The 7 Approaches To Pain Management
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
More Than One Way To Kill Pain
This is Dr. Deepak Ravindran (MD, FRCA. FFPMRCA, EDRA. FIPP, DMSMed). He has decades of experience and is a specialist in acute and chronic pain management, anesthesia, musculoskeletal medicine, and lifestyle medicine.
A quick catch-up, first:
We’ve written about chronic pain management before:
Managing Chronic Pain (Realistically!)
As well as:
Science-Based Alternative Pain Relief
Dr. Ravindran’s approach
Dr. Ravindran takes a “trauma-informed care” approach to his professional practice, and recommends the same for others.
In a nutshell, this means starting from a position of not “what’s wrong with you?”, but rather “what happened to you?”.
This seemingly subtle shift is important, because it means actually dealing with a person’s issues, instead of “take one of these and call my secretary next month”. Read more:
Pain itself can be something of a many-headed hydra. Dr. Ravindran’s approach is equally many-headed; specifically, he has a 7-point plan:
Medications
Dr. Ravindran sees painkillers (and a collection of other drugs, like antidepressants and muscle relaxants) as a potential means to an end worth exploring, but he doesn’t expect them to be the best choice for everyone, and nor does he expect them to be a cure-all. Neither should we. He also advises being mindful of the drawbacks and potential complications of these drugs, too.
Interventions
Sometimes, surgery is the right choice. Sometimes it isn’t. Often, it will change a life—one way or the other. Similar to with medications, Dr. Ravindran is very averse to a “one size fits all” approach here. See also:
The Insider’s Guide To Making Hospital As Comfortable As Possible
Neuroscience and stress management
Often a lot of the distress of pain is not just the pain itself, but the fear associated with it. Will it get worse if I move wrong or eat the wrong thing? How long will it last? Will it ever get better? Will it get worse if I do nothing?. Dr. Ravindran advises tackling this, with the same level of importance as the pain itself. Here’s a good start:
Stress, And Building Psychological Resilience
Diet and the microbiome
Many chronic illnesses are heavily influenced by this, and Dr. Ravindran’s respect for lifestyle medicine comes into play here. While diet might not fix all our ills, it certainly can stop things from being a lot worse. Beyond the obvious “eat healthily” (Mediterranean diet being a good starting point for most people), he also advises doing elimination tests where appropriate, to screen out potential flare-up triggers. You also might consider:
Four Ways To Upgrade The Mediterranean Diet
Sleep
“Get good sleep” is easy advice for those who are not in agonizing pain that sometimes gets worse from staying in the same position for too long. Nevertheless, it is important, and foundational to good health. So it’s important to explore—whatever limitations one might realistically have—what can be done to improve it.
If you can only sleep for a short while at a time, you may get benefit from this previous main feature of ours:
How To Nap Like A Pro (No More “Sleep Hangovers”!)
Exercise and movement
The trick here is to move little and often; without overdoing it, but without permitting loss of mobility either. See also:
The Doctor Who Wants Us To Exercise Less, And Move More
Therapies of the mind and body
This is about taking a holistic approach to one’s wellness. In Dr. Ravindran’s words:
❝Mind-body therapies are often an extremely sensitive topic about which people hold very strong opinions and sometimes irrational beliefs.
Some, like reiki and spiritual therapy and homeopathy, have hardly any scientific evidence to back them up, while others like yoga, hypnosis, and meditation/mindfulness are mainstream techniques with many studies showing the benefits, but they all work for certain patients.❞
In other words: evidence-based is surely the best starting point, but if you feel inclined to try something else and it works for you, then it works for you. And that’s a win.
Want to know more?
You might like his book…
The Pain-Free Mindset: 7 Steps to Taking Control and Overcoming Chronic Pain
He also has a blog and a podcast.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Statins and Brain Fog?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I was wondering if you had done any info about statins. I’ve tried 3, and keep quitting them because they give me brain fog. Am I imagining this as the research suggests?❞
If you are female, the chances of adverse side-effects are a lot higher:
As an extra kicker, not only are the adverse side-effects more likely for women, but also, the benefits are often less beneficial, too (see the above main feature for some details).
That’s not to say that statins can’t have their place for women; sometimes it will still be the right choice. Just, not as readily so as for men.
Enjoy!
Share This Post
-

Statistical Models vs. Front-Line Workers: Who Knows Best How to Spend Opioid Settlement Cash?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
MOBILE, Ala. — In this Gulf Coast city, addiction medicine doctor Stephen Loyd announced at a January event what he called “a game-changer” for state and local governments spending billions of dollars in opioid settlement funds.
The money, which comes from companies accused of aggressively marketing and distributing prescription painkillers, is meant to tackle the addiction crisis.
But “how do you know that the money you’re spending is going to get you the result that you need?” asked Loyd, who was once hooked on prescription opioids himself and has become a nationally known figure since Michael Keaton played a character partially based on him in the Hulu series “Dopesick.”
Loyd provided an answer: Use statistical modeling and artificial intelligence to simulate the opioid crisis, predict which programs will save the most lives, and help local officials decide the best use of settlement dollars.
Loyd serves as the unpaid co-chair of the Helios Alliance, a group that hosted the event and is seeking $1.5 million to create such a simulation for Alabama.
The state is set to receive more than $500 million from opioid settlements over nearly two decades. It announced $8.5 million in grants to various community groups in early February.
Loyd’s audience that gray January morning included big players in Mobile, many of whom have known one another since their school days: the speaker pro tempore of Alabama’s legislature, representatives from the city and the local sheriff’s office, leaders from the nearby Poarch Band of Creek Indians, and dozens of addiction treatment providers and advocates for preventing youth addiction.
Many of them were excited by the proposal, saying this type of data and statistics-driven approach could reduce personal and political biases and ensure settlement dollars are directed efficiently over the next decade.
But some advocates and treatment providers say they don’t need a simulation to tell them where the needs are. They see it daily, when they try — and often fail — to get people medications, housing, and other basic services. They worry allocating $1.5 million for Helios prioritizes Big Tech promises for future success while shortchanging the urgent needs of people on the front lines today.
“Data does not save lives. Numbers on a computer do not save lives,” said Lisa Teggart, who is in recovery and runs two sober living homes in Mobile. “I’m a person in the trenches,” she said after attending the Helios event. “We don’t have a clean-needle program. We don’t have enough treatment. … And it’s like, when is the money going to get to them?”
The debate over whether to invest in technology or boots on the ground is likely to reverberate widely, as the Helios Alliance is in discussions to build similar models for other states, including West Virginia and Tennessee, where Loyd lives and leads the Opioid Abatement Council.
New Predictive Promise?
The Helios Alliance comprises nine nonprofit and for-profit organizations, with missions ranging from addiction treatment and mathematical modeling to artificial intelligence and marketing. As of mid-February, the alliance had received $750,000 to build its model for Alabama.
The largest chunk — $500,000 — came from the Poarch Band of Creek Indians, whose tribal council voted unanimously to spend most of its opioid settlement dollars to date on the Helios initiative. A state agency chipped in an additional $250,000. Ten Alabama cities and some private foundations are considering investing as well.
Stephen McNair, director of external affairs for Mobile, said the city has an obligation to use its settlement funds “in a way that is going to do the most good.” He hopes Helios will indicate how to do that, “instead of simply guessing.”
Rayford Etherton, a former attorney and consultant from Mobile who created the Helios Alliance, said he is confident his team can “predict the likely success or failure of programs before a dollar is spent.”
The Helios website features a similarly bold tagline: “Going Beyond Results to Predict Them.”
To do this, the alliance uses system dynamics, a mathematical modeling technique developed at the Massachusetts Institute of Technology in the 1950s. The Helios model takes in local and national data about addiction services and the drug supply. Then it simulates the effects different policies or spending decisions can have on overdose deaths and addiction rates. New data can be added regularly and new simulations run anytime. The alliance uses that information to produce reports and recommendations.
Etherton said it can help officials compare the impact of various approaches and identify unintended consequences. For example, would it save more lives to invest in housing or treatment? Will increasing police seizures of fentanyl decrease the number of people using it or will people switch to different substances?
And yet, Etherton cautioned, the model is “not a crystal ball.” Data is often incomplete, and the real world can throw curveballs.
Another limitation is that while Helios can suggest general strategies that might be most fruitful, it typically can’t predict, for instance, which of two rehab centers will be more effective. That decision would ultimately come down to individuals in charge of awarding contracts.
Mathematical Models vs. On-the-Ground Experts
To some people, what Helios is proposing sounds similar to a cheaper approach that 39 states — including Alabama — already have in place: opioid settlement councils that provide insights on how to best use the money. These are groups of people with expertise ranging from addiction medicine and law enforcement to social services and personal experience using drugs.
Even in places without formal councils, treatment providers and recovery advocates say they can perform a similar function. Half a dozen advocates in Mobile told KFF Health News the city’s top need is low-cost housing for people who want to stop using drugs.
“I wonder how much the results” from the Helios model “are going to look like what people on the ground doing this work have been saying for years,” said Chance Shaw, director of prevention for AIDS Alabama South and a person in recovery from opioid use disorder.
But Loyd, the co-chair of the Helios board, sees the simulation platform as augmenting the work of opioid settlement councils, like the one he leads in Tennessee.
Members of his council have been trying to decide how much money to invest in prevention efforts versus treatment, “but we just kind of look at it, and we guessed,” he said — the way it’s been done for decades. “I want to know specifically where to put the money and what I can expect from outcomes.”
Jagpreet Chhatwal, an expert in mathematical modeling who directs the Institute for Technology Assessment at Massachusetts General Hospital, said models can reduce the risk of individual biases and blind spots shaping decisions.
If the inputs and assumptions used to build the model are transparent, there’s an opportunity to instill greater trust in the distribution of this money, said Chhatwal, who is not affiliated with Helios. Yet if the model is proprietary — as Helios’ marketing materials suggest its product will be — that could erode public trust, he said.
Etherton, of the Helios Alliance, told KFF Health News, “Everything we do will be available publicly for anyone who wants to look at it.”
Urgent Needs vs. Long-Term Goals
Helios’ pitch sounds simple: a small upfront cost to ensure sound future decision-making. “Spend 5% so you get the biggest impact with the other 95%,” Etherton said.
To some people working in treatment and recovery, however, the upfront cost represents not just dollars, but opportunities lost for immediate help, be it someone who couldn’t find an open bed or get a ride to the pharmacy.
“The urgency of being able to address those individual needs is vital,” said Pamela Sagness, executive director of the North Dakota Behavioral Health Division.
Her department recently awarded $7 million in opioid settlement funds to programs that provide mental health and addiction treatment, housing, and syringe service programs because that’s what residents have been demanding, she said. An additional $52 million in grant requests — including an application from the Helios Alliance — went unfunded.
Back in Mobile, advocates say they see the need for investment in direct services daily. More than 1,000 people visit the office of the nonprofit People Engaged in Recovery each month for recovery meetings, social events, and help connecting to social services. Yet the facility can’t afford to stock naloxone, a medication that can rapidly reverse overdoses.
At the two recovery homes that Mobile resident Teggart runs, people can live in a drug-free space at a low cost. She manages 18 beds but said there’s enough demand to fill 100.
Hannah Seale felt lucky to land one of those spots after leaving Mobile County jail last November.
“All I had with me was one bag of clothes and some laundry detergent and one pair of shoes,” Seale said.
Since arriving, she’s gotten her driver’s license, applied for food stamps, and attended intensive treatment. In late January, she was working two jobs and reconnecting with her 4- and 7-year-old daughters.
After 17 years of drug use, the recovery home “is the one that’s worked for me,” she said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

Fight Inflammation & Protect Your Brain, With Quercetin
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Querying Quercetin
Quercetin is a flavonoid (and thus, antioxidant) pigment found in many plants. Capers, radishes, and coriander/cilantro score highly, but the list is large:
USDA Database for the Flavonoid Content of Selected Foods
Indeed,
❝Their regular consumption is associated with reduced risk of a number of chronic diseases, including cancer, cardiovascular disease (CVD) and neurodegenerative disorders❞
~ Dr. Aleksandra Kozłpwsla & Dr. Dorota Szostak-Wegierek
Read more: Flavonoids—food sources and health benefits
For this reason, quercetin is often sold/consumed as a supplement on the strength of its health-giving properties.
But what does the science say?
Quercetin and inflammation
In short, it helps:
❝500 mg per day quercetin supplementation for 8 weeks resulted in significant improvements in clinical symptoms, disease activity, hs-TNFα, and Health Assessment Questionnaire scores in women with rheumatoid athritis❞
Quercetin and blood pressure
It works, if antihypertensive (i.e., blood pressure lowering) effect is what you want/need:
❝…significant effect of quercetin supplementation in the reduction of BP, possibly limited to, or greater with dosages of >500 mg/day.❞
~ Dr. Maria-Corina Serban et al.
Quercetin and diabetes
We’re less confident to claim this one, because (almost?) all of the research so far as been in non-human animals or in vitro. As one team of researchers put it:
❝Despite the wealth of in animal research results suggesting the anti-diabetic and its complications potential of quercetin, its efficacy in diabetic human subjects is yet to be explored❞
Quercetin and neuroprotection
Research has been done into the effect of quercetin on the risk of Parkinson’s disease and Alzheimer’s disease, and they found…
❝The data indicate that quercetin is the major neuroprotective component in coffee against Parkinson’s disease and Alzheimer’s disease❞
Read more: Quercetin, not caffeine, is a major neuroprotective component in coffee
Summary
Quercetin is a wonderful flavonoid that can be enjoyed as part of one’s diet and by supplementation. In terms of its popular health claims:
- It has been found very effective for lowering inflammation
- It has a moderate blood pressure lowering effect
- It may have anti-diabetes potential, but the science is young
- It has been found to have a potent neuroprotective effect
Want to get some?
We don’t sell it, but for your convenience, here’s an example product on Amazon
Enjoy!
Share This Post


Related Posts
-

The Vitamin Solution – by Dr. Romy Block & Dr. Arielle Levitan
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A quick note: it would be remiss of us not to mention that the authors of this book are also the founders of a vitamin company, thus presenting a potential conflict of interest.
That said… In this reviewer’s opinion, the book does seem balanced and objective, regardless.
We talk a lot about supplements here at 10almonds, especially in our Monday Research Review editions. And yesterday, we featured a book by a doctor who hates supplements. Today, we feature a book by two doctors who have made them their business.
The authors cover all the most common vitamins and minerals popularly enjoyed as supplements, and examine:
- why people take them
- factors affecting whether they help
- problems that can arise
- complicating factors
The “complicating factors” include, for example, the way many vitamins and/or minerals interplay with each other, either by requiring the presence of another, or else competing for resources for absorption, or needing to be delicately balanced on pain of diverse woes.
This is the greatest value of the book, perhaps; it’s where most people go wrong with supplementation, if they go wrong.
While both authors are medical doctors, Dr. Romy Block is an endocrinologist specifically, and she clearly brought a lot of extra attention to relevant metabolic/thyroid issues, and how vitamins and minerals (such as thiamin and iron) can improve or sabotage such, depending on various factors that she explains. Informative, and so far as this reviewer could see, objective and well-balanced.
Bottom line: supplementation is a vast and complex topic, but this book does a fine job of demystifying and simplifying it in a clear and objective fashion, without resorting to either scaremongering or hype.
Click here to check out The Vitamin Solution, and upgrade your knowledge!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Oral vaccines could provide relief for people who suffer regular UTIs. Here’s how they work
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In a recent TikTok video, Australian media personality Abbie Chatfield shared she was starting a vaccine to protect against urinary tract infections (UTIs).
Huge news for the UTI girlies. I am starting a UTI vaccine tonight for the first time.
Chatfield suffers from recurrent UTIs and has turned to the Uromune vaccine, an emerging option for those seeking relief beyond antibiotics.
But Uromune is not a traditional vaccine injected to your arm. So what is it and how does it work?

9nong/Shutterstock First, what are UTIs?
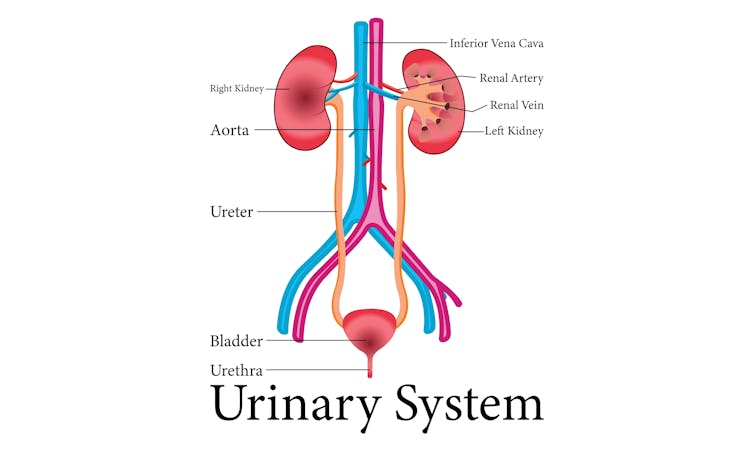
UTIs are caused by bacteria entering the urinary system. This system includes the kidneys, bladder, ureters (thin tubes connecting the kidneys to the bladder), and the urethra (the tube through which urine leaves the body).
The most common culprit is Escherichia coli (E. coli), a type of bacteria normally found in the intestines.
While most types of E. coli are harmless in the gut, it can cause infection if it enters the urinary tract. UTIs are particularly prevalent in women due to their shorter urethras, which make it easier for bacteria to reach the bladder.
Roughly 50% of women will experience at least one UTI in their lifetime, and up to half of those will have a recurrence within six months.
UTIs are caused by bacteria enterning the urinary system. oxo7051/Shutterstock The symptoms of a UTI typically include a burning sensation when you wee, frequent urges to go even when the bladder is empty, cloudy or strong-smelling urine, and pain or discomfort in the lower abdomen or back. If left untreated, a UTI can escalate into a kidney infection, which can require more intensive treatment.
While antibiotics are the go-to treatment for UTIs, the rise of antibiotic resistance and the fact many people experience frequent reinfections has sparked more interest in preventive options, including vaccines.
What is Uromune?
Uromune is a bit different to traditional vaccines that are injected into the muscle. It’s a sublingual spray, which means you spray it under your tongue. Uromune is generally used daily for three months.
It contains inactivated forms of four bacteria that are responsible for most UTIs, including E. coli. By introducing these bacteria in a controlled way, it helps your immune system learn to recognise and fight them off before they cause an infection. It can be classified as an immunotherapy.
A recent study involving 1,104 women found the Uromune vaccine was 91.7% effective at reducing recurrent UTIs after three months, with effectiveness dropping to 57.6% after 12 months.
These results suggest Uromune could provide significant (though time-limited) relief for women dealing with frequent UTIs, however peer-reviewed research remains limited.
Any side effects of Uromune are usually mild and may include dry mouth, slight stomach discomfort, and nausea. These side effects typically go away on their own and very few people stop treatment because of them. In rare cases, some people may experience an allergic reaction.
How can I access it?
In Australia, Uromune has not received full approval from the Therapeutic Goods Administration (TGA), and so it’s not something you can just go and pick up from the pharmacy.
However, Uromune can be accessed via the TGA’s Special Access Scheme or the Authorised Prescriber pathway. This means a GP or specialist can apply for approval to prescribe Uromune for patients with recurrent UTIs. Once the patient has a form from their doctor documenting this approval, they can order the vaccine directly from the manufacturer.
Antibiotics are the go-to treatment for UTIs – but scientists are looking at options to prevent them in the first place. Photoroyalty/Shutterstock Uromune is not covered under the Pharmaceutical Benefits Scheme, meaning patients must cover the full cost out-of-pocket. The cost of a treatment program is around A$320.
Uromune is similarly available through special access programs in places like the United Kingdom and Europe.
Other options in the pipeline
In addition to Uromune, scientists are exploring other promising UTI vaccines.
Uro-Vaxom is an established immunomodulator, a substance that helps regulate or modify the immune system’s response to bacteria. It’s derived from E. coli proteins and has shown success in reducing UTI recurrences in several studies. Uro-Vaxom is typically prescribed as a daily oral capsule taken for 90 days.
FimCH, another vaccine in development, targets something called the adhesin protein that helps E. coli attach to urinary tract cells. FimCH is typically administered through an injection and early clinical trials have shown promising results.
Meanwhile, StroVac, which is already approved in Germany, contains inactivated strains of bacteria such as E. coli and provides protection for up to 12 months, requiring a booster dose after that. This injection works by stimulating the immune system in the bladder, offering temporary protection against recurrent infections.
These vaccines show promise, but challenges like achieving long-term immunity remain. Research is ongoing to improve these options.
No magic bullet, but there’s reason for optimism
While vaccines such as Uromune may not be an accessible or perfect solution for everyone, they offer real hope for people tired of recurring UTIs and endless rounds of antibiotics.
Although the road to long-term relief might still be a bit bumpy, it’s exciting to see innovative treatments like these giving people more options to take control of their health.
Iris Lim, Assistant Professor in Biomedical Science, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Collagen Cure – by Dr. James DiNicolantonio
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Collagen is vital for, well, most of our bodies, really. Where me most tend to feel its deficiency is in our joints and skin, but it’s critical for bones and many other tissues too.
You may be wondering: why a 572-page book to say what surely must amount to “take collagen, duh”?
Dr. DiNicolantonio has a lot more of value to offer us than that. In this book, we learn about not just collagen synthesis and usage, different types of collagen, the metabolism of it in our diet (if we get it—vegans and vegetarians won’t). We also learn about the building blocks of collagen (vegans and vegetarians do get these, assuming a healthy balanced diet), with a special focus on glycine, the smallest amino acid which makes up about a third of the mass of collagen (a protein).
Not stopping there, we also learn about the interplay of other nutrients with our metabolism of glycine and, if applicable, collagen. Vitamin C and copper are star features, but there’s a lot more going on with other nutrients too, down to the level of “So take this 75 minutes before this but after that and/but definitely not with the other”, etc.
The style is incredibly clear and readable for something that’s also quite scientifically dense (over 1000 references and many diagrams).
Bottom line: if you’re serious about maintaining your body as you get older, and you’d like a book about collagen that’s a lot more helpful than “take collagen, duh”, then this is the book for you.
Click here to check out The Collagen Cure, and take care of yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: