s a scheduled timeslot with nothing scheduled in it, and it works as an “overflow” catch-all.
Additionally:
- You can usually cut down the time it takes you to do tasks by setting “Deep Work” rules for yourself. For example: cut out distractions, single-task, work in for example 25-minute bursts with 5-minute breaks, etc
- You can also usually cut down the time it takes you to do tasks by making sure you’re prepared for them. Not just task-specific preparation, either! A clear head on, plenty of energy, the resources you’ll need (including refreshments!) to hand, etc can make a huge difference to efficiency.
See Also: Time Optimism and the Planning Fallacy
Do you have a question you’d like to see answered here? Hit reply or use the feedback widget at the bottom; we’d love to hear from you!
Share This Post
-

From immunotherapy to mRNA vaccines – the latest science on melanoma treatment explained
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More than 16,000 Australians will be diagnosed with melanoma each year. Most of these will be caught early, and can be cured by surgery.
However, for patients with advanced or metastatic melanoma, which has spread from the skin to other organs, the outlook was bleak until the advent of targeted therapies (that attack specific cancer traits) and immune therapies (that leverage the immune system). Over the past decade, these treatments have seen a significant climb in the number of advanced melanoma patients surviving for at least five years after diagnosis, from less than 10% in 2011 to around 50% in 2021.
While this is great news, there are still many melanoma patients who cannot be treated effectively with current therapies. Researchers have developed two exciting new therapies that are being evaluated in clinical trials for advanced melanoma patients. Both involve the use of immunotherapy at different times and in different ways.
The first results from these trials are now being shared publicly, offering insight into the future of melanoma treatment.
Svitlana Hulko/Shutterstock Immunotherapy before surgery
Immunotherapy works by boosting the power of a patient’s immune system to help kill cancer cells. One type of immunotherapy uses something called “immune checkpoint inhibitors”.
Immune cells carry “immune checkpoint” proteins, which control their activity. Cancer cells can interact with these checkpoints to turn off immune cells and hide from the immune system. Immune checkpoint inhibitors block this interaction and help keep the immune system activated to fight the cancer.
Results from an ongoing phase 3 trial using immune checkpoint inhibitors were recently published in the New England Journal of Medicine.
This trial used two types of immune checkpoint inhibitors: nivolumab, which blocks an immune checkpoint called PD-1, and ipilimumab, which blocks CTLA-4.
More than 16,000 Australians are diagnosed with melanoma each year. Delovely Pics/Shutterstock Some 423 patients (including many from Australia) were enrolled in the trial, and participants were randomly assigned to one of two groups.
The first group had surgery to remove their melanoma, and were then given immunotherapy (nivolumab) to help kill any remaining cancer cells. Giving a systemic (whole body) therapy such as immunotherapy after surgery is a standard way of treating melanoma. The second group received immunotherapy first (nivolumab plus ipilimumab) and then underwent surgery. This is a new approach to treating these cancers.
Based on previous observations, the researchers had predicted that giving patients immunotherapy while the whole tumour was still present would activate the tumour-fighting abilities of the patient’s immune system much better than giving it once the tumour had been removed.
Sure enough, 12 months after starting therapy, 83.7% of patients who received immunotherapy before surgery remained cancer-free, compared to 57.2% in the control group who received immunotherapy after surgery.
Based on these results, Australian of the year Georgina Long – who co-led the trial with Christian Blank from The Netherlands Cancer Institute – has suggested this method of immunotherapy before surgery should be considered a new standard of treatment for higher risk stage 3 melanoma. She also said a similar strategy should be evaluated for other cancers.
The promising results of this phase 3 trial suggest we might see this combination treatment being used in Australian hospitals within the next few years.
mRNA vaccines
Another emerging form of melanoma therapy is the post-surgery combination of a different checkpoint inhibitor (pembrolizumab, which blocks PD-1), with a messenger RNA vaccine (mRNA-4157).
While checkpoint inhibitors like pembrolizumab have been around for more than a decade, mRNA vaccines like mRNA-4157 are a newer phenomenon. You might be familiar with mRNA vaccines though, as the biotechnology companies Pfizer-BioNTech and Moderna released COVID vaccines based on mRNA technology.
mRNA-4157 works basically the same way – the mRNA is injected into the patient and produces antigens, which are small proteins that train the body’s immune system to attack a disease (in this case, cancer, and for COVID, the virus).
However, mRNA-4157 is unique – literally. It’s a type of personalised medicine, where the mRNA is created specifically to match a patient’s cancer. First, the patient’s tumour is genetically sequenced to figure out what antigens will best help the immune system to recognise their cancer. Then a patient-specific version of mRNA-4157 is created that produces those antigens.
The latest results of a three-year, phase 2 clinical trial which combined pembrolizumab and mRNA-4157 were announced this past week. Overall, 2.5 years after starting the trial, 74.8% of patients treated with immunotherapy combined with mRNA-4157 post-surgery remained cancer-free, compared to 55.6% of those treated with immunotherapy alone. These were patients who were suffering from high-risk, late-stage forms of melanoma, who generally have poor outcomes.
It’s worth noting these results have not yet been published in peer-reviewed journals. They’re available as company announcements, and were also presented at some cancer conferences in the United States.
Based on the results of this trial, the combination of pembrolizumab and the vaccine progressed to a phase 3 trial in 2023, with the first patients being enrolled in Australia. But the final results of this trial are not expected until 2029.
It is hoped this mRNA-based anti-cancer vaccine will blaze a trail for vaccines targeting other types of cancer, not just melanoma, particularly in combination with checkpoint inhibitors to help stimulate the immune system.
Despite these ongoing advances in melanoma treatment, the best way to fight cancer is still prevention which, in the case of melanoma, means protecting yourself from UV exposure wherever possible.
Sarah Diepstraten, Senior Research Officer, Blood Cells and Blood Cancer Division, WEHI (Walter and Eliza Hall Institute of Medical Research) and John (Eddie) La Marca, Senior Research Officer, Blood Cells and Blood Cancer, WEHI (Walter and Eliza Hall Institute of Medical Research)
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post




Related Posts
-

Why Psyllium Is Healthy Through-And-Through
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Psyllium is the powder of the husk of the seed of the plant Plantago ovata.
It can be taken as a supplement, and/or used in cooking.
What’s special about it?
It is fibrous, and the fiber is largely soluble fiber. It’s a “bulk-forming laxative”, which means that (dosed correctly) it is good against both constipation (because it’s a laxative) and diarrhea (because it’s bulk-forming).
See also, because this is Research Review Monday and we provide papers for everything:
In other words, it will tend things towards being a 3 or 4 on the Bristol Stool Scale ← this is not pretty, but it is informative.
Before the bowels
Because of how it increases the viscosity of substances it finds itself in, psyllium slows stomach-emptying, and thus improves feelings of satiety.
Here’s a study in which taking psyllium before breakfast and lunch resulted in increased satiety between meals, and reduction in food-related cravings:
Satiety effects of psyllium in healthy volunteers
Prebiotic benefits
We can’t digest psyllium, but our gut bacteria can—somewhat! Because they can only digest some of the psyllium fibers, that means the rest will have the stool-softening effect, while we also get the usual in-gut benefits from prebiotic fiber first too:
The Effect of Psyllium Husk on Intestinal Microbiota in Constipated Patients and Healthy Controls
Cholesterol-binding
Psyllium can bind to cholesterol during the digestive process. Why only “can”? Well, if you don’t consume cholesterol (for example, if you are vegan), then there won’t be cholesterol in the digestive tract to bind to (yes, we do need some cholesterol to live, but like most animals, we can synthesize it ourselves).
What this cholesterol-binding action means is that the dietary cholesterol thus bound cannot enter the bloodstream, and is simply excreted instead:
Heart health beyond cholesterol
Psyllium supplementation can also help lower high blood pressure but does not significantly lower already-healthy blood pressure, so it can be particularly good for keeping things in safe ranges:
❝Given the overarching benefits and lack of reported side effects, particularly for hypertensive patients, health care providers and clinicians should consider the use of psyllium supplementation for the treatment or abatement of hypertension, or hypertensive symptoms.❞
Read in full: The effect of psyllium supplementation on blood pressure: a systematic review and meta-analysis of randomized controlled trials ← you can see the concrete numbers here
Is it safe?
Psyllium is first and foremost a foodstuff, and is considered very safe unless you have an allergy (which is rare, but possible).
However, it is still recommended to start at a low dose and work up, because anything that changes your gut microbiota, even if it changes it for the better, will be easiest if done slowly (or else, you will hear about it from your gut).
Want to try some?
We don’t sell it, but here for your convenience is an example product on Amazon
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

10almonds Tells The Tea…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s Bust Some Myths!
It’s too late after puberty, hormones won’t change xyz
While yes, many adult trans people dearly wish they’d been able to medically transition before going through the “wrong” puberty, the truth is that a lot of changes will still occur later… even to “unchangeable” things like the skeleton.
The body is remaking itself throughout life, and hormones tell it how to do that. Some parts are just quicker or slower than others. Also: the skeleton is pulled-on constantly by our muscles, and in a battle of muscle vs bone, muscle will always win over time.
Examples of this include:
- trans men building bigger bones to support their bigger muscles
- trans women getting smaller, with wider hips and a pelvic tilt
Trans people have sporting advantages
Assuming at least a year’s cross-sex hormonal treatment, there is no useful advantage to being trans when engaging in a sport. There are small advantages and disadvantages (which goes for any person’s body, really). For example:
- Trans women will tend to be taller than cis women on average…
- …but that larger frame is now being powered by smaller muscles, because they shrink much quicker than the skeleton.
- Trans men taking T are the only athletes allowed to take testosterone…
- …but they will still often be smaller than their fellow male competitors, for example.
Read: Do Trans Women Athletes Have Advantages? (A rather balanced expert overview, which does also cover trans men)
There’s a trans population explosion; it’s a social contagion epidemic!

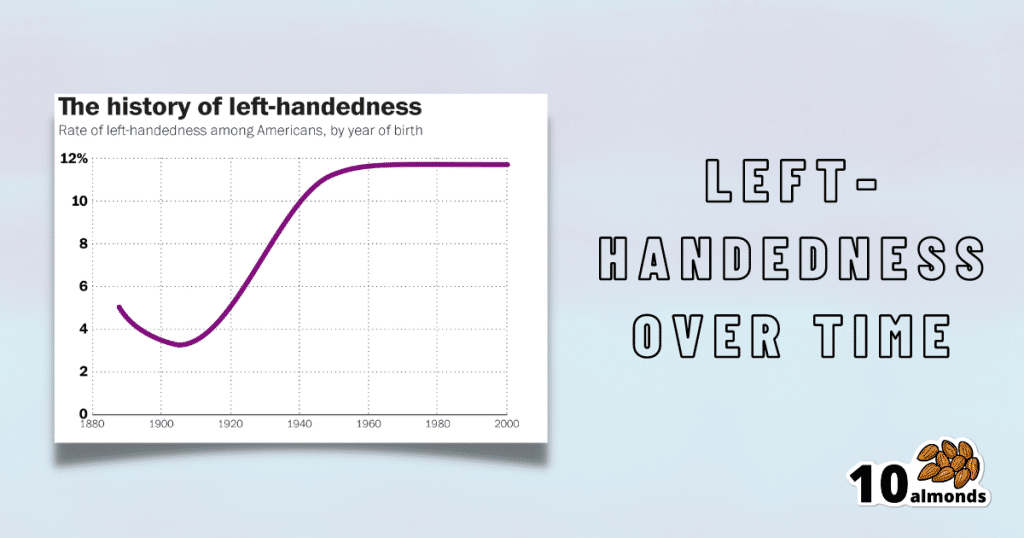
Source for figures: The Overall Rate Of Left-Handedness (Researchgate)
Left-handed people used to make up around 3% of the population… Until the 1920s, when that figure jumped sharply upwards, before plateauing at around 12% in around 1960, where it’s stayed since. What happened?! Simple, schools stopped forcing children to use their right hand.
Today, people ask for trans healthcare because they know it exists! Decades ago, it wasn’t such common knowledge.
The same explanation can be applied to other “population explosions” such as for autism and ADHD.
Fun fact: Mt. Everest was “discovered” in 1852, but scientists suspect it probably existed long before then! People whose ancestors were living on it long before 1852 also agree. Sometimes something exists for a long time, and only comes to wider public awareness later.
Transgender healthcare is too readily available, especially to children!
To believe some press outlets, you’d think:
- HRT is available from school vending machines,
- kids can get a walk-in top surgery at recess,
- and there’s an after-school sterilization club.
In reality, while availability varies from place to place, trans healthcare is heavily gatekept. Even adults have trouble getting it, often having to wait years and/or pay large sums of money… and get permission from a flock of doctors, psychologists, and the like. For those under the age of 18, it’s almost impossible in many places, even with parental support.
Puberty-blockers shouldn’t be given to teenagers, as the effects are irreversible
Quick question: who do you think should be given puberty-blockers? For whom do you think they were developed? Not adults, for sure! They were not developed for trans teens either, but for cis pre-teens with precocious puberty, to keep puberty at bay, to do it correctly later. Nobody argues they’re unsafe for much younger cis children, and only object when it’s trans teens.
They’re not only safe and reversible, but also self-reversing. Stop taking them, and the normally scheduled puberty promptly ensues by itself. For trans kids, the desired effect is to buy the kid time to make an informed and well-considered decision. After all, the effects of the wrong puberty are really difficult to undo!
A lot of people rush medical transition and regret it!
Trans people wish it could be rushed! It’s a lot harder to get gender-affirming care as a trans person, than it is to get the same (or comparable) care as a cis person. Yes, cis people get gender-affirming care, from hormones to surgeries, and have done for a long time.
As for regret… Medical transition has around a 1% regret rate. For comparison, hip replacement has a 4.8% regret rate and knee replacement has a 17.1% regret rate.
A medical procedure with a 99% success rate would generally be considered a miracle cure!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Science-Based Alternative Pain Relief
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Painkillers Aren’t Helping, These Things Might
Maybe you want to avoid painkillers, or maybe you’ve already maxed out what you can have, and want more options as an extra help against the pain.
Today we’ll look at some science-backed alternative pain relief methods:
First: when should we try to relieve pain?
There is no such thing as “this pain is not too much”. The correct amount of pain is zero. Maybe your body won’t let you reach zero, but more than that is “too much” already.
You don’t have to be suffering off the scale to deserve relief from pain!
So: if it hurts, then if you can safely get relief from the pain, it’s already wise to do so.
A couple of things we covered previously
CBD and THC are technically drugs, but are generally considered “alternative” pain relief, so we’ll give a quick mention here:
Short version:
- CBD can treat some kinds of treatment-resistant pain well (others, not so much—try it and find out if it works for you)
- THC can offer some people respite not found from other methods—but beware, because there are many health risks to consider.
Acupuncture
Pain relief appears to be its strongest suit:
Pinpointing The Usefulness Of Acupuncture
Cloves
Yes, just like you can get from the supermarket.
In its medicinal uses, it’s most well-known as a toothache remedy, but it has a local analgesic effect wherever you put it (i.e., apply it topically to where the pain is), thanks to its eugenol content:
Boswellia (frankincense)
The resin of the Boswellia serrata tree, this substance has an assortment of medicinal properties, including pain relief, anti-inflammatory effect, and psychoactive (anxiolytic and antidepressant) effects:
Frankincense is psychoactive: new class of antidepressants might be right under our noses
And as for physical pain? Here’s how it faired against the pain of osteoarthritis (and other OA symptoms, but we’re focusing on pain today), for example:
Here’s an example product on Amazon, but feel free to shop around as there are many options, including for example this handy roll-on
Further reading
Intended for chronic pain, but in large part applicable to acute pain also:
Managing Chronic Pain (Realistically!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: